Article Text

Statistics from Altmetric.com
A 79-year-old male with a history of mechanical aortic valve replacement and concomitant saphenous vein grafting (SVG) to the left anterior descending (LAD) artery and right coronary artery (RCA) 23 years earlier, was investigated for exertional angina and a new continuous murmur.
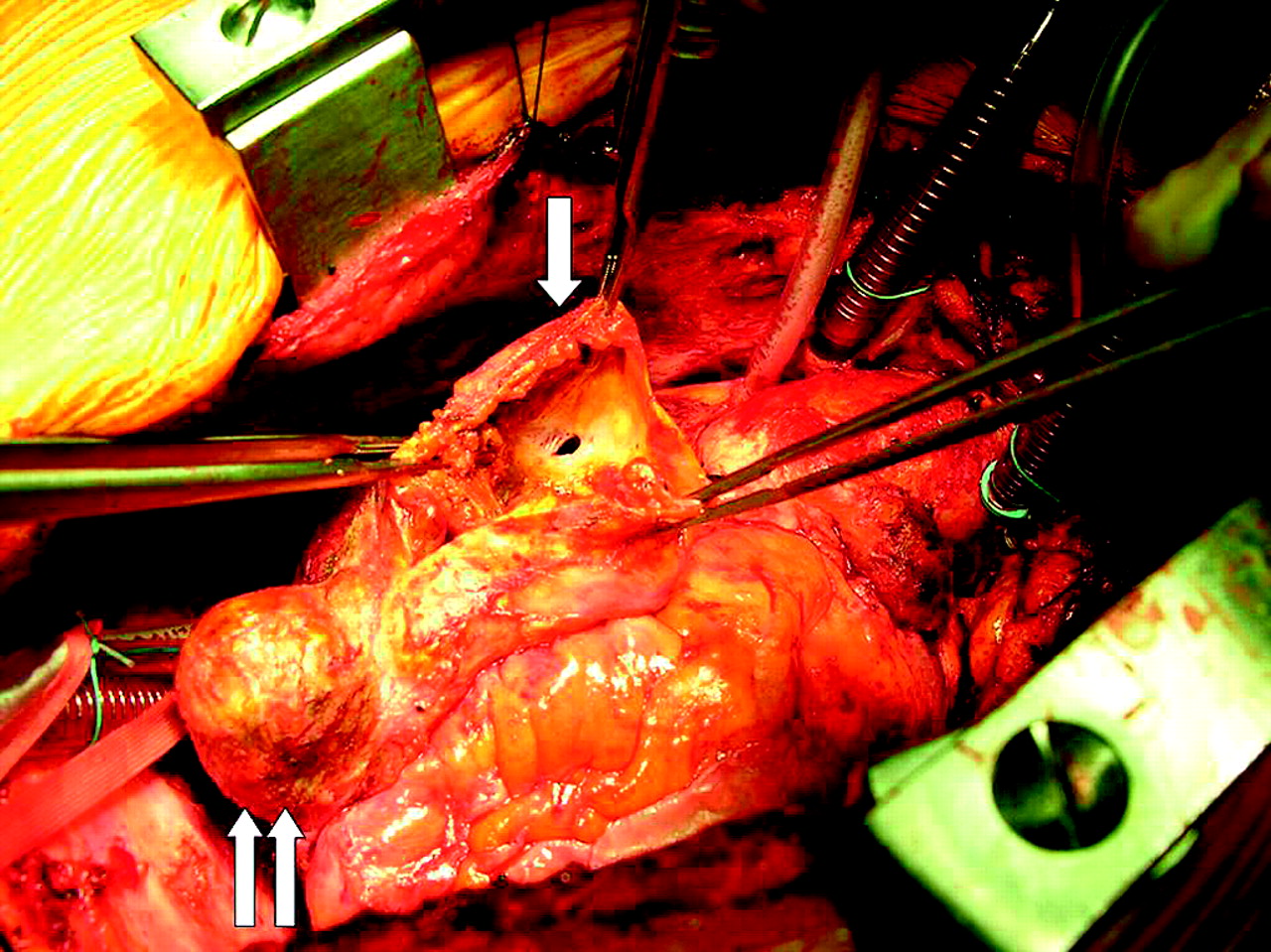
Three-hundred-and-twenty-slice dynamic volume computed tomography (CT) (figure 1, online video 1) demonstrated aneurysmal dilatation of the RCA SVG with a patent distal RCA beyond the anastomosis. An RCA SVG to right atrial fistula with continuous flow throughout systole and diastole was clearly identified, which was not seen on echocardiography and invasive angiography. He underwent successful surgical revascularisation of RCA and closure of the fistula (figure 2) with no audible murmur postoperatively and symptomatic improvement at 5 months' follow-up.
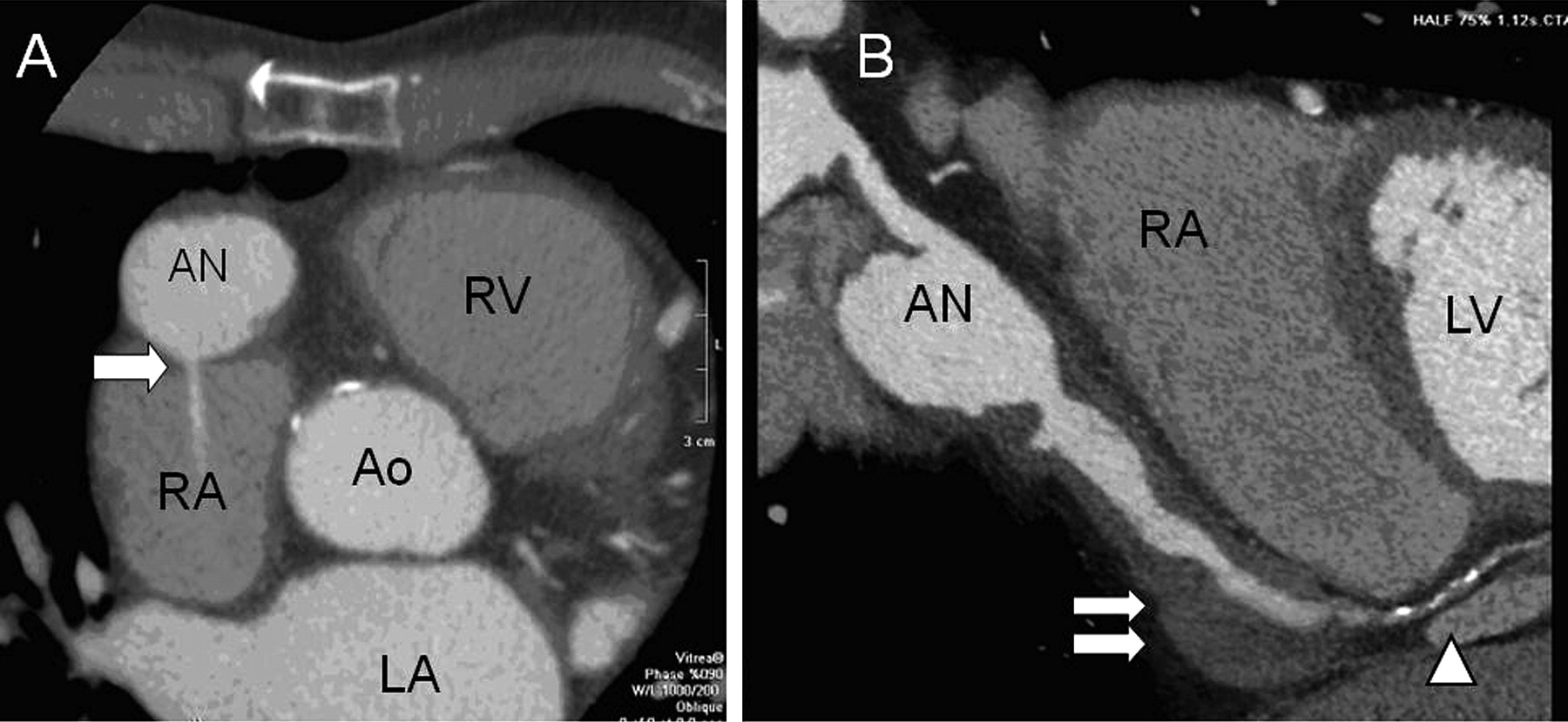
Coronary computed tomography (CT): transverse axial (A) and saggital curved (B) images of right coronary artery vein graft aneurysm. CT clearly identified the vein graft to the right atrial fistula (single arrow) and demonstrated the extent of mural thrombi in the distal portion of the aneurysm (double arrows) and the distal right coronary artery beyond the anastomosis (arrowhead). AN, aneurysm; Ao, aorta; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle.

{kind=link}
{kind=link}
Right coronary artery saphenous vein grafting aneurysm to right atrial fistula demonstrated introperatively. The proximal portion of the aneurysm had been opened to reveal the fistula (single arrow). The distal portion of the graft was also aneurysmal (double arrows), which was not appreciated on the luminogram on invasive coronary angiography.
While surgery is often chosen to revascularise the distal vessel and to reduce the risks of aneurysmal rupture and or heart failure due to fistulous shunting,1 there are reported cases of successful percutaneous coil embolisation.2 In this patient, CT demonstrated a suitable distal vessel for grafting and localised the fistula in a wide portion of the aneurysm, which is a contraindication for coiling.
Accurate diagnosis and localisation of the SVG related fistula can be challenging. This case illustrates the additional value of CT above conventional imaging modalities to aid in both the diagnosis and management of patients with SVG aneurysms and suspected fistulous communication.
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; not externally peer reviewed.