Article Text

Abstract
Cardiovascular diseases (CVDs) have now been finally recognised as a major public health issue in Nepal. This small landlocked South Asian country has an abundance of harmful risk factors that lead to CVD and the country lacks a system to maintain cardiovascular health. Recent national and international attention on CVDs led to the formulation of a non-communicable diseases policy draft, which is yet to be endorsed by the government. This paper describes the present situation of CVDs in Nepal, with a focus on coronary heart disease and its risk factors (epidemiology), ongoing global and national strategies pertaining to the country (strategies), and the work that needs attention to implement the strategies (implementation).
- Hypertension
- lipids
Statistics from Altmetric.com
Introduction
Nepal is a small country of about 30 million people with vast ethnic diversity that is situated between India and China in South Asia. Like many low- and middle-income countries (LMICs), Nepal is battling a double burden of disease, communicable and non-communicable diseases (NCDs), with cardiovascular diseases (CVDs) being the most common among the latter. Research work done particularly in the last decade has shown that the conventional risk factors are present in a high proportion in the Nepalese population.1 There is still much to be done in the areas of communicable and infectious diseases, maternal and child healthcare, and childhood malnutrition. Nepal has to tackle, with its limited economy and resources, the increasing problem of NCDs including CVDs. The silver lining in the midst of these problems has been the formulation of an NCD policy draft2 that can potentially be a roadmap towards the control of CVDs and other NCDs in the country.
Epidemiology: situational analysis of CVDs in Nepal
Apparently, cases of NCDs in Nepal began to be noticed only in the second half of the 20th century. CVD was first documented in the 1970s with cases of myocardial infarction3 followed by occasional publications on risk factors such as hypertension and smoking in the different Nepalese and Indian journals.4–7 The last decade has seen more publications of CVD studies, including reports of hospital audits on CVDs, biochemical studies on blood sugar and lipids, and a few more on interventional cardiology as well.8–11
As there is an absence of a routine surveillance or registry system, the actual burden and trend of CVDs in Nepal is unknown. But combined data from various sources do indicate that the problem is common, and for many CVDs, particularly coronary heart disease (CHD) and its risk factors, it is perhaps increasing too. For instance, a study done in the eastern Nepalese town of Dharan found an approximately 6% prevalence of CHD in male subjects.12 In the Gangalal National Heart Centre, the main referral cardiac hospital in the capital Kathmandu, the number of patients doubled annually between 2001 and 2008.13 Even in a general central hospital such as Tribhuvan University Teaching Hospital, 20% of the admitted patients had CVDs, 8% of whom had CHD.14 Outside the capital, the Nepalgunj Teaching Hospital, which caters to the remote hilly districts of western Nepal, receives 20–40 CVD patients daily.15 Thus, it is not surprising that a recent hospital-based prevalence study of NCDs in 31 hospitals across the country found that 36.5% of the admissions were for NCDs, of which CVDs were the most common (38% among NCDs).16
Besides CHD, there are some data available for other CVDs as well. The Gangalal National Heart Centre reports that after CHD, which is the most common cause of admission (37–43%), rheumatic heart diseases (RHDs) (20–28%), hypertensive heart diseases (7–9%), arrhythmias (4–11%), congenital heart diseases (4–7%) and infective endocarditis (0.5–2.5%) are the other common cardiac ailments presenting to the centre.13 Population-based studies have indicated that RHD has a prevalence of 1.2 per 1000 school children in the capital Kathmandu17 and 1.35 per 1000 in rural children.18 RHD is also the second most common reason, after congenital heart diseases, for open heart surgery in children. The latter have been reported to be frequent in different hospital audits, with one of them reporting it to be present in 5.8 per 1000 paediatric admissions in an eastern Nepal hospital19; another audit from western Nepal reported that half of the paediatric heart patients (n=187) suffered from congenital cardiac ailments.20
In 2001–2003, Nepal contributed 244 cases and 239 controls to the global multicentre case–control INTERHEART study.21 As in other participating countries, the following nine factors were found to be important in Nepal too: abnormal lipids, smoking, hypertension, diabetes, abdominal obesity, psychosocial factors, consumption of fruits and vegetables, alcohol consumption and physical inactivity. Many of these factors were eventually frequently identified as major risk factors by the nationwide 2007 NCD Risk Factor Survey and other smaller studies (figure 1).1 3–9 12 22 Furthermore, metabolic syndrome has also been recently reported to have a prevalence of 1 in 5 in the Nepalese population.23 Besides, an increased trend has also been observed for at least some of these risk factors like obesity and hypertension (figure 2).1 24 25 It has been estimated that the prevalence of tobacco consumption in adults will double from 12% in 1995 to 25% in 2025 and rise to a staggering 40% by 2050.26 At this point, there are no comparable temporal studies to indicate whether diabetes mellitus and dyslipidaemia are on the rise, as the studies are limited and they too are methodologically unrepresentative of the general population. For example, a poorly selected sample leading to a possible overestimation of diabetes (19%) and impaired glucose tolerance (10.6%) has been reported for urban Kathmandu.27 A high prevalence of dyslipidaemia, as reported in another study from the capital, is also likely to be an overestimation as the sample consisted of people coming to cardiac health camps.9
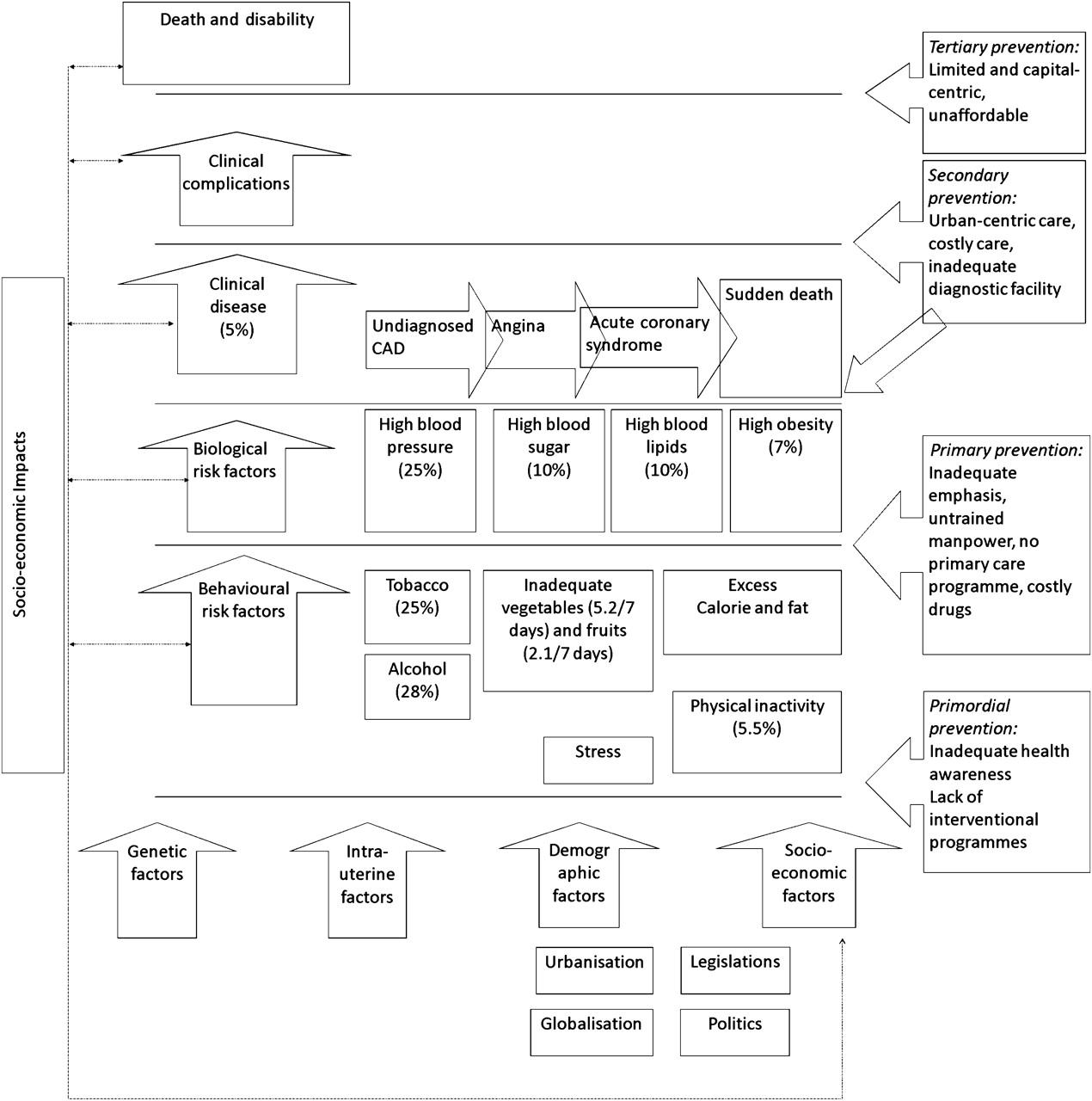
An overview of the risk factors for cardiovascular diseases in the Nepalese context, including the vicious cycle of socio-economic impacts and major hindrances at different levels of prevention. Note: The figures in parentheses are approximate figures for Nepal based on different national or subnational studies carried out in the period 2003–2007.1 3–9 12 22

{kind=link}
{kind=link}
It can be said that because Nepal has similar socio-demographic characteristics to other South Asian countries and has undergone phenomena such as urbanisation and globalisation as in other South Asian countries, particularly India, the increasing trends in CVDs being witnessed in India28 might well be taking place here as well. Besides, it must be noted that international migration studies on CVDs involving people of South Asian origin29 30 have so far not recruited those migrating from Nepal, although the number of people who migrate from Nepal to Europe, the Americas and Australia is also substantial.
Strategies: national and international activities towards tackling CVDs
Currently, Nepal is yet to implement health policies to tackle CVDs or other NCDs. Infectious diseases, maternal and child health and malnutrition deservedly receive the attention of the government and external development partners—more so after the endorsement of the millennium development goals (MDGs).
Management of CVDs in Nepal has characteristically been focused on treatment rather than education and preventive healthcare. There has been a dramatic rise in the availability of interventional cardiology and cardiothoracic surgery services. Although these services are essential to save the lives of those who are already diseased, they have not helped to slow down the growing epidemic of CVDs in the country. The increasing annual numbers of hospital admissions with CVDs also suggest the same.13 It may be added that there are about 80 registered cardiologists in Nepal: 90% of them in Kathmandu. But the majority of the country comprises villages and healthcare in these remote areas is provided mainly by auxiliary health staff who do not have the training needed to deal with CVDs in the primary healthcare that they provide.
Apparently, there was an attempt to produce an NCD policy in the late 1990s but the document did not translate into anything substantial. Another effort in 2009 has yielded an NCD policy draft.2 The document has outlined overall goals, objectives and strategies for NCD control and prevention. Highlights include integrated management of risk factors, capacity building and training, and surveillance. Unfortunately, the draft is yet to be endorsed by the government because of the ongoing political imbroglio. Furthermore, policies in other health-related sectors such as transport and agriculture also do not address CVD issues.
Health-related legislative measures have also been absent or weak in implementation. Nepal had signed the WHO Framework Convention on Tobacco Control in 2003. However, there is still no comprehensive anti-tobacco legislation, which should have been immediately in place after the ratification of the framework in 2006.
On the international front, the Global Strategy on the Prevention and Control of NCDs was formulated at the turn of the millennium. However, the implementation of the strategy did not take place in most of the LMICs, and was probably overshadowed by a larger global agenda, the MDGs. Although some industrialised nations like the USA could implement the objectives under the ‘Healthy People 2010’ programme,31 LMICs such as Nepal have been far from having any real plans. Nevertheless, a Southeast Asian Regional Civil Society Meeting in Nepal in January 2011 has helped to rekindle the regional and national effort towards NCD control including CVDs. The meeting was in preparation for the 65th UN General Assembly, which is expected to come up with concrete plans on NCD control at the global level, in particular on how to align the issue of NCDs with the MDGs (table 1).32–34
Time-line of important global and regional events pertaining to CVD control in Nepal
Implementation: overcome the challenges and grab the opportunities
The challenges and opportunities that are present in Nepal for CVD control are outlined in box 1 and feature in figure 1 as well. A concerted effort by all stakeholders at all levels is the call of the day if Nepal wants to control the burgeoning epidemic of CVD.
Challenges and opportunities for cardiovascular disease (CVD) control in Nepal
Challenges
Political instability, malfunctioning governance, weak laws
Inadequate commitment of government and external developmental partners towards CVDs
Inferior healthcare facilities
Poor health literacy, rigid public attitude, adverse health behaviour
Limited trained workforce in CVHD prevention and control
Health inaccessibility: geographical, economical, etc
Prime focus on curative methods of disease control
Rapid urbanisation, rising purchasing capacity, exposure to unhealthy food and lifestyle
Opportunities
A well-set healthcare delivery system from the centre to the grass-root level
A successful primary healthcare system that caters to a wide population base
Greater proportion of children and young: opportunity for primordial prevention
Increasing numbers of medical colleges across the country: advantage for referral of cases
To ensure the smooth implementation of CVD strategies, the following areas, as advocated by the Centers for Disease Control and Prevention, shall need strong individual attention.35
Communication to convey the urgency and importance of CVDs through a long-term strategy of public information and education
This is an important aspect of CVD control as most of the risk factors are behavioural in origin and they need to be tackled at an incipient stage through health promotional activities. Indeed, studies have shown that cardiovascular health literacy in Nepal is poor.36 37 The opportunity to mobilise community health workers to spread relevant heart health messages exists and its use has been successfully demonstrated in maternal and child health. Primary healthcare settings that reach down to the grass-root level throughout the country would be the most sustainable way of disseminating heart health messages to the public. Such a community-based health promotional primary care approach has been successfully demonstrated in many resource-constrained settings such as in Chandigarh, India,38 and in Ashanti, Ghana.39 Developed countries have used other methods and techniques such as telephone40 and email41 messages for health promotion, which may not work in Nepal because of the limited availability of technology and poor health literacy.
Public health leadership and partnership to foster effective leadership for CVDs
There is a dearth of public health personnel trained in CVDs and thus there is an urgent need to groom staff in this sector. Partnerships between government and private institutes are not conducive, leading to a lack of concerted efforts to deal with CVDs. Lately, the Nepal Public Health Foundation, a non-governmental organisation, has taken up the issue of NCDs and is working towards bringing all the stakeholders together.
Work from other developing and often politically disturbed countries such as Pakistan and Iran illustrates how CVD prevention can still be carried out with vision, leadership and partnership. The Isfahan Healthy Heart Program42 in Iran and the Heartfile Lodhran CVD Prevention Project43 in Pakistan produced integrated public–private partnership models to work conjointly towards improving the heart health of the country, many of which are applicable in Nepal's context as well.
Action priorities to identify effective policies in cardiovascular health promotion and CVD prevention at the national and local levels to ensure effective public health action against CVDs
Although the NCD policy in Nepal was already drafted in 2009, no short-term and long-term programmes based on the policy have been formulated yet. At present, the Ministry of Health and Population appears to be at a loss on how to implement the policy in reality.
For effective implementation of the NCD policy, the geographical, ethnic, rural–urban diversities and differences must be considered while formulating action plans because the health system provision and health-seeking behaviour in urban areas are entirely different from those in the agriculture-based rural areas. For example, physical inactivity is not a problem for farmers whereas it is one of the major risk factors for CVDs in city dwellers. Tobacco and alcohol, on the other hand, are almost equally used in both rural and urban areas, but they have to be dealt differently when it comes to their control. In the villages, these addictions are centred on the agricultural work and often they are the only means of leisurely pleasure and escape, whereas in the towns they often underline the urban despair, glamour and peer pressure.
Organisational capacity at the national and local levels, including laboratories, to address CVDs and develop the needed competencies and resources through training
The existing hierarchical healthcare system that is decentralised from the centre to the grass-root level can be upgraded and adapted to take up CVDs. The existing healthcare staff have to be trained in order to deal with the present situation of CVDs in the country, which might only be the tip of the iceberg. The health policy should ensure equitable distribution of the workforce. The grass-root level health workers can be used to screen for CVDs and risk factors such as high blood pressure as well as for health promotional activities as shown by the study in Chandigarh, India.38
Optimal laboratory backup is essential and a hierarchical model similar to the one for communicable diseases can be adopted for NCDs as well. The use of simple techniques such as glucometers for blood sugar readings and instruments for blood pressure and body mass index measurements should be possible at the lower levels of the healthcare system. A referral system with availability of secondary and tertiary services in the district and central hospitals will ensure cost-effective utilisation of resources.
Besides, Nepal has recently witnesses an increase in the number of new private medical colleges being set up across the country. These private medical colleges can be involved as partners in NCD control because they have the technical workforce and laboratories and can provide tertiary care services.
Monitoring and evaluating the burden of CVDs and measuring progress in prevention and treatment
This has to be achieved by expanding and standardising resources and activities and by establishing frameworks, methods and core indicators for evaluation of policies and interventions. Here, it may be important to develop clinical and programme evaluation protocols that are most appropriate in Nepal's context. The healthcare system can learn a lot from the successful adoption of health programmes for communicable diseases such as malaria, tuberculosis and leprosy. The development of longitudinal surveillance systems to monitor progress would also be beneficial in this context.
Policy research to develop a comprehensive agenda that fosters translation of this research into practice
Appropriate methods for translation and dissemination of knowledge must be determined and tailor-made to suit the local circumstances. Research to identify best practices for effective interventions should be carried out simultaneously along with the implementation of the intervention itself. In this context, Nepal can initiate the NCD interventions as pilot programmes in some districts of the country and a simultaneous operational research can be carried out to provide crucial insights to expand the programme to national or subnational levels.
Regional and global collaboration to engage regional and global partners in mobilising resources for CVD prevention and treatment
The public health personnel and cardiologists in the region can come together, for example, to develop specific guidelines for CVD risk assessment in the South Asian population. There should be opportunities to carry out collaborative work at the regional and international levels on various aspects of CVDs—from community to catheterisation laboratory and from prevention to intervention. International agencies should stop ignoring the rising problem of CVDs in the region. They should also coax the health policy makers in the region to initiate or accelerate programmes towards CVD control.
Conclusion
Nepal is at an interesting juncture as far as CVDs are concerned. Although in bits and pieces, we now do have data that can no longer be overlooked but rather require us to come up with definite plans and policies for the prevention and control of CVDs. A rejuvenated global and national interest has given us an ideal platform to launch CVD-related policies and programmes. It is now time to combine all these forces and put our plans into action.
Acknowledgments
The author would like to thank Associate Professor Alexandra Krettek, Nordic School of Public Health, for reviewing the manuscript.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; internally peer reviewed.