Article Text

Abstract
Background Complete atrioventricular block complicating acute anterior wall ST elevation myocardial infarction (MI) is classically considered one of the worst prognostic indicators.
Methods We present the case of a gentleman who developed complete atrioventricular block during the course of acute anterior wall ST elevation MI, and had spontaneous resolution of the same. Mechanisms of spontaneous resolution of complete atrioventricular block in the setting of acute MI are discussed. Attention is drawn to a subgroup of patients, albeit a minority, who have a better prognosis owing to reversible causes than classically expected and seen.
Results Clinical features suggested that this patient had reocclusion of the infarct-related artery after thrombolysis on presentation and spontaneous reperfusion.
Conclusion Coronary angiography provides invaluable information for decision making in such clinical scenarios. Complete atrioventricular block due to reversible ischaemia produced by reocclusion of an infarct-related artery should be reversible by percutaneous coronary angioplasty of the infarct-related artery. We suggest that reversible causes be considered before attributing atrioventricular block to irreversible damage, which would require a permanent pacemaker implantation. This would be more significant in most of the developing world, where resources are scarce.
Statistics from Altmetric.com
Case description
A 47-year-old gentleman with no history of conventional risk factors for coronary artery disease presented with rest angina of 3 h duration, Killip class I. His ECG showed right bundle branch block, left posterior hemiblock and ST elevation in leads V2–V5 (figure 1; above). He was advised immediate reperfusion therapy in addition to other guideline-directed medications. The family opted for thrombolytic therapy with streptokinase owing to lack of insurance cover and financial constraints for primary percutaneous coronary intervention (PCI). Thrombolysis was successful by clinical and ECG criteria. There was resolution of ST elevation and the bundle branch block (figure 1; below). Cardiac enzymes were elevated on admission. Bedside echocardiography showed severe hypokinesia of left anterior descending artery territory, severe left ventricle (LV) dysfunction.

ECG on admission; right bundle branch block, left posterior hemiblock and ST elevation in leads V2–V5 (above) and post-thrombolysis ECG; resolution of ST elevation and bundle branch block (below).
He maintained stable hemodynamics during the initial 48 h. On day 3, his ECG showed re-elevation of ST segments and reappearance of right bundle branch block along with Mobitz type 2 AV (atrioventricular) block (figure 2; above). An immediate transvenous temporary pacemaker insertion was done (figure 2; below). Within a few hours, the ECG showed progression to complete atrioventricular block with broad QRS slow ventricular rate (figure 3; above). Cardiac enzymes were elevated above the previous levels. The patient did not have recurrence of angina during this event, nor did he develop clinical features of acute left ventricular failure. He was continued on low molecular weight heparin (LMWH), aspirin, clopidogrel, high-dose statin and angiotensin converting enzyme (ACE) inhibitor with temporary transvenous pacemaker support, as the scenario precluded a ‘rescue’ PCI, as mentioned above.

ECG on day 3; re-elevation of ST segments and reappearance of right bundle branch block along with Mobitz type 2 atrioventricular block (above) and ECG after temporary pacemaker insertion (below).

Day 3; progression to complete atrioventricular block with broad QRS slow ventricular rate (above), and day 5, resolution of ST elevation and complete atrioventricular block (below).
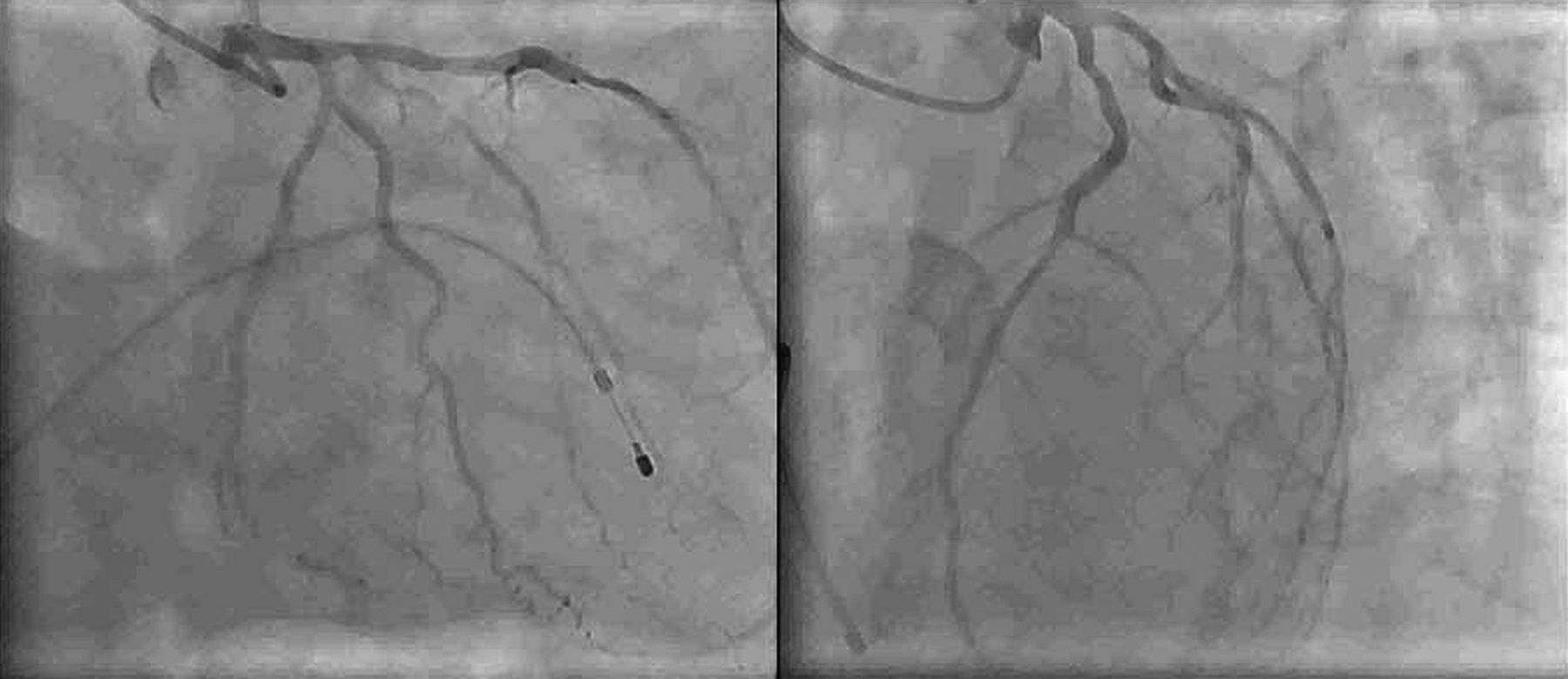
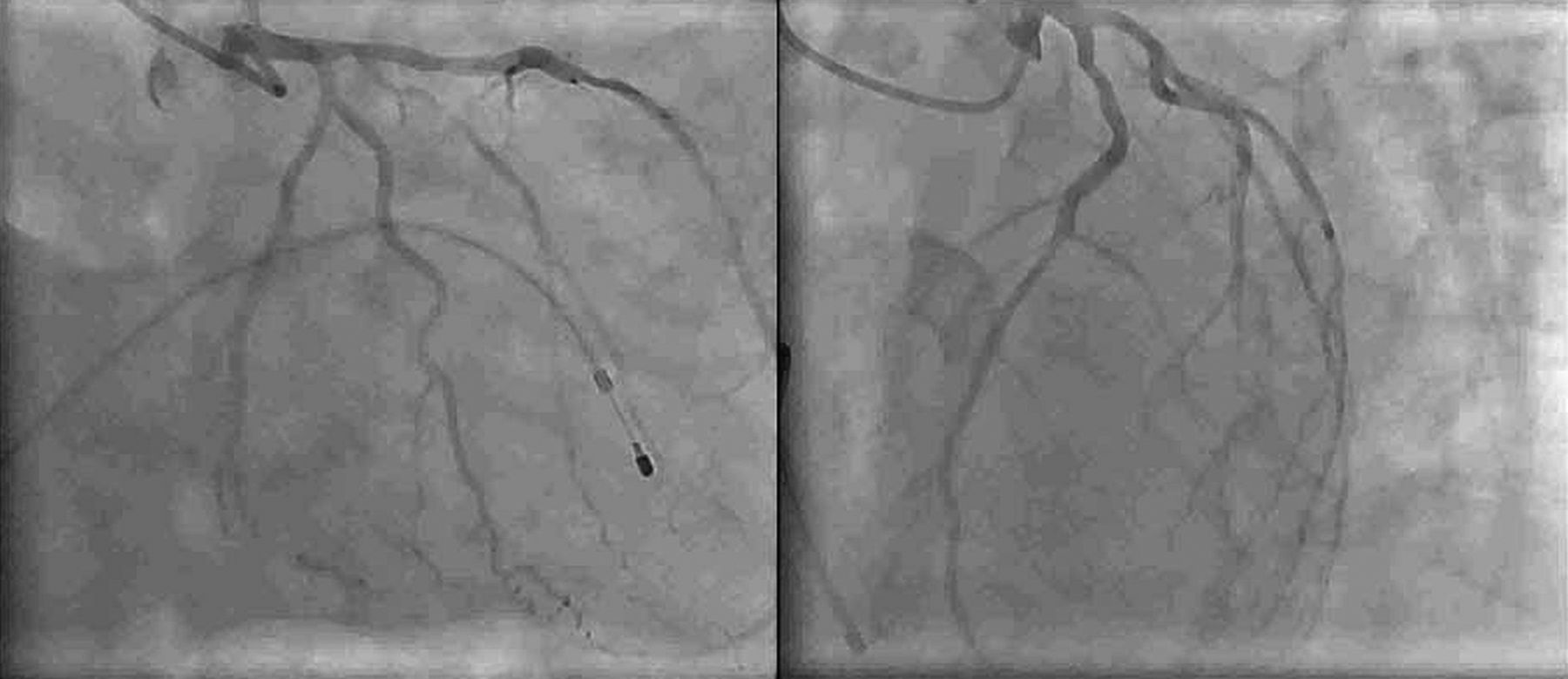
On day 5, day his ECG showed resolution of ST elevation and complete atrioventricular block (figure 3; below). Meanwhile, the family arranged resources for a coronary angiography with intent for PCI of the infarct-related artery if needed. It was decided to go ahead with the coronary angiography, as delineating the coronary anatomy was essential in a rapidly changing clinical scenario in addition to the postmyocardial infarction risk-stratification point of view. Transradial coronary angiography revealed a patent left anterior descending artery with minor plaques (figure 4), and minor disease in distal right coronary artery. The patient was continued on optimal medical management. He was observed in hospital for 2 more days and discharged on guideline-directed medical therapy.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patent left anterior descending artery with minor plaques.
At 3 months follow-up, he was asymptomatic, had no evidence of bundle branch/AV block on ECG and 24 h Holter. His echocardiography showed significant improvement in left ventricular function. He is on regular follow-up, and is doing fine 20 months after the event.
Discussion
The finding of bundle branch block on ECG in the setting of acute ST elevation myocardial infarction (MI) implies extensive infarction, and identifies patients at higher risk for complications.1 Both left and right bundle branch block are associated with higher in-hospital and long-term mortality.2 Mortality is high owing to the occurrence of severe pump failure secondary to the extensive myocardial necrosis required to produce extensive intraventricular block,3 rather than due to the conduction disturbance.4 The high rate of mortality has been found to occur even in the absence of high-grade AV block.4 Bundle branch blocks had been reported to occur in 5%–10% of patients with ST elevation MI (STEMI) in the prefibrinolytic era, and in 2%–5% in the reperfusion era.5 The reduced incidence in the thrombolytic era is attributed to enhanced reperfusion and limitation of infarct size.6 ,7 The reduced incidence in non-thrombolysed patients reflects the overall improvement in medical management.8–10 Even though the incidence has been found to be decreased, right bundle branch block is still found to be associated with poor clinical outcome in patients with anterior myocardiaI infarction even in the coronary intervention era.11 The patient described here belonged to the high-risk category, and primary PCI would have been a better choice for him.
After an initial stable period, the clinical course turned stormy with the reinfarction and appearance of complete AV block a few hours later. Atrioventricular block in anterior infarction is usually the result of extensive septal necrosis that involves the bundle branches. The high rate of mortality in this group of patients with slow idioventricular rhythm and wide QRS complexes is also attributed to extensive myocardial necrosis, which results in severe left ventricular failure and often shock, as in the case of patients with bundle branch blocks.4 The discussed patient's characteristics fit into the classical description of complete atrioventricular block in anterior infarction and, accordingly, the family was explained of the prognosis and the need for rescue PCI, and the possible need of a permanent pacemaker. Logistic reasons precluded a rescue PCI at this point of time, and he was continued on medications. Spencer et al, after analysing two-decade-long trends of complete atrioventricular block associated with acute STEMI concluded that though the incidence of complete AV block complicating acute MI has declined with time, these patients remain at an increased risk of in-hospital mortality. They observed that the long-term prognosis of patients with inferior MI and complete atrioventricular block is similar to that of patients in whom complete atrioventricular block did not develop, whereas patients with anterior MI and complete atrioventricular block may be at an increased risk of long-term mortality.12
There had been conflicting reports from the early thrombolytic era as to the incidence of complete atrioventricular block. Verstraete et al9 found a non-significant tendency to higher ratios of second- and third-degree AV block associated with rt-PA (8%) versus streptokinase (2%).13 Harpaz et al found that thrombolytic therapy was independently associated with a twofold increased risk for the development of complete atrioventricular block.14 Others found that there was no increased or decreased risk.15–17 Harpaz et al propose association as an explanation for this, that is, patients with larger infarcts receiving thrombolysis, they also being more likely to develop AV block.14 Although this explanation is plausible, the findings point to the possibility of alternative mechanisms in operation responsible for complete AV block in the setting of acute anterior wall MI.
The spontaneous resolution of complete atrioventricular block and ST elevations on day 5 after the reinfarction on day 3 in the described patient points to reversible mechanisms. Wilber et al described two patients who showed resolution of complete atrioventricular block within minutes of late reperfusion (>40 h) by angioplasty in anterior infarction, suggesting reversible ischaemia rather than extensive necrosis of the proximal conduction system as the mechanism of heart block in this subgroup.18 Harpaz et al also attributed resolution of complete heart block(CHB) in survivors to spontaneous or medical reperfusion causing relief of ischaemia.14 Whereas AV block due to necrosis of the conduction system would invariably be irreversible and lead to permanent pacemaker implantation, the alternative mechanisms seem reversible, thus avoiding permanent pacemaker and sparing resources. AV block attributable to reocclusion and reversible ischaemia can be reversed by PCI of the infarct-related artery, as shown by Wilber et al in anterior infarction,18 and Ramamurthy et al in inferior infarction.19 AV block, attributable to reversible ischaemia outside the setting of acute myocardial infarction (AMI) and resolution by reperfusion, was also demonstrated by others.20–22 The conduction system being relatively resistant to ischaemia,23 can recover function faster than the adjacent myocardium once the ischaemia is reversed. Transient complete atrioventricular block has also been reported as being caused by occlusion of the first septal perforator branch during PCI of left anterior descending coronary artery.24 Reversible ischaemia seems to be the most plausible explanation for transient complete heart block in anterior wall MI, the same being applicable in our patient too. This was confirmed by a patent infarct-related artery on coronary angiography in our patient. Possibly, an ongoing thrombotic process was aborted spontaneously, aided by the antiplatelet and antithrombotic strategies. Visualisation of coronary anatomy is essential for decision making in such situations.
Other suggested mechanisms include reperfusion injury and vagal mediation.14 Clemmensen et al, from the TAMI study group, in their study of complete AV block complicating inferior wall MI, found a similar incidence of complete atrioventricular block with thrombolysis compared with the prethrombolytic era. They also found that complete atrioventricular block was associated with an active component of reperfusion therapy in 38% of patients, suggesting that reperfusion could itself provoke the AV block associated with acute inferior wall MI either via reperfusion injury or reocclusion of the opened-up artery.25 Thus, successful reperfusion, pharmacologically or invasively achieved or clinical markers of reocclusion, as in our patient, should alert the clinician of this possibility. Even though complete atrioventricular block was mostly limited to patients with inferior wall MI due to complete occlusion of the right coronary artery in their study25, complete atrioventricular block with anterior wall infarction can also similarly be linked to reperfusion. Having stated this, it should also be mentioned that the major effect of reperfusion on the natural history of complete AV block is to minimise its duration, by decreasing ischaemia of the AV node.
Vagally mediated complete atrioventricular block has been suggested as a sign of successful reperfusion.13 Restoration of flow has been found to facilitate leukocyte migration to the infarcted area, and to stimulate vagal nerve endings in the inferoposterior aspect of the left ventricle.23 Higher afferent vagal activity in the posterior ventricular myocardium, accounting for the vagomimetic effects of inferior MI suggests that flow restoration stimulating vagal nerve endings, causing AV block should be more applicable in the setting of inferior wall MI than anterior wall.
Conclusion
The resolution of complete atrioventricular block in this patient after a classical presentation and identification of a patent infarct-related artery with no significant stenosis on coronary angiography draws attention to a subgroup of patients, albeit a minority, having a prognosis better than expected. This patient probably had a reocclusion of the infarct-related artery and spontaneous reperfusion, supported by the re-elevation of ST segments and cardiac enzymes at the time of reappearance of the bundle branch block along with AV block. Complete atrioventricular block due to reversible ischaemia produced by reocclusion of an infarct-related artery should be reversible by percutaneous coronary angioplasty of the infarct-related artery. The information provided by coronary angiography regarding the status of the infarct-related artery in such scenarios is invaluable for clinical decision making. It is worthwhile considering this possibility before attributing the AV block to irreversible damage, which would require a permanent pacemaker implantation, especially in resource-scarce settings.
Acknowledgments
We thank Dr Shyam Sunder Kothari, Professor of Cardiology, All India Institute of Medical Sciences, New Delhi and Dr Ajay U Mahajan, Associate Professor of Cardiology, Lokmanya Tilak Municipal Medical College and Hospital, Sion, Mumbai for reviewing the manuscript.
References
Footnotes
-
Contributors Dr NS and Dr IK were involved in conception and design, analysis and interpretation of data, drafting the article, revising it critically for important intellectual content and final approval of the version to be published. The patient mentioned in the case was under the care of Dr IK.
-
Funding None.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; internally peer reviewed.