Article Text

Statistics from Altmetric.com
- Acute stroke
- primary angioplasty
- recombinant tissue plasminogen activator
- glycoprotein GP IIb/IIIa inhibitor
- stroke
- carotid artery disease
- thrombolysis
Introduction
Mortality rates associated with basilar artery occlusions, internal carotid artery ‘T’ occlusions and middle cerebral artery (MCA)–M1 segment occlusions are particularly high despite the best available medical therapy. The recanalisation rate of a patient with carotid T occlusion is 10%1 2 with intravenous thrombolysis and 33% with intra-arterial (IA) thrombolysis.3 We report a case of acute stroke in whom primary angioplasty of the left internal carotid artery followed by IA thrombolysis of MCA was done with a favourable outcome in our centre. This is the first reported case of such a procedure in India.
Case report
A 65-year-male subject who is a known diabetic and smoker presented with a history of blurring of vision of 6 h duration, followed by global aphasia and right sided hemiplegia of 2 h duration. The patient had global aphasia, gaze deviation to left side and right sided hemiplegia at admission. At presentation, National Institutes of Health Stroke Scale was 28. MRI brain showed restricted diffusion in basal ganglia, anterior cerebral artery/MCA and posterior cerebral artery/MCA watershed area (figure 1). Magnetic resonance angiogram showed complete occlusion of left internal carotid artery from the origin with occlusion of left MCA and A1 segment of anterior cerebral artery (figure 2). As the patient had symptoms of 6 h duration and long segment occlusion, the patient was taken for intervention.

Diffusion image showing patchy restricted diffusion in left middle cerebral artery territory.
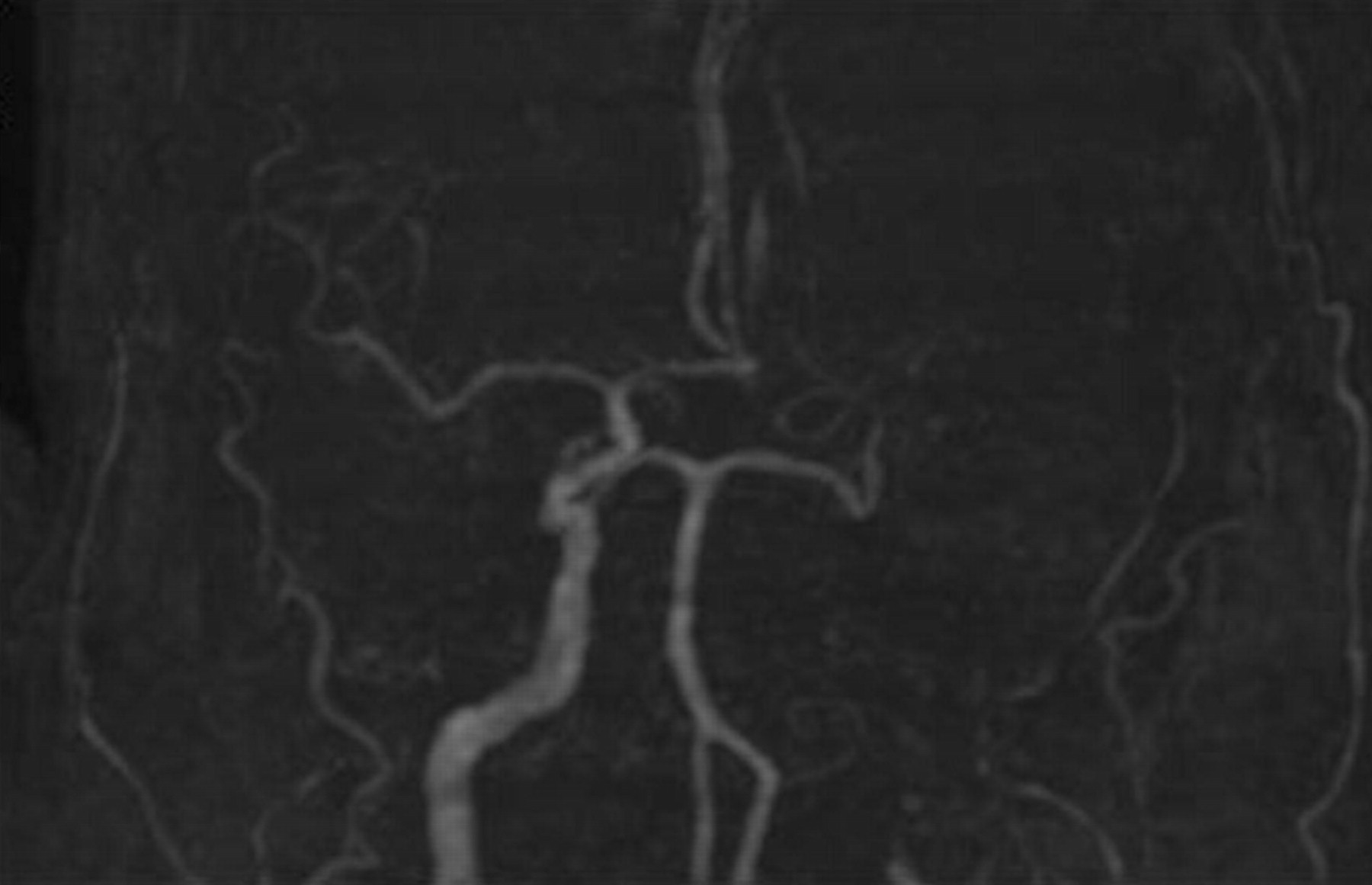
MR angiogram showing complete occlusion of left internal carotid artery (ICA) and middle cerebral artery.
Under general anaesthesia, 6F guiding catheter was negotiated into the left common carotid artery (figure 3). The patient received 3000 U of heparin bolus. Micro catheter was then navigated into the thrombus distally into the MCA bifurcation. Using exchange length 014 wire, angioplasty was done using 2×12 voyager balloon in supraclinoid, cavernous and petrous segment of internal carotid artery (figure 4). Angiogram showed residual severe stenosis of petrous internal carotid artery segment. Using 4×20 balloon, repeat angioplasty was done in the petrous internal carotid artery segment. Angiogram showed good recanalisation of entire internal carotid artery. Using micro catheter, recombinant tissue plasminogen activator (rtPA) infusion (20 mg) was performed in a small dose in M1 segment of MCA. Then, the internal carotid artery showed sluggish flow indicating reocclusion. So, 5 mg GP IIb/IIIa inhibitor (reopro) was injected slowly in the cervical internal carotid artery. Within 5 min, there was complete recanalisation of the entire internal carotid artery and MCA (figure 5). Following the procedure, the patient was sedated and ventilated for 12 h and postextubation, clinical examination showed complete recovery.

Left common carotid artery angiogram shows complete occlusion of left ICA.

Angioplasty of supraclinoid ICA using 2×12 balloon.

Final angiogram shows complete recanalisation of ICA and middle cerebral artery.
CT brain plain (figure 6) done 24 h after procedure showed hypo density in the left lentiform nucleus and water shed territory of left MCA as was seen in the preprocedure MRI-diffusion weighted imaging. There was no evidence of any reperfusion haemorrhage.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Twenty-four h postprocedure CT brain plain did not reveal any reperfusion haemorrhage.
Discussion
Management of acute ischaemic stroke has always been a formidable challenge. Various treatment strategies available today lead to higher rates of recanalisation. The efficacy of intravenous thrombolysis in acute ischaemic stroke has been proven in National Institute of Neurological Disorders and Stroke trial. But, only 10% of patient with carotid T occlusion will have recanalisation with intravenous thrombolysis.1 2
So, for patients with large vessel occlusion, IA thrombolysis is one of the treatment modalities available. But, even with IA thrombolysis for carotid T occlusion, the recanalisation rate with IA thrombolysis is only 33%. In the study by Gonner et al, the recanalisation rate was 63%. Twenty-one percent recovered to modified Rankin Scale score (mRS) scores 0 or 1, and 40% to scores of 2 or 3. The outcome was good (mRS 0–3) in 80% with MCA occlusions, in 33% with ICA and in 50% with basilar artery occlusions.3
In a study of carotid T occlusion patients treated by IA thrombolysis, four patients (16.6%) had a favourable (mRS≤2) and 10 patients (41.7%) a poor outcome (mRS 3 or 4) after 3 months. Ten patients (41.7%) died. One symptomatic intracerebral haemorrhage (4.2%) occurred. Partial recanalisation of the intracranial internal carotid artery was achieved in 15 (63%) of the MCA in four (17%), and of the anterior cerebral artery in eight patients (33%). Complete recanalisation never occurred.4
In a retrospective study of carotid T occlusion patients, the lowest recanalisation rates were observed with IA lytics alone (3/17, 17.6%). Mechanical embolus removal in cerebral ischaemia embolectomy alone achieved 46.2% recanalisation rates (6/13; p=0.23). Angioplasty or stenting and IA lytics achieved 25% (2/8; p=0.65) and 40% (4/10; p=0.085) recanalisation.5
The procoagulation activity may increase tremendously immediately post-thrombolysis with rtPA (peaks after 1–3 h and persists up to 72 h), indicating that thrombolysis may trigger the coagulation cascade and hence enhance thrombin formation at the site of occlusion. This may be the explanation for reocclusion after IA thrombolysis.6 So, GP IIb/IIIa inhibitors can be used along with rtPA to have a synergistic effect.7
Thus, for a patient with a long segment occlusion, multimodality treatment with combination of mechanical and chemical treatment is necessary.8
Conclusion
Multimodality treatment is an option for patients who present with acute ischaemic stroke with a long segment (carotid and MCA) occlusion.
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; internally peer reviewed.