Article Text

Abstract
Objectives To find out and explore the knowledge and opinion of Chinese people on cardiovascular disease and awareness of cardiac rehabilitation.
Design A cross-sectional study using 14-item bilingual (Chinese and English) questionnaires that include information on demographics, health status, cardiovascular disease related knowledge and perception, and awareness and understanding of the cardiac rehabilitation programme.
Setting Chinese community groups in the Midlands, UK from January to April 2008.
Participants 436 questionnaires from Chinese adults over 18 were obtained.
Main outcome measures Current knowledge and attitude towards cardiovascular disease and awareness of cardiac rehabilitation.
Results Obesity was the most common risk factor identified by 80.7% of participants. Those originated from China had significantly less knowledge compared with subjects from other countries (p<0.001). People who have had exposure or experience of cardiac disease rated a higher risk of cardiac disease for Chinese living in the UK than people without experience. A majority (81.7%) used orthodox medicine and perceived it to be most effective against cardiac disease. Only 30% of participants were aware of cardiac rehabilitation.
Conclusion The coronary artery disease (CAD) risk factors of Chinese population have increased significantly in the last decade. Cardiac rehabilitation awareness was poor among the sample population of this study and language barrier is still a problem. More large studies on Chinese population assessing CAD risk should be done to provide more evidence on CAD prevention for this growing population in the Western world.
- Intensive care
- cardiac surgery
- cardiac function
- coronary artery disease
- congenital heart disease
Statistics from Altmetric.com
Background
Coronary artery disease (CAD) has been on a rapid rise in China over the past few decades.1 The number of deaths from CAD in China is the second highest in the world, after India.2 This was due to rapid economic development in China over the past 20 years3 which has allowed people to change their living conditions and lifestyle, becoming more sedentary and consuming unhealthy diets. This has led to an increase in prevalence of risk factors related to CAD such as diabetes,4 hypercholestrolaemia5 6 and hypertension.5 Another main risk factor of CAD is smoking, China being the greatest producer and consumer of tobacco products worldwide,7 and consumption of tobacco products is becoming more popular among Chinese teenagers.
In 2001, 0.4% of the total UK population were Chinese,8 and between 2004 and 2005, there was an estimate of 10.2% increase.9 With growing numbers of Chinese immigrants coming into the UK, accompanied by their lifestyle behaviours, it is possible that a sharp rise in incidence of CAD among UK Chinese may occur.
Cardiac rehabilitation, a secondary prevention intervention for CAD, has been shown to be successful in lowering mortality rates in treated patients.10 However, only 30% of eligible patients participate in such programmes and only about a third maintain attendance after 6 months.11 In addition, patients of ethnic minorities are less likely to be referred or attend the programmes due to lack of awareness and the widely varying capacity of cardiac rehabilitation centres to provide the service12 and being non-English speaking reduced the likelihood of attendance by nearly 10-fold.13
Past studies suggested that there was a widespread lack of knowledge of the risk factors of heart attacks among the US general public especially in ethnic monirities.14–16 Another study suggested that the prevalence of CAD was significantly lower in UK Chinese than Caucasian men due to a favourable risk factor profile in UK Chinese.17 However, this study was done between 1991 and 1993 and so it may be outdated. This cross-sectional study was undertaken to demonstrate these topics and the current state of the Chinese health belief with regard to CAD.
Method
This cross-sectional quantitative study was conducted with an aim to find out the knowledge and awareness of cardiac disease in the Chinese populations around various cities in the UK.
Participants
Six hundred bilingual 14-item questionnaires (online appendix 1) were dispatched, of which 436 (72.7%) were returned and analysed from Chinese adults who were not from the medical profession.
Participants were selected by cluster sampling of a number of Chinese community groups in various nearby cities around the Midlands including Birmingham, Nottingham, Leicester and Coventry. Snowball sampling was also used whereby respondents were asked to voluntarily pass on questionnaires to their family, friends and colleagues.
The Chinese population in the Midlands in 2005 was 53 400.9 Although our sample population made up a small percentage of the whole population in the Midlands, it may still be representative as we targeted places with high density of Chinese people and included various backgrounds, as stated in the above criteria.
Data collection
Information was gathered by self-administered bilingual (Chinese and English) questionnaires, which were distributed between January and April 2008. Completed questionnaires were either collected immediately or sent back via mail or electronically at a later date.
A 14-item questionnaire was distributed to measure the main areas of interest, including knowledge of risk factors, perceived risk of CAD, awareness and understanding of cardiac rehabilitation, and use and perceived effectiveness of Chinese and orthodox medicine. Subjects were asked a series of questions with Likert scales and tick boxes. In addition, baseline characteristics such as age, gender, country of origin, social class and educational level were recorded.
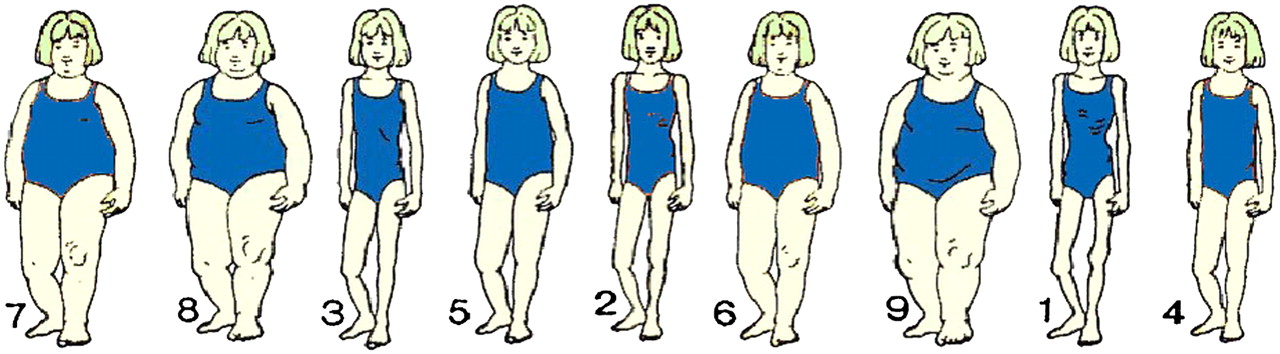
Perception of health with regard to obesity was determined by a visual analogue scale (figure 1) showing girls with various body mass indices (BMIs). Participants were asked to choose which BMI they think is healthiest, least healthy and most at risk of getting CAD.
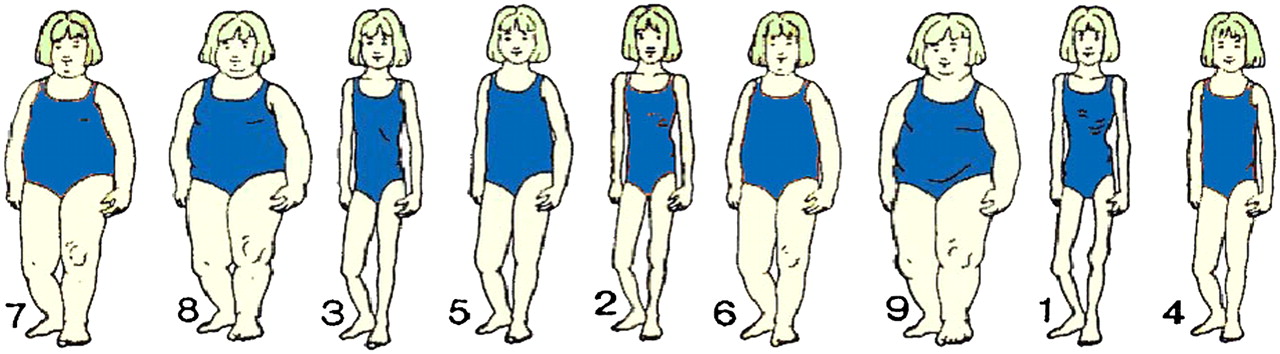
A visual analogue scale of girls with various body mass indices.
Statistical analysis
The data collected were encoded and Statistical Package of Social Science V.16 (SPSS) was used for analysis. Baseline characteristics of our sample population were summarised descriptively in table 1.
Sample characteristics (n=436)
Risk factor awareness was calculated by scoring each individual out of 18 on the basis of accurately identifying the risk factors for cardiac disease and correctly responding to a list of statements regarding conservative management post cardiac event. This score was further analysed by using independent t tests to compare any differences in means between the subgroups of the various baseline variables, such as age, gender, educational level, country of origin and cardiac disease experience. If the independent grouping variable consisted of more than two groups, for example, country of origin, a K-independent t test such as Kruskal–Wallis H test was utilised.
Differences in means within the various baseline subgroups for each of the perceived cardiac disease risks in the UK and in China were investigated separately by the Mann–Whitney U test. The mean difference in perceived cardiac disease risks of Chinese population in UK and China was collectively analysed by a non-parametric Wilcoxon test.
The relationship among the individual's health awareness, perceived curability, seriousness and individual susceptibility of cardiac disease was tested using χ2 and linear regression analyses. χ2 Analysis was used in this case to see if the differences found, if any, were due to chance. If statistically significant differences were found, the association between the independent and dependent variables would be tested with linear regression analyses.
BMI values were compared among different age groups, genders and countries of origin by Mann–Whitney U test to investigate any significant variations in perception standards among these groups. χ2 Analysis was again used to compare the perceived effectiveness of Chinese and orthodox medicine among different age groups, genders and countries of origin.
Results
Characteristics of the participants
This sample population was predominately of the younger age group, aged 18–29 (n=181, 41.5%), of which 72% were students (n=127). The male to female ratio was found to be 2:3. The majority of our participants originated from Hong Kong (n=215, 49.3%) and China (n=100, 22.9%). Two hundred and thirty-nine participants (54.8%) had obtained an education of university level. Two hundred and twenty-seven participants (52.1%) reported having a cardiac disease experience.
Knowledge of risk factors
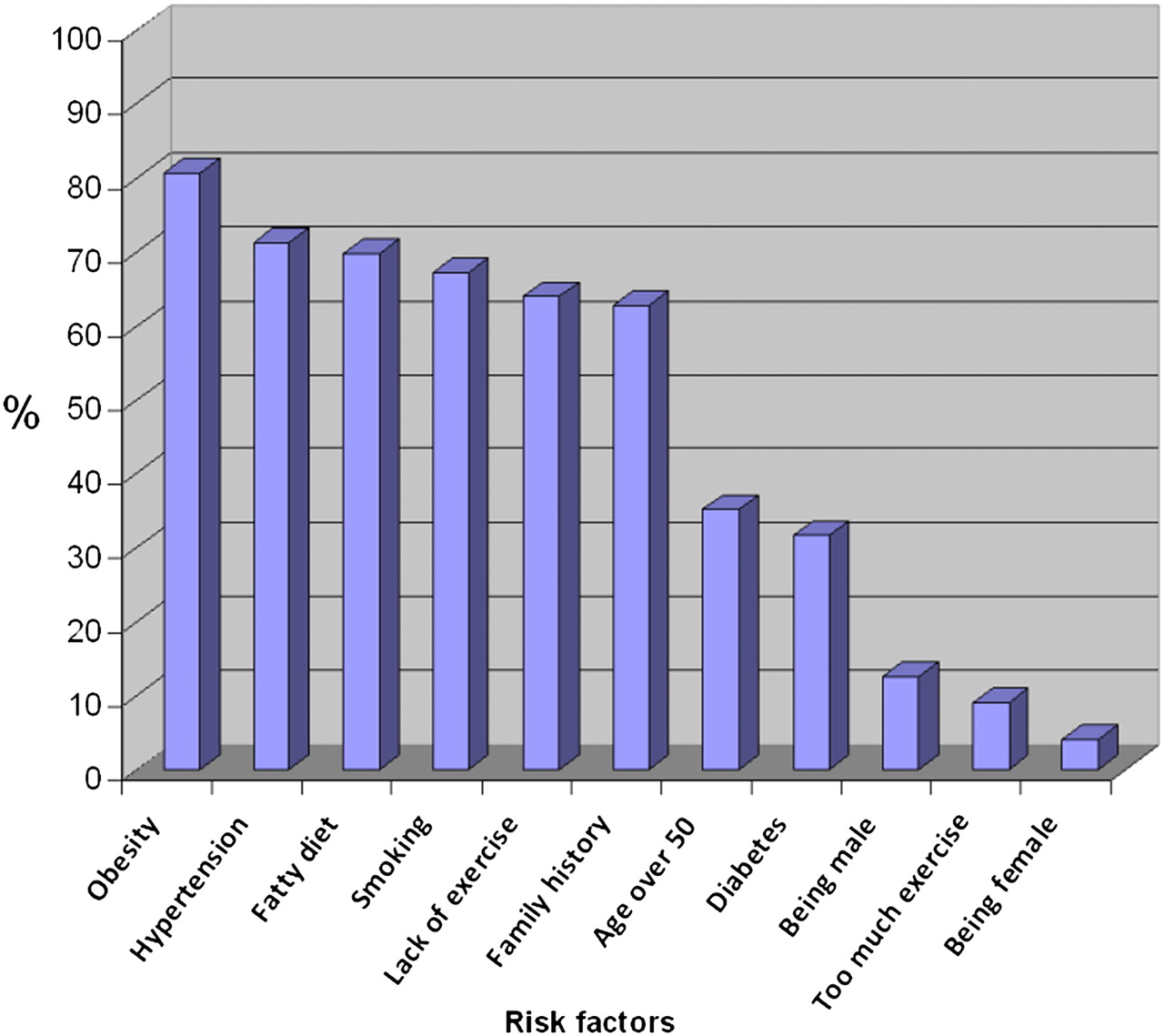
Figure 2 refers to the frequencies of the risk factors being chosen. Obesity was the risk factor most frequently identified (n=352, 80.7%). The behaviour-related risk factors, for example, smoking, exercise and diet were more readily identified. However, only a minority acknowledged that physiological risk factors, namely, being male (n=55, 12.6%), over the age of 50 (n=154, 35.3%) and having diabetes (n=138, 31.4%) were also important for cardiac disease.
{kind=link}
{kind=link}
Graph showing percentage of population identifying various risk factors.
Participants originating from China scored significantly less than those from other countries (p<0.001). While participants with cardiac disease experience scored higher than those without, this was not statistically significant (p=0.097).
Perception of obesity
Overall, 43.3% (n=189) of participants thought the image with a BMI of 20 was the healthiest looking, and 72.2% (n=315) recognised a stature with a BMI of 32.5 was at the highest risk of getting cardiac disease. In all, 20.2% (n=88) and 61% (n=266) of our population chose the lowest (12.5) and highest (32.5) BMI values of the scale respectively as being the least healthy.
Perception of risk of cardiac disease
Three hundred and thirty-two participants (76%) claimed that they were often conscious of their cardiac health when making lifestyle choices. Three hundred and ninety-six participants (90.8%) agreed or strongly agreed that cardiac disease is a serious illness, and most people thought they were at low (42%) or medium (40.6%) risk of getting cardiac disease themselves. Overall, 34.9% (n=152) remained neutral and were unsure whether cardiac disease is curable. Those with cardiac disease experience perceived a significantly higher risk of getting cardiac disease than those without (p<0.001).
Awareness of cardiac rehabilitation
Only 30% (n=132) of participants had heard of cardiac rehabilitation. Although many failed to illustrate what it involved, participants had optimistic views in terms of improvements in quality of life after rehabilitation.
Perceptions medicine for the treatment of cardiac disease
Overall, 81.7% (n=356) of our sample population used orthodox medicine more than traditional Chinese medicine (TCM) in the UK. There was a significant difference (p<0.001) in the perceived effectiveness among TCM, orthodox medicine and a mixture of both types. In all, 47.7% (n=208) and 44% (n=192) of participants perceived orthodox medicine or a mixture of both types respectively to be more effective for treatment of cardiac disease than Chinese medicine alone (5%, n=22).
Only nine participants (2.6%) using predominantly orthodox medicine thought Chinese medicine alone would be more beneficial. On the other hand, only seven out of 45 (15.6%) Chinese medicine predominant users thought orthodox medicine alone would be more effective for cardiac disease.
In all, 56.2% (n=63) of the older population (aged over 50) perceived orthodox medicine as the best treatment, whereas a combination of both types of medicine was a more popular choice among younger age groups (p<0.05).
Discussion
In this study, the perceptions of CAD of Chinese people were sought from different aspects. There were several findings in people's perceptions regarding CAD risk factors, knowledge score, TCM and orthodox medicine, and cardiac rehabilitation.
Knowledge of risk factors
In our study, only 12.6% of people recognised that being male was a risk factor. Being male is an important risk factor of CAD, especially in young Chinese adults.18 This reflects the need to address this risk factor in Chinese people in the prevention of CAD. From the conversations with staff members in the Chinese community centre, it was revealed that Chinese male subjects are more reluctant to acknowledge the diagnosis of cardiac disease. As a result, they may refuse to change their lifestyle and will not comply with the course of medication.
The knowledge score can reflect the level of cardiac disease knowledge. People from China score significantly lower. A majority of this group was overseas university students, and this may suggest that the educational background of these students is different from the Western world, with cardiac diseases being less well known in China. In addition, other factors such as lifestyle and socio-economic class may affect these findings.
Compared with a Canadian study,19 the risk factor awareness in Chinese respondents in our study was higher than that of the Canadians, as shown in table 2.
Comparison of awareness of risk factors between Chinese people in our study and Canadian people in a previous study
Western lifestyle and its consequence
Chinese migrants in the Western world have been associated with increasing acculturation, with more Chinese people living a western lifestyle. A study showed that Chinese people in the USA had higher CAD risks and levels of mortality from CAD than Chinese born in China.17
In China, increased consumption of fast food will inevitably lead to an obesity endemic among the Chinese population in the near future. In this study, 47% of people either agreed or remained neutral on the fact that losing weight is harmful for people with CAD. This suggested that they may not be certain of the benefits of losing weight in the context of CAD.
Prevention of cardiac disease
The three major risk factors, that is, smoking, hyperlipidaemia and hypertension, were incorporated into the questionnaire in the hope of determining the views of Chinese people on the benefits of risk factor reduction after myocardial infarction (table 3).
Statements to assess knowledge of secondary prevention (n=436, frequency (%))
Smoking
Over 90% of people realised the benefit of smoking cessation after myocardial infarction, which showed that people were generally aware of the harmful effect of smoking in the development of CAD. Traditionally, Chinese men smoke more than women, with 75% male persons compared with 4% female persons.20 Unfortunately, in China there no national campaigns against smoking yet, although many other countries including the UK have already started.
Lowering blood pressure
There was a varied response from people regarding the benefit of lowering blood pressure after myocardial infarction: 15.6% answered agree, 24.8% neutral and 34.2% disagree. Further conversation with older participants revealed that they acknowledged the benefits of lowering blood pressure while being aware of the unpleasant effect of hypotension. This indicated that people were not very certain about the importance of lowering blood pressure in the context of CAD.
Lower intake of fatty food
Overall, 95% of people agreed with the fact that eating less fatty food was beneficial after having myocardial infarction. It is also worth knowing that primary prevention of cardiac disease before it develops is as important as secondary prevention. Studies have shown that primary prevention achieved a fourfold reduction in CAD mortality compared with secondary prevention in England and Wales between 1981 and 2000 and a twofold reduction in Ireland between 1985 and 2000.21 22 Therefore, healthy diet and smoking cessation should be promoted to people nationwide as ‘prevention is better than cure’.
Perception of obesity
Traditionally, Chinese people think that a chubby child is healthier because fat people are comparable with the image of laughing Buddha, which represents prosperity. Also, a fat child was perceived as more likely to survive undernourishment in the past when living conditions were poor. Although this misconception still exist today, 88% of participants in this study thought that obese people were more likely to get cardiac disease, which suggests that most Chinese people have the correct perception of obesity as a CAD risk factor.
Risks of CAD also increased with the length of residence in developed countries.17 The Western lifestyle in the UK may put Chinese people at a higher risk of developing CAD, but only 14.1% of the participants in this study thought so, whereas 62.7% thought that the risk was moderate.
It is difficult to compare health risks based on BMIs in different populations as WHO definitions for overweight and obesity were established based on data from Caucasians. The Framingham heart study functions cannot be applied to other populations (such as the Chinese population) without recalibration.23 The Chinese Medical Association Subsection of Cardiovascular Disease adopted BMIs of 24 and 28 as cut-off points for overweight and obesity, respectively.24 Therefore, in order to allow more accurate prediction of risk of various metabolic conditions, further large-scale studies on Chinese populations are required.
Perception of cardiac disease risk
Participants with cardiac disease experience thought that Chinese living in the UK had a higher risk of cardiac disease. Most of the Chinese population in the UK are immigrants from Hong Kong and China from the large scale migrations in the periods 1950–1960 and 1980, respectively.25 These immigrants may now be at the peak age of risk of cardiac disease. As our survey was conducted in the UK, those with cardiac disease experience will most likely have experienced it in the UK. This may have influenced the perceived risk of cardiac disease in the UK.
Those without cardiac disease experience did not believe that the risk of Chinese people living in the UK in getting cardiac disease would be different compared with those living in China. This reflects the public understanding that the individual's lifestyle governs the risk exposure.
Cardiac rehabilitation
Cardiac rehabilitation is an effective intervention for patients recovering from acute cardiac illness or surgery. It reduces total mortality over 3 years by 20% and cardiac mortality by 26%. It is seen as an integral component of both acute stages and secondary prevention of CAD. It offers physical, psychosocial and educational support to patients for secondary prevention.26
In this study, 30% of the participants have heard of cardiac rehabilitation before. However, only a minority was able to describe a superficial definition of cardiac rehabilitation. The majority of participants appeared to be optimistic about cardiac rehabilitation.
Ethnic minorities did not appear to contribute to cardiac investigation and rehabilitation, with <1% of Chinese people attending cardiac rehabilitation.27 28 The inability to support minority languages plays a role in the inequality of recruitment of ethnic minority groups to cardiac rehabilitation.27 28 This suggests that language barrier is still one of the reasons for low attendance for cardiac rehabilitation in Chinese people.
Comparison of TCM and orthodox medicine
In all, 81.7% of participants utilise orthodox medicine principally. TCM is not registered free on the National Health Service and seeking a Chinese medical herbalist often requires expensive consultation fees on top of treatment costs. In addition, TCM is less readily available to the community as compared with orthodox medicine. These two were the main factors that influenced their choice of medicine.
It was originally believed that older population preferred Chinese medicine due to the fact that they tend to think in more traditional ways. However, it was found that the majority of the older participants perceived orthodox medicine as being more effective for cardiac disease. On the other hand, a combination of Chinese and orthodox medicine is a more effective choice for cardiac disease among a majority of the younger age group (aged 18–49).
This finding can be justified by the fact that there is no common traditional Chinese herbal medicine treatment for acute cardiac events. Chinese herbal medicine is more often used in the treatment of chronic illnesses like arthritis. This can also be used to explain why only 5% (n=22) of our participants thought Chinese medicine alone was an effective treatment for cardiac conditions. Indeed, it seems that the nature of the illness dictates the use of orthodox and Chinese medicine.29
Conclusions
From our study, we found that the level of CAD knowledge was significantly lower in people who originated from China. Also, the lifestyle of the Chinese does not appear to be dependent on the perceived CAD risk. Awareness of risk factors widely varies but in general Chinese people in our study identified more risk factors than Canadian people in a previous study (table 2). Cardiac rehabilitation awareness was poor among our sample population and language barrier is still a problem. As prevalence of CAD risk factors in the Chinese population has increased significantly over the last decade, with exponentially increasing numbers of Chinese immigrants coming into the UK, it may be necessary for further extensive health promotion to be achieved in the Chinese and also other ethnic minorities in the UK.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; internally peer reviewed.