Article Text

Statistics from Altmetric.com
A 3-year-old boy presented with a history of 2 weeks fever 1 year ago. At that time he was found to have nasal discharge, bilateral non-exudative conjunctivitis, glossitis, bilateral cervical lymphadenopathy and rash with peeling of the skin of the hands and feet. His investigations showed polymorphonuclear leukocytosis and increased Erythrocyte sedimentation rate (ESR) and C reactive protein. The child was diagnosed as having Kawasaki disease and was treated with intravenous immunoglobulin, aspirin and clopidogrel. A 2D echocardiogram at that time showed a diffuse aneurysm of the left main coronary artery.
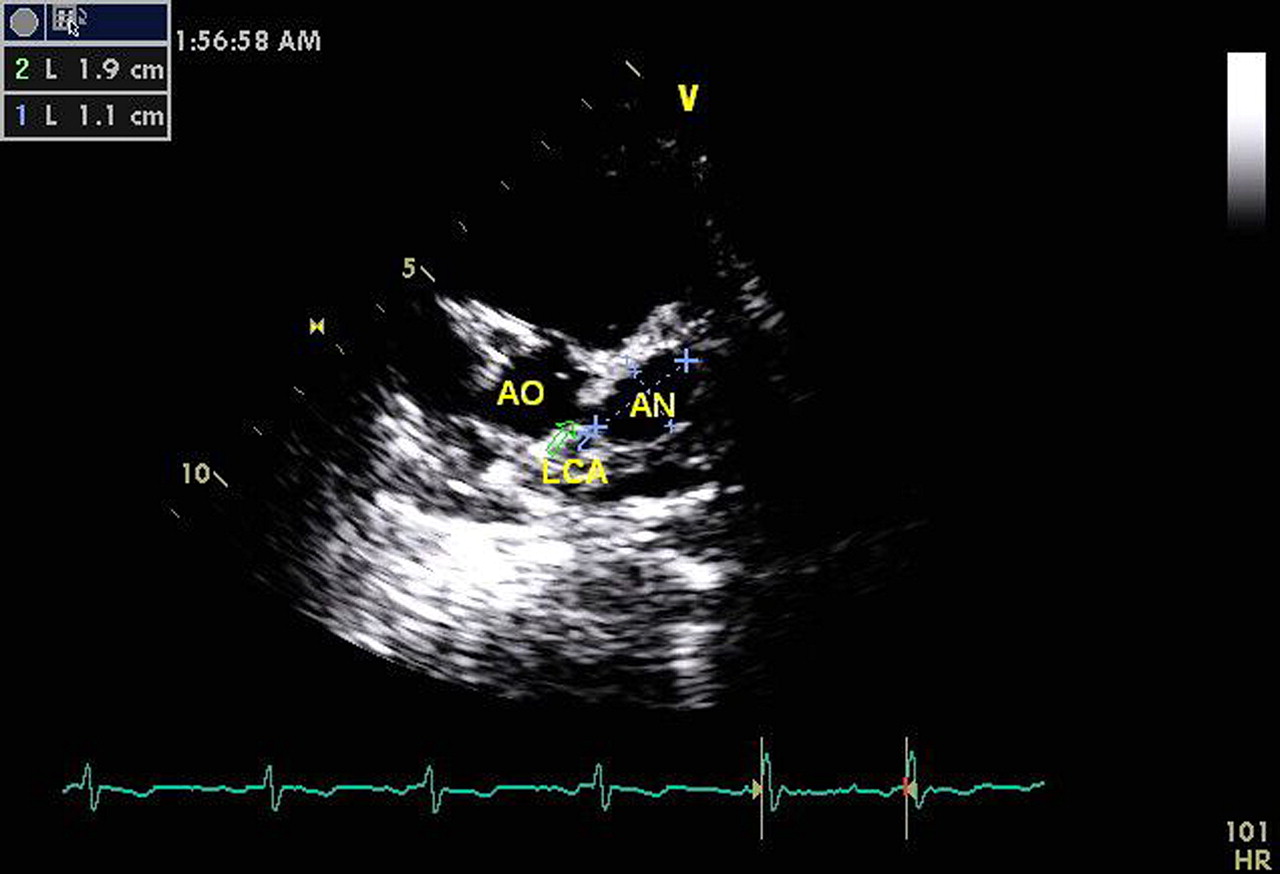
The patient was advised medical follow-up. On evaluation now at our institute, he was asymptomatic with a normal clinical examination. His ECG showed sinus rhythm, T wave inversion in V1–V5 and no significant ST changes. His chest x-ray was normal. The 2D echocardiogram revealed normal left ventricular (LV) systolic function and size and normal valves. There was a giant fusiform coronary artery aneurysm measuring 12×19 mm involving the distal left main coronary artery and proximal left anterior descending artery (figure 1). The patient underwent a coronary angiogram according to recommended guidelines,2 which showed a giant aneurysm of the distal left main coronary artery and proximal left anterior descending (figure 2). There was an additional small aneurysm involving the proximal right coronary artery. There were no areas of coronary stenosis or thrombus. As the child was asymptomatic with no increase in size of the aneurysm/stenosis, he was given aspirin, clopidogrel and warfarin. It was decided to follow-up the child by serial echocardiograms1 and coronary imaging. Giant coronary artery aneurysms are rare in Kawasaki disease and usually progress to obstructive lesions with thrombus, or have a risk of rupture or compression of cardiac structures. Hence, close follow-up and timely intervention are required.2
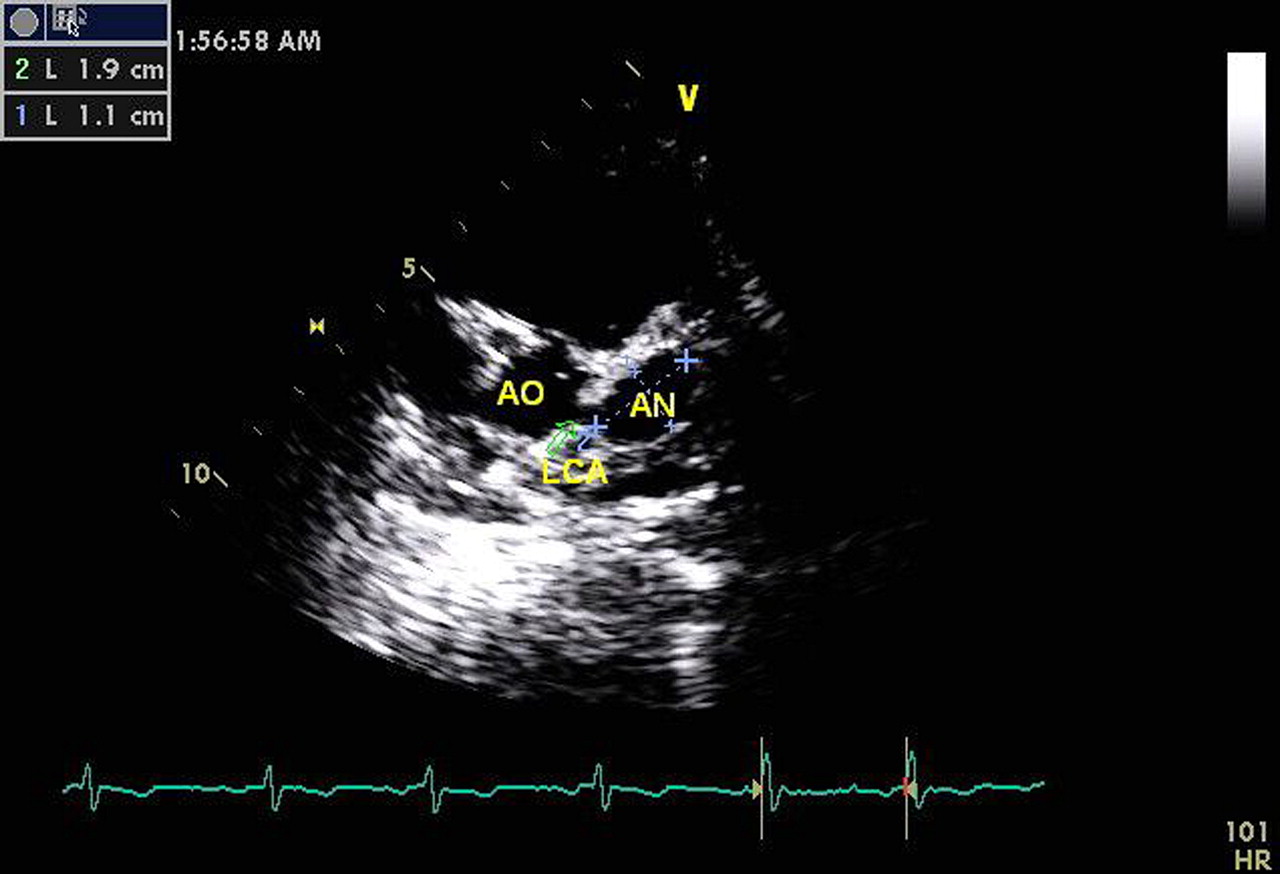
2D echocardiogram parasternal short axis view showing a giant aneurysm involving the distal left main coronary artery and the proximal left anterior descending artery. AN, aneurysm; AO, aorta; LCA, left coronary artery.

{kind=link}
{kind=link}
Coronary angiogram in left anterior oblique cranial view showing a giant coronary aneurysm of the distal left main coronary artery and proximal left anterior descending arteries due to Kawasaki disease.
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; internally peer reviewed.