Article Text

Statistics from Altmetric.com
- Congenital heart disease
- coronary artery disease
- imaging and diagnostics
- echocardiography
- electrocardiography
- ventricular tachycardia
- Fallot's tetralogy
- risk stratification
- cardiac function
- aorta
- great vessels and trauma
- arrhythmias
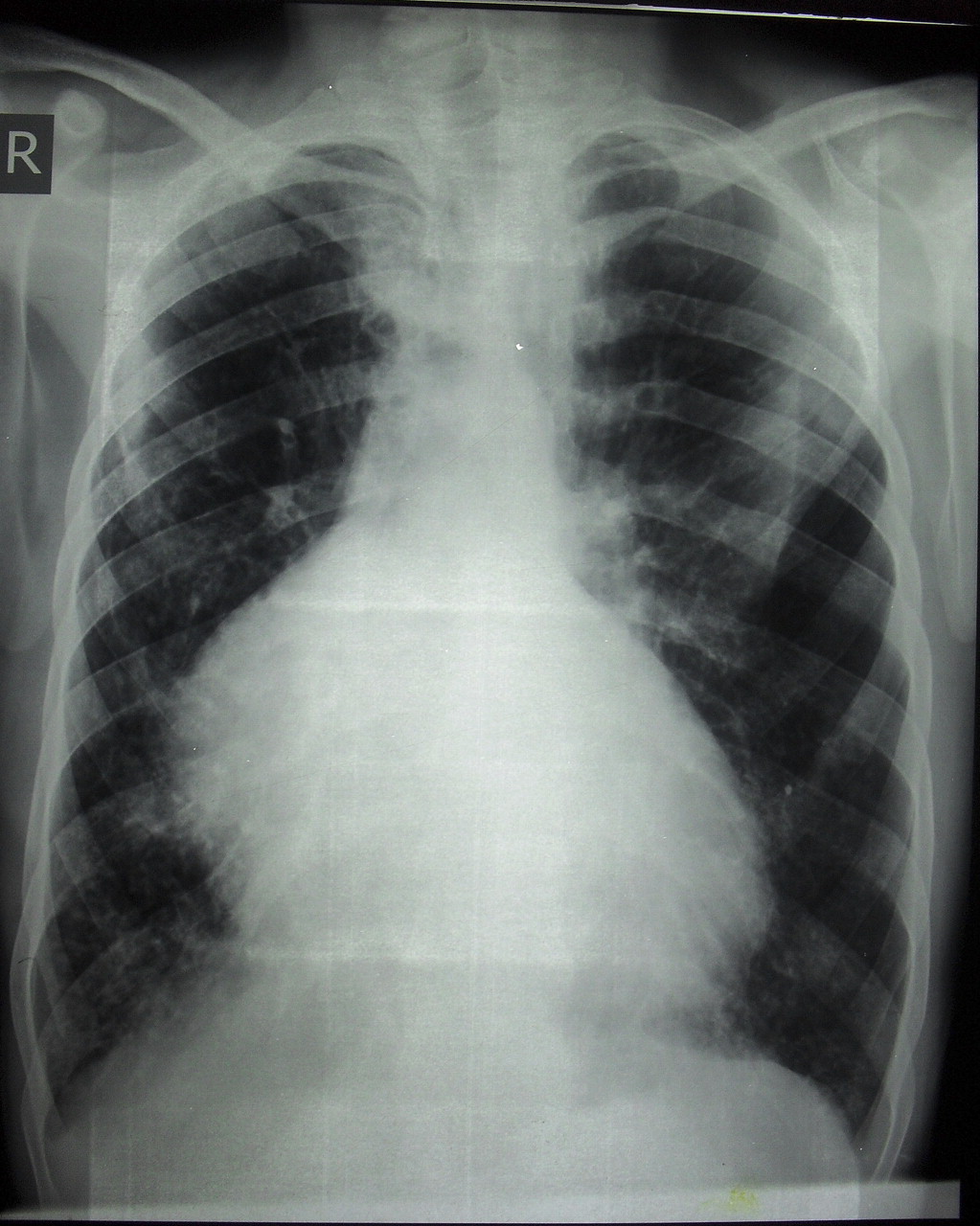
A 26-year-old man presented with progressively worsening dyspnoea on exertion since the past 6 months. He was referred to our centre with the initial diagnosis of secundum type atrial septal defect and tricuspid regurgitation (see online appendix 1) based on a transthoracic echocardiography. On physical examination, he had a systolic murmur at the left sternal border with inspiratory augmentation. Electrocardiography showed normal sinus rhythm with right bundle branch block (figure 1). Chest x-ray was suggestive of right chamber enlargement with reduced pulmonary blood flow (figure 2).


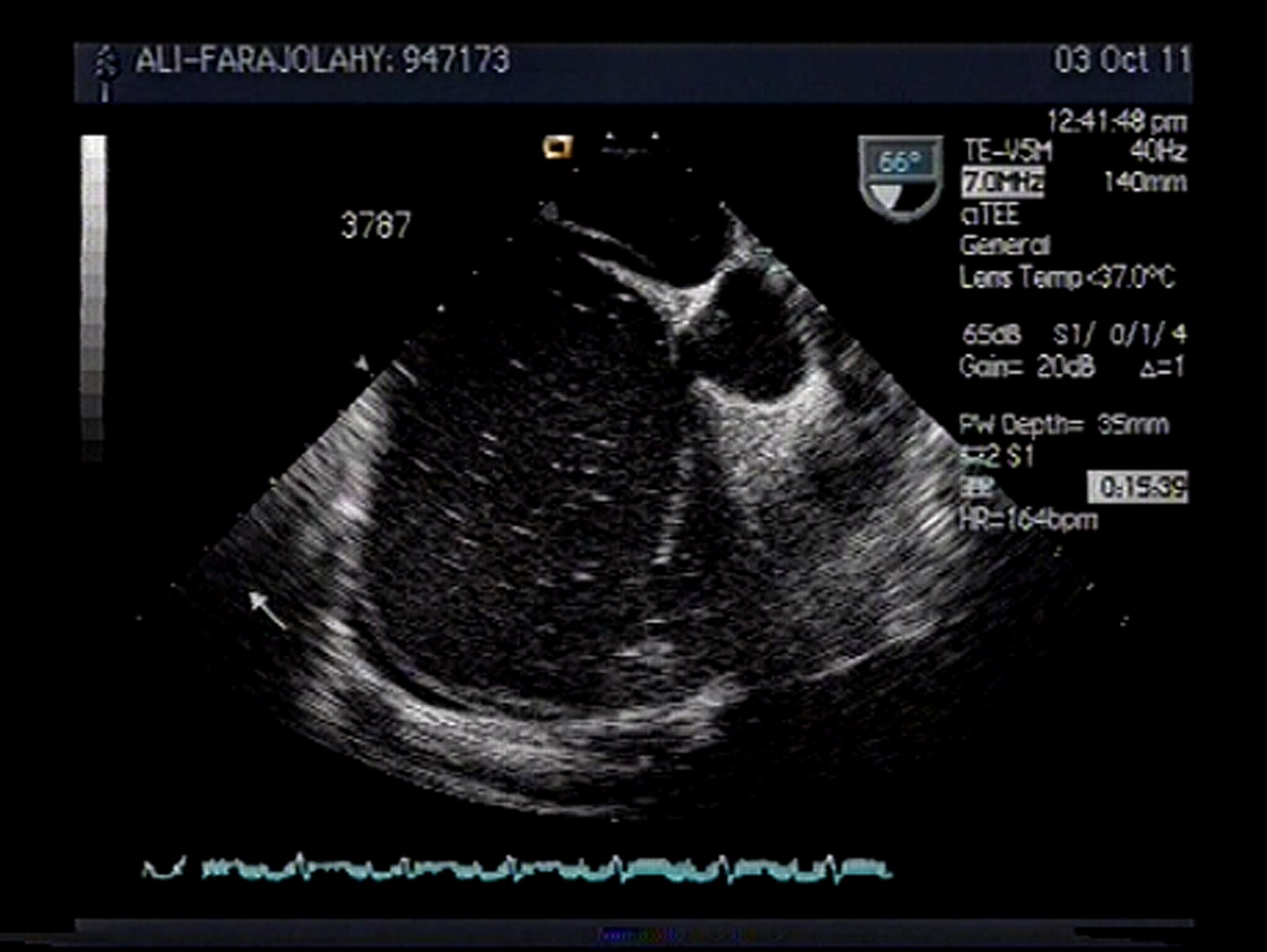
Transthoracic and transoesophageal echocardiograms revealed a normal-sized left ventricle with preserved systolic function, huge right atrium, severe right ventricular (RV) enlargement with moderate dysfunction, malcoapted tricuspid valve with Ebstein-like apical displacement (7 mm/m2) and abnormal chordal attachment of its septal leaflet resulting in severe tethering of leaflets, and severe tricuspid regurgitation. In addition, a large tunnel-shaped patent foramen ovale of 4 mm size, and significant right to left shunt was noted (figure 3).

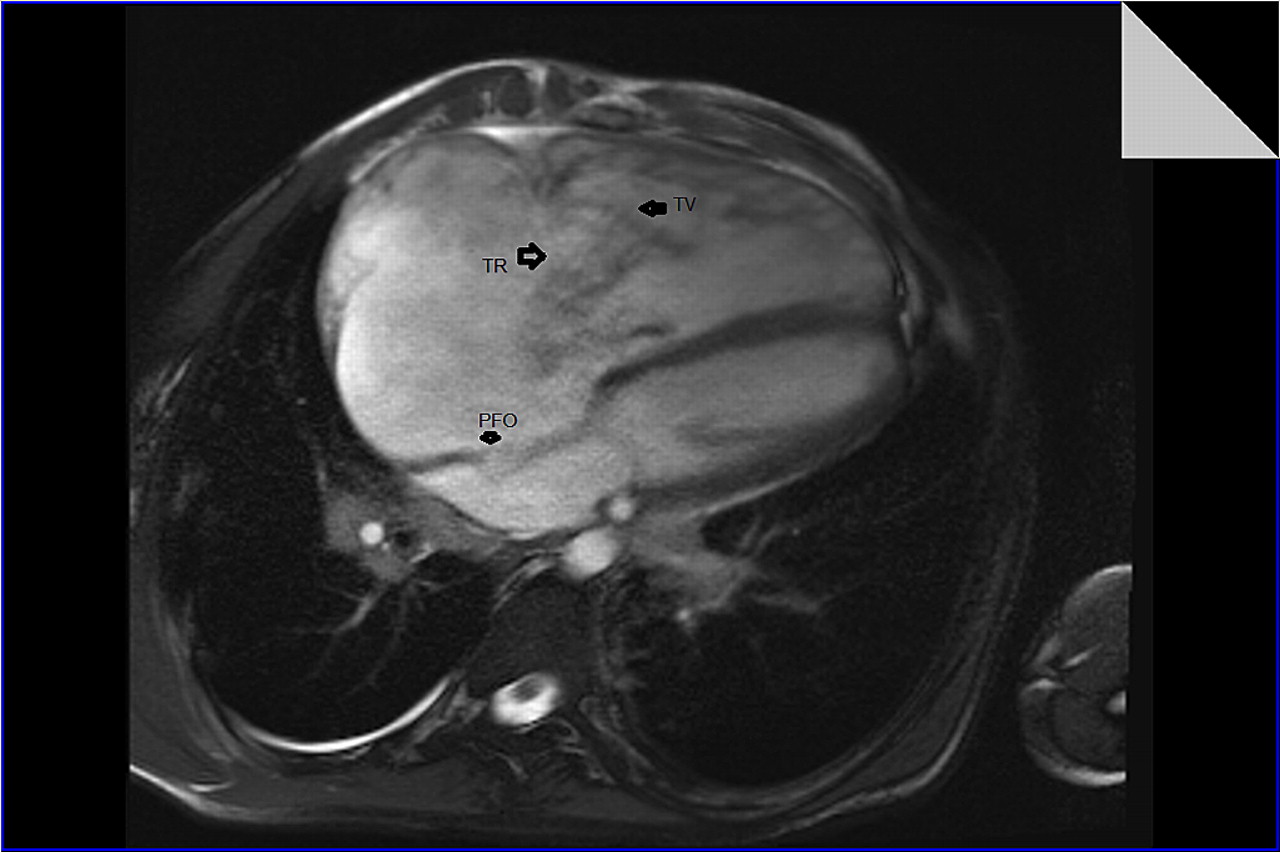
The patient underwent catheterisation, and the data were consistent with echocardiographic findings (see online appendix 2). Furthermore, haemodynamic data included normal pulmonary artery pressure, increased RV end diastolic pressure, increased right atrial pressure about 15 mm Hg and a large CV wave. The evaluation continued with cardiac MRI that depicted a severely enlarged right ventricle with prominent trabeculation and moderate systolic dysfunction, RV free wall thickness was approximately 3.5 mm and there was no RV regional wall motion abnormality. Other cardiac MRI findings included a huge right atrium and a malcoapted tricuspid valve with severe regurgitation, and no myocardial fibrofatty infiltration (figure 4 and online appendix 3).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Considering the aforementioned data, the patient was given the final diagnosis of an Ebstein-like primary tricuspid valve anomaly causing severe tricuspid regurgitation.
Diseases of the tricuspid valve are divided into primary and secondary (or functional) abnormalities. Secondary tricuspid regurgitation is much more common in adult population and is generally caused by RV dysfunction or dilation with subsequent malcoaptation of leaflets due to tricuspid annular dilatation.1 Examples include pulmonary hypertension, mitral stenosis or regurgitation, primary pulmonary diseases, left-sided heart failure, congenital heart diseases such as ventricular septal defect, and RV infarction.
Isolated involvement of tricuspid valve apparatus with subsequent significant tricuspid regurgitation is uncommon.2 Aetiology of primary tricuspid regurgitation includes congenital heart diseases such as Ebstein's anomaly, endocarditis, connective tissue disorders, carcinoid syndrome, rheumatic fever, myxomatous degeneration causing tricuspid valve prolapse, etc.
In our opinion, tricuspid regurgitation was caused by apical displacement with abnormal chordal attachment and tethering of septal TV leaflet. In typical Ebstein’s anomaly, apical displacement of septal leaflet of the tricuspid valve must be at least 8 mm/m2. Thus, our patient does not fulfil the criterion for Ebstein's anomaly. Absence of fibrofatty infiltration is against the diagnosis of arrhythmogenic RV dysplasia. Thinning of RV apex in this patient may turn our minds to the Uhl's anomaly in which there is severe thinning of the RV apex and free wall, but in Uhl's anomaly, morphology of the tricuspid valve is normal.3
References
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by the Ethics Committee, Rajayee Heart Center, Tehran, Iran.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement All unselected files from the one sent will be available to everyone.