Article Text

Abstract
Rationale Remote ischaemic preconditioning (RIPC) is a novel cardioprotective strategy that uses brief intermittent limb ischaemia to protect the myocardium and other organs from perioperative ischaemic damage. The precise mechanism through which this protective effect occurs is unknown, but potentially could be related to changes in blood-borne mediators such as cytokines.
Objective To determine whether RIPC alters inflammatory cytokine expression in a double-blind, randomised, controlled trial of patients undergoing high-risk cardiac surgery.
Methods and results Serum interleukin (IL)-6, IL-8, and IL-10 levels from 95 patients randomised to RIPC (n=47) or control treatment (n=48) were measured preoperatively, and 1, 2, 3, 6 and 12 h after cross-clamp removal. Systemic concentrations of all cytokines were increased from baseline following surgery, and, compared with simple procedures, complex surgeries were associated with significantly higher release of IL-6 (ratio of mean area under the curves 1.54 (95% CI 1.02 to 2.34), p=0.04) and IL-10 (1.97 (1.16 to 3.35), p=0.012). No significant difference in mean cytokine levels between the RIPC and control groups was detected at any time point, irrespective of the type of surgery undergone.
Conclusions High levels of IL-6, IL-8 and IL-10 are produced during high-risk cardiac surgery, and RIPC does not alter these elevated perioperative cytokine concentrations. Identification of factors that influence the ability to induce RIPC-mediated cardioprotection should be the priority of future research.
Trial registration is in the Australian New Zealand Clinical Trials Registry (http://www.anzctr.org.au; ACTRN12609000965202)
Statistics from Altmetric.com
Introduction
Ischaemia-reperfusion (I/R) injury is a major cause of myocardial and renal damage following cardiac surgery with cardiopulmonary bypass. Remote ischaemic preconditioning (RIPC) is a novel cytoprotective strategy capable of attenuating I/R injury by utilising brief periods of ischaemia in one tissue to elicit protection from subsequent prolonged ischaemic insults in other organs. Animal studies have repeatedly demonstrated the ability of this technique to reduce myocardial infarct size by up to 50% in cardiac I/R injury1 ,2; however, trials of RIPC in humans undergoing cardiac surgery have not shown such reproducible results.3 ,4 These inconsistencies have prompted a call for further research investigating the mechanisms of RIPC in order to define its clinical indication and limitations.5
There is mounting evidence that RIPC modulates the inflammatory response, suppressing pro-inflammatory gene expression in human leukocytes6 and activation of the key effector cells of postoperative tissue damage, neutrophils.7 Furthermore, the inflammatory cytokine, interleukin (IL)-6, is essential for preconditioning-induced cardioprotection in mice.8 In cardiac surgery, high levels of IL-6 and IL-8 have been associated with numerous postoperative complications, including increased myocardial damage9 and acute kidney injury,10 yet the impact of RIPC on early expression of these biomarkers has not been previously characterised. IL-6, IL-8, and other cytokines may have a direct role in the initiation of RIPC or, alternatively, function as indirect markers of preconditioning. Higher systemic levels of these mediators are associated with increasing duration and invasiveness of surgery.11 ,12 In this study, we therefore aimed to determine whether RIPC alters cytokine expression in the perioperative period in patients undergoing high-risk cardiac surgery.
Methods
We completed a double-blind, randomised, controlled trial of RIPC in 96 adult high-risk cardiac surgery patients recruited between May 2010 and June 2011. The study was registered on the Australian New Zealand Clinical Trials Registry (ACTRN 12609000965202) and received ethics approval from the Central Regional Ethics Committee (CEN/09/12/096).
Patients over 18 years of age were invited to participate if they were undergoing high-risk cardiac surgery, defined as double, triple or mitral valve replacement, coronary artery bypass graft surgery (CABG) with ejection fraction <50%, CABG+valve(s), or any redo cardiac operation. These surgeries were considered high-risk because they are generally associated with extended bypass times, or are performed in patients with significantly impaired cardiac function. For the study overall, patients with peripheral vascular disease affecting the upper limbs, or requiring deep hypothermic circulatory arrest or radial artery conduit harvesting were excluded. Additionally, for the cytokine analyses, patients receiving systemic immunosuppressives were also excluded. Written informed consent was obtained from all patients.
Patients were permuted-block randomised in groups of eight by a third party using an online randomisation sequence generator with an allocation ratio of 1 : 1 to either RIPC or control. Treatment group allocation was concealed in sequentially numbered opaque envelopes until an anaesthetic technician applied the intervention. Each participant had one tourniquet placed on their upper limb and a second tourniquet wrapped around a towel next to them on the operating table. RIPC was applied beginning with the first surgical incision by inflating the cuff to 200 mm Hg for 5 min, followed by 5 min of deflation. This process was repeated three times. For the control group, the same intervention was applied to the tourniquet wrapped around the towel. Patients, theatre staff (with the exception of the anaesthetic technician), Intensive Care Unit (ICU) staff, and investigators were masked as to treatment allocation until data collection was completed.
All patients received premedication, cardiac anaesthesia involving the use of isoflurane, tepid cardiopulmonary bypass with blood cardioplegia, and postoperative hemodynamic management, according to standardised study protocols, as described in the online data supplement.
The main clinical outcome variables were high-sensitivity troponin-T, postoperative renal injury, and ICU-support requirements, and have been reported elsewhere.13 Blood samples were collected from the radial artery preoperatively, and 1, 2, 3, 6 and 12 h after cross-clamp removal. The samples were incubated at room temperature for 30 min then centrifuged, and the serum collected for storage at −80°C until analysis. Serum concentrations of IL-1ß, IL-6, IL-8, IL-10, IL-12p70 and tumour necrosis factor-α (TNF-α) were quantified using a human inflammatory cytokine cytometric bead array (CBA) kit with an upper range limit of 5000 pg/ml, and sensitivities of 7.2, 2.5, 3.6, 3.3, 1.9 and 3.7 pg/ml, respectively (BD Biosciences, San Jose, California, USA). According to the manufacturer, the inter-assay coefficients of variation for samples at 2500 pg/ml were 11, 11, 10, 7, 9 and 13% for IL-1ß, IL-10, IL-6, IL-8, IL-12p70 and TNF-α, respectively. Patient samples were run in singlet, and standards as well as a serum sample used as a known positive control were run in duplicate for each assay. The cytokine data distribution was skewed and normality assumptions were better met with logarithm transformation, thus cytokine concentrations were log transformed and compared using t tests and analysis of covariance (ANCOVA). The exponent of the difference in logarithms shown in the results is equivalent to the ratio of mean values for the two groups. These exploratory analyses were each carried out with a type I error rate of 5%, and no adjustment was used for multiple comparisons.
Our sample size was based on power calculations performed for the main clinical end points of our study, which are described elsewhere.13 At the time our study protocol was written, there was no relevant published data on which to base a power calculation for the cytokine measurements.
Results
Perioperative serum samples from 95 patients were analysed (n=47 RIPC and n=48 control; figure 1). Randomisation appeared successful with similar distribution of baseline characteristics in the treatment groups, although there were some differences in the operative details. Five patients in the RIPC group underwent three or more procedures, whereas, no patients in the control group had more than two procedures (table 1). The main clinical outcome variables were not different between treatment groups.13 Serum IL-6, IL-8 and IL-10 levels increased considerably from baseline following surgery (see supplementary table S1). By contrast, IL-1ß, IL-12p70 and TNF-α concentrations did not increase, and were below the level of detection of the CBA (7.2, 1.9 and 3.7 pg/ml, respectively; data not shown). The inflammatory cytokines, IL-6 and IL-8, peaked between 1 and 3 h postreperfusion, and remained increased at 12 h. To reduce the incidence of type I error, statistical testing of the cytokine data was limited to the 1 and 12 h time points, which were deemed the most informative. The point estimates were consistent with the hypothesis that there are higher levels of the proinflammatory mediators present in the RIPC patients, compared with controls. However, the CIs were wide and there were no statistically significant differences in mean log IL-6 and IL-8 levels between the RIPC and control groups at 1 or 12 h (table 2), or in the total area under the curve (AUC; IL-6: ratio of means 1.32 (95% CI 0.84 to 2.05), p=0.22; IL-8: 1.17 (0.79 to 1.72), p=0.43). ANCOVA was used to determine if accounting for potential confounding variables altered the difference between the treatment groups. Adjustment for baseline interleukin levels, age, EuroSCORE-predicted mortality,14 bypass and cross-clamp times, surgery type (CABG only vs all other procedures), and statin use, did not alter the absence of a statistically significant difference in the univariate analysis (table 2). Levels of the immunosuppressive cytokine, IL-10, peaked in all patients 1 h postreperfusion and then steadily declined. IL-10 levels were similar in the RIPC and control groups (AUC: ratio of means 1.13 (0.70 to 1.80), p=0.62), and this was not affected by adjustment for confounding variables (table 2).
Demographic, clinical and operative data
Perioperative cytokine concentrations

CONSORT diagram showing the flow of participants through the trial.
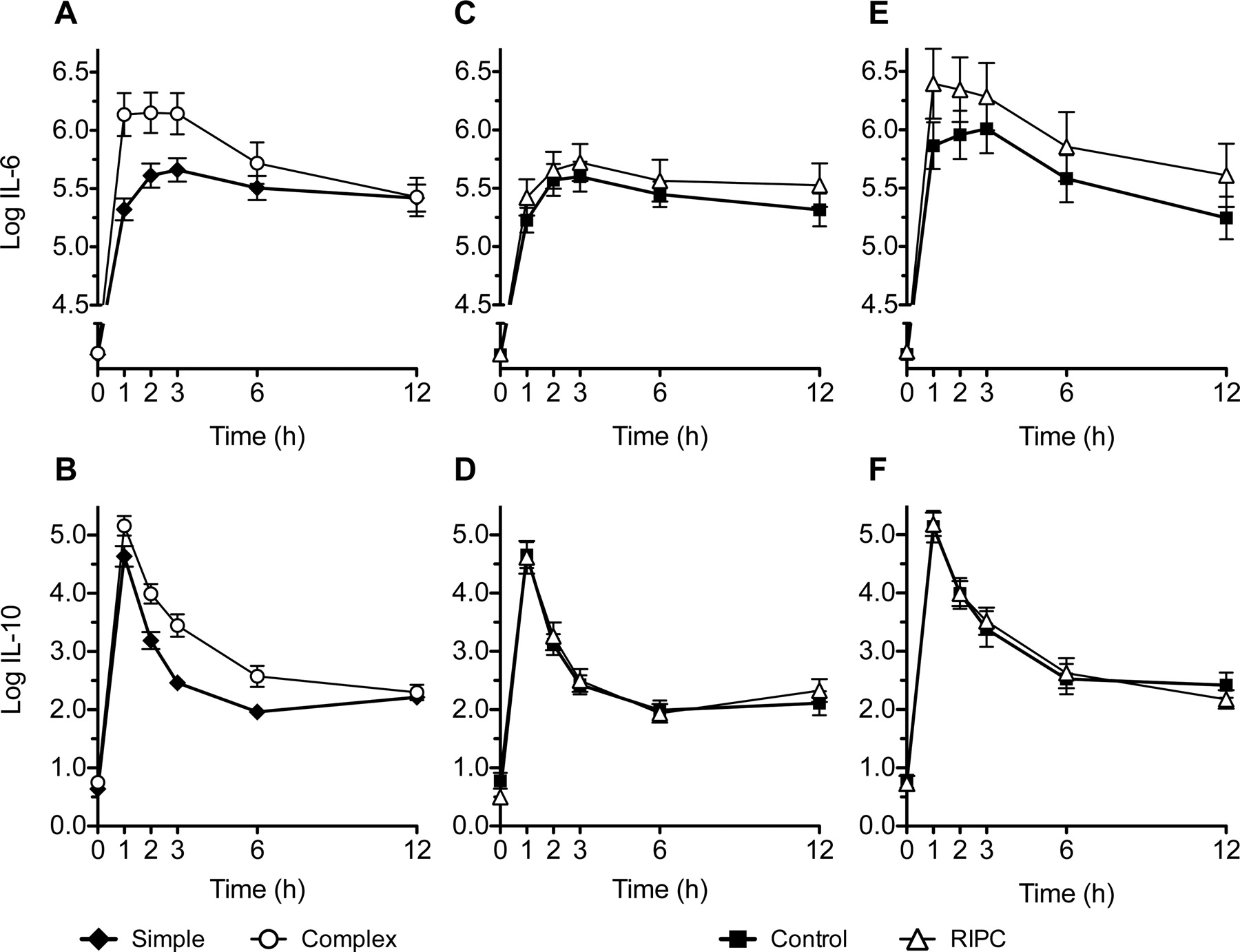
A posthoc analysis investigated whether RIPC differentially modulates cytokine expression depending on the complexity of the surgery undergone. In this study and in previous work,15 we observed that troponin release and bypass duration varied with surgical procedure. Participants were, therefore, categorised as having either simple surgery: CABG with ejection fraction (EF) <50% or CABG±aortic valve surgery; or complex surgery: Mitral valve repair with or without any other procedure. ANCOVA with baseline interleukin levels and treatment randomisation as covariates was used to compare cytokine levels. Complex surgery was associated with significantly higher levels of IL-6 (ratio of means 2.14 (95% CI 1.45 to 3.16); p<0.001) and IL-10 (1.82 (1.05 to 3.19); p=0.033) at 1 h postbypass, and in the total AUC (IL-6: ratio of means 1.54 (95% CI 1.02 to 2.34), p=0.04; IL-10: 1.97 (1.16 to 3.35), p=0.012; figure 1A,B). By 12 h, there was no evidence of a difference in the estimates (IL-6: 0.91 (0.64 to 1.31), p=0.62; IL-10: 1.08 (0.72 to 1.63), p=0.69). RIPC did not alter expression of these cytokines in either simple or complex surgeries (figure 2C–F).

{kind=link}
{kind=link}
Effect of remote ischaemic preconditioning (RIPC) on perioperative cytokine expression in simple versus complex surgery. Compared with simple surgery (n=49), complex procedures (n=46) significantly increase IL-6 (A) and IL-10 (B) release in the early postbypass period. (C, E) RIPC has no impact on IL-6 expression in simple or complex procedures, respectively. (D, F) IL-10 levels are not altered by RIPC in simple or complex surgery, respectively. Data expressed as mean±SEM.
Discussion
This study is the first to show that RIPC does not alter expression of a panel of inflammatory cytokines in high-risk cardiac surgery patients. Although the point estimates favoured the hypothesis that there were higher levels of IL-6 and IL-8 in the RIPC group, the differences were not statistically significant even after adjustment for confounding variables, such as statin use, EuroSCORE and total bypass time. Consistent with previous research,16 we confirmed that perioperative IL-6 levels are higher with complex valvular surgery compared with straightforward CABG and aortic valve replacement (AVR) procedures. In addition, we found that the release of the anti-inflammatory cytokine, IL-10, is also enhanced. A posthoc analysis indicated that RIPC did not alter IL-6 and IL-10 expression in patients undergoing simple procedures, or the more complex surgeries that are associated with higher cytokine levels. As this was an exploratory study, one limitation is that multiple comparisons were performed, and therefore it is possible that some of the statistically significant differences may represent type I error.
The precise mechanism of RIPC has yet to be fully elucidated; however, there are data supporting the hypothesis that an unidentified humoral factor transmits the protective signal from the remote preconditioned tissue to the myocardium.17 Cytokines are a prime candidate for such a factor given their function as endocrine-signalling peptides; however, our finding that RIPC does not modify expression of the key cytokines, IL-6, IL-8 and IL-10, suggests this mechanism is unlikely. This confirms previous research by Karuppasamy et al4 who showed that systemic concentrations of these cytokines were not altered following each cycle of ischaemia during RIPC application and postoperatively. One possible explanation for our findings is that the systemic cytokine levels induced by high-risk cardiac procedures are too high to be significantly altered by the RIPC treatment in this setting.
Two previous studies have reported on cytokine expression following RIPC in children undergoing repair of congenital heart defects. The first applied lower limb RIPC and reported IL-6, IL-8, IL-10 and TNF-α levels were not significantly different from the controls.18 The second, which applied RIPC both 1 day and 1 h preoperatively, found that levels of proinflammatory and anti-inflammatory cytokines were weakly attenuated postoperatively.19 Both studies differ substantially from our own in that bypass times were dramatically shorter, the earliest samples corresponded to time points after detection of the peak period of cytokine expression in our study, and the RIPC interventions were fundamentally different to the standard stimulus applied in the majority of trials, including our own, making it difficult to relate this earlier work to the present findings.
RIPC appears to afford two windows of protection that may involve different pathways. The first occurs immediately, lasting less than 4 h; whereas, the second presents 24 h after the initial conditioning.20 RIPC is most feasibly applied in surgery patients postanaesthesia, therefore, most trials, to date, including our own, have investigated the efficacy of early phase RIPC. Biomarkers of myocardial damage peak 6–8 h postbypass,15 rendering the first 12 h following surgery the most relevant period for examining factors that may modify or mediate myocardial injury. Our time points were thus carefully selected to allow us to determine whether an RIPC-induced change in cytokine expression could contribute to the protection against myocardial damage previously described in the literature. We were able to capture the period of peak perioperative cytokine release, and have shown no change in systemic cytokine levels following RIPC in the pathophysiologically relevant period.
A related study by Karuppasamy et al4 determined that RIPC does not alter levels of IL-6, IL-8 or IL-10 at 24 and 48 h following uncomplicated CABG. This study, and our own, demonstrates that IL-6 levels are not altered during early or late-phase RIPC in humans, which is intriguing given that IL-6 is considered obligatory for preconditioning-induced cardioprotection in mice.8 Furthermore, in humans there is evidence that upregulation of proinflammatory cytokines in unstable angina patients is sufficient to induce a late preconditioning effect.21 The results of these studies have two key implications. First, it is possible that the mechanism of RIPC may differ between species, and to that of classic local ischaemic preconditioning. This is supported by the recent suggestion that the cytokine-activated transcription factors associated with cardioprotection may differ between animals and humans.22 Second, contrary to the hypotheses of previous research, they suggest preconditioning would be expected to induce protection through an increase in IL-6 and IL-8 levels, rather than a decrease. Indeed, while RIPC may not alter systemic IL-6 and IL-8 concentrations, it is well established that the reperfused myocardium is a major source of inflammatory cytokines.23 The possibility that the local inflammatory milieu in the myocardium is modulated by RIPC cannot be excluded. Sampling blood from the coronary sinus may be of interest in this regard for future studies.
Our trial adds to a growing number that have not shown a clinical benefit from RIPC in adult cardiac surgery patients.3 ,4 ,24 It is possible that the absence of a clinical effect in our trial was due to the lack of change in the cytokine levels. If an increase in cytokines is essential to induce RIPC, factors that alter cytokine production, such as the use of anti-inflammatory or statin therapies,25 ,26 may influence the ability to precondition patients. Alternatively, a preconditioning effect may have been activated in all patients through secondary pathways. Our study used a standardised anaesthesia protocol that included the use of volatile anaesthetics, which have attracted attention for their ability to induce cardiac preconditioning27 ,28 and decrease inflammatory cytokine expression.29 Thus, our control group may also have been, to some extent, preconditioned. This interpretation would suggest that the marginal effect of RIPC in patients already treated with volatile anaesthetics as per our study protocol is negligible. Given the widespread adoption of these anaesthetic agents, future research is essential to clarify their relationship with RIPC.
In conclusion, we provide evidence that RIPC does not alter perioperative cytokine concentrations in patients treated with the volatile anaesthetic, isoflurane, irrespective of whether the surgeries performed are simple or complex. The priority for future research should be to identify and characterise potential factors that may alter the ability to induce RIPC-mediated cardioprotection in order to facilitate the design and interpretation of further clinical trial work.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors JW conducted the research and wrote the manuscript, PY designed and conducted the clinical trial, JP contributed to the research, MW contributed to the statistical analyses, JHM contributed to the experimental design, RB contributed to the design of the clinical trial, and ACL (the guarantor) oversaw the design and realisation of the experimental work and the final manuscript.
-
Funding This study was funded by grants from the New Zealand Lotteries Commission and the National Heart Foundation of New Zealand.
-
Competing interests None.
-
Ethics approval New Zealand Central Regional Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.