Article Text

Abstract
Background Coronary sinus blood flow (CSBF) is reduced in coronary artery disease (CAD).
Objective To evaluate the usefulness of transthoracic echocardiography (TTE) in assessing CSBF in patients with CAD.
Methods and results 232 patients with CAD, including 28 patients with acute myocardial infarction (AMI) (thrombolysed), 80 patients with unstable angina and delayed presentation MI, 80 patients admitted for coronary angiography (CAG) and 44 patients awaiting percutaneous transluminal coronary angioplasty (PTCA) were evaluated with TTE to obtain CSBF values; results were compared with those of controls. In the CAG group, the correlation between CSBF and lesion severity was assessed while in the thrombolysis and PTCA groups, CSBF levels before and after treatment were evaluated. The control group had a coronary sinus diameter of 8.73±2.08 mm and mean CSBF of 441±172 mL/min. Both the diameter and mean CSBF levels were reduced in patients with CAD. In the AMI group, patients with anterior wall myocardial infarction (AWMI) showed a greater percentage increase in CSBF after thrombolysis than patients with inferior wall myocardial infarction (IWMI). In the CAG group, patients with lower CSBF values (<300 mL/min) had more multivessel involvement, especially in patients with AWMI than in those with IWMI. In the PTCA group, patients with AWMI with initial CSBF levels <300 mL/min had a greater percentage increase in CSBF levels after stenting than patients with AWMI with CSBF values >300 mL/min.
Conclusions Non-invasive assessment of CSBF by TTE is a simple, cost-effective, imaging modality in patients with CAD, especially for risk stratification and assessing therapeutic success.
Statistics from Altmetric.com
It is well known that coronary sinus blood flow (CSBF) can be reduced in patients with coronary artery disease (CAD). Most previous studies used invasive methods or transoesophageal echocardiography for the evaluation of CSBF in patients with acute myocardial infarction (AMI).1
Methods
Our study cohort consisted of 108 patients with acute coronary syndrome (ACS), 80 patients with symptomatic CAD with a previous myocardial infarction (MI) who were admitted for diagnostic coronary angiography (CAG) and 44 patients with anterior wall myocardial infarction (AWMI) awaiting percutaneous transluminal coronary angioplasty (PTCA). There were 44 controls (normal healthy adults without CAD or CAD risk factors). In all patients and controls, the CSBF values were measured within 24 hours by transthoracic echocardiography (TTE). The study period was between September 2010 and December 2011.
AMI was defined as the presence of typical chest pain lasting >30 min with ST elevation >0.5 mV in precordial leads (V1–V6 for AWMI and II, III, aVF for inferior wall myocardial infarction (IWMI)) with creatine kinase (CK) levels more than two times the upper limit of normal. Unstable angina was defined based on the Braunwald classification.2 Demographic and comorbid conditions in all the patients and the controls were also recorded (see online supplementary table S1).
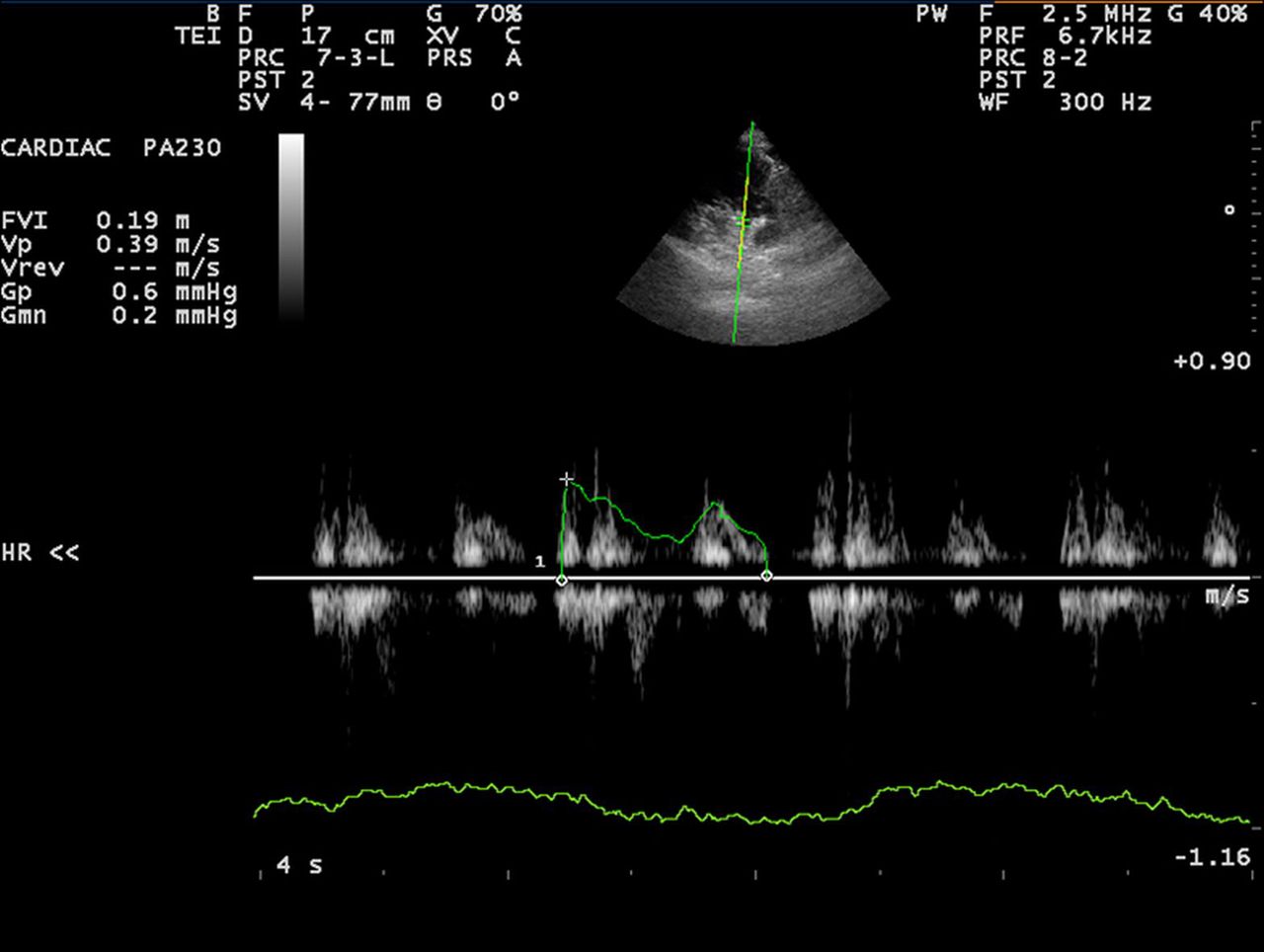
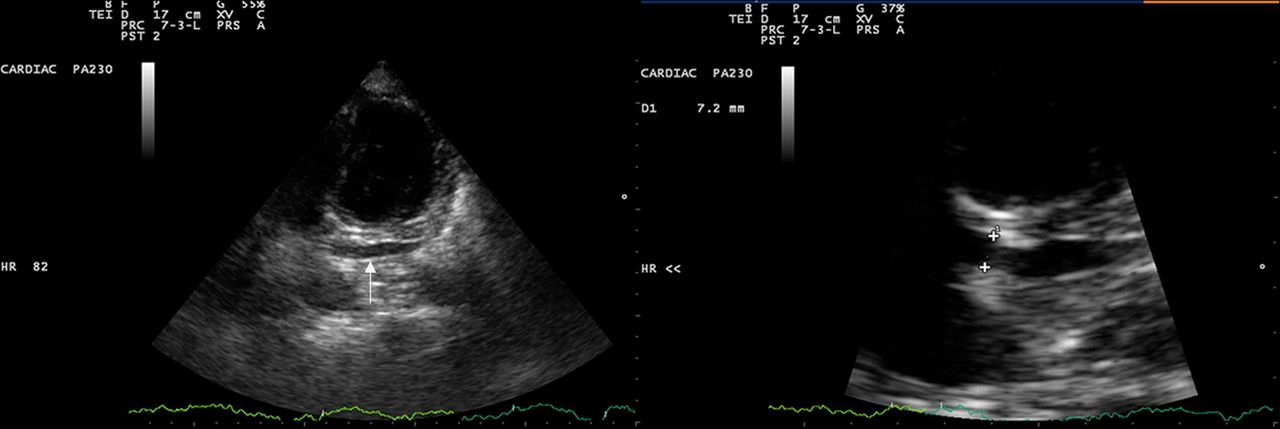
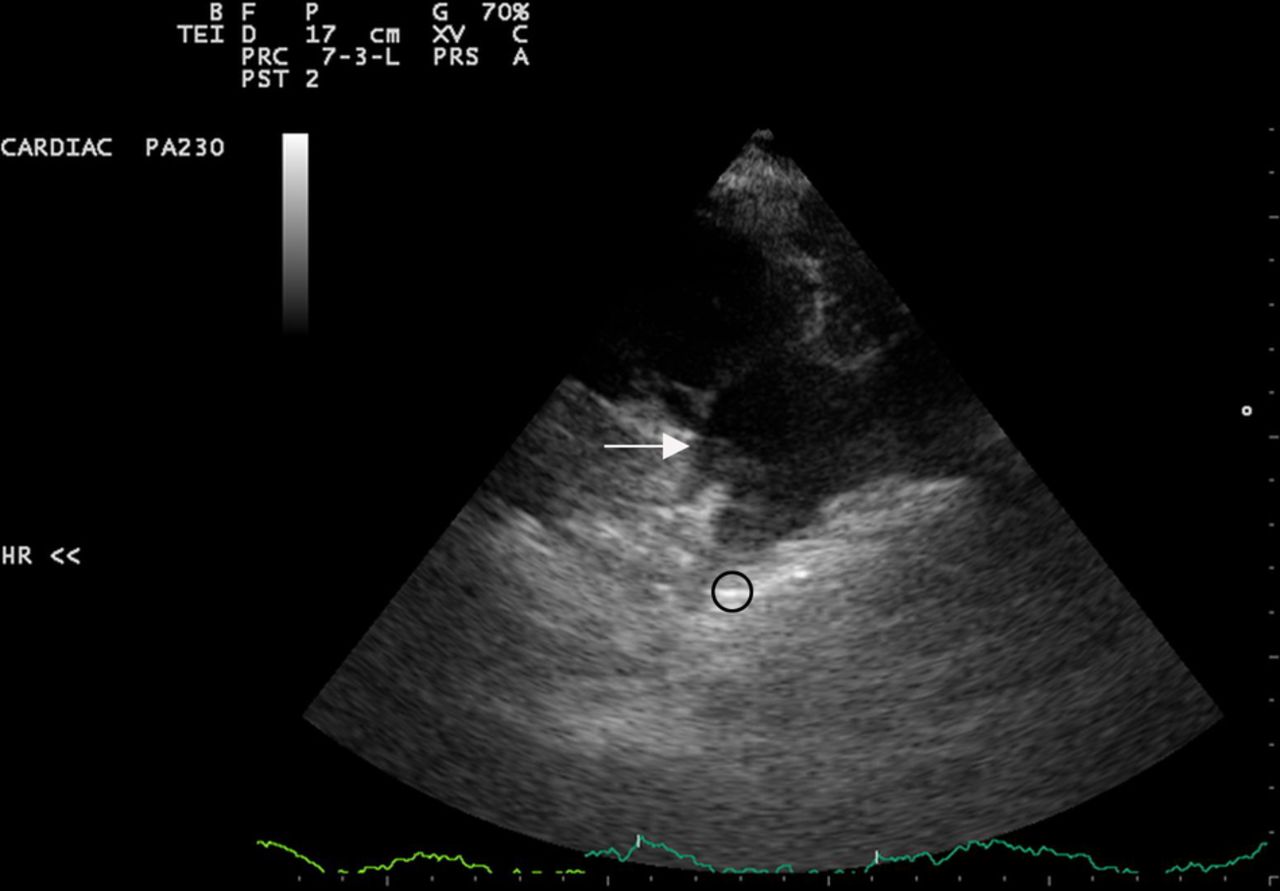
All patients underwent TTE for complete evaluation of left ventricle internal dimensions, left ventricular ejection fraction (LVEF) and CSBF parameters. An echocardiographic study was performed with a 2.5 MHz transducer using the commercially available Philips HD7 equipment. Coronary sinus (CS) diameter was measured in apical four-chamber view with slight posterior angulation (figure 1). CS flow parameters and velocity time interval (VTI) were measured using a pulse-wave sample volume kept within 1 cm of the CS opening in the right ventricular inflow view with optimised zooming (figures 2 and 3). CSBF was identified by systolic and diastolic signals, which showed very little respiratory variation, in contrast to inferior vena cava flow, which was in close proximity to the CS and showed marked respiratory variation. Assuming that the cross-section of the CS is an ellipse and that the major diameter is double the length of the minor diameter, the cross-sectional area of the CS was calculated as: (0.39 × (the major diameter)²). CSBF was then calculated as: ((CSVTI)×(cross-sectional area of the CS)×(heart rate)).3

Apical four-chamber view with posterior angulation showing coronary sinus (arrow, left panel). Optimal zooming of the above view to measure coronary sinus diameter within 1 cm of its opening into right atrium.
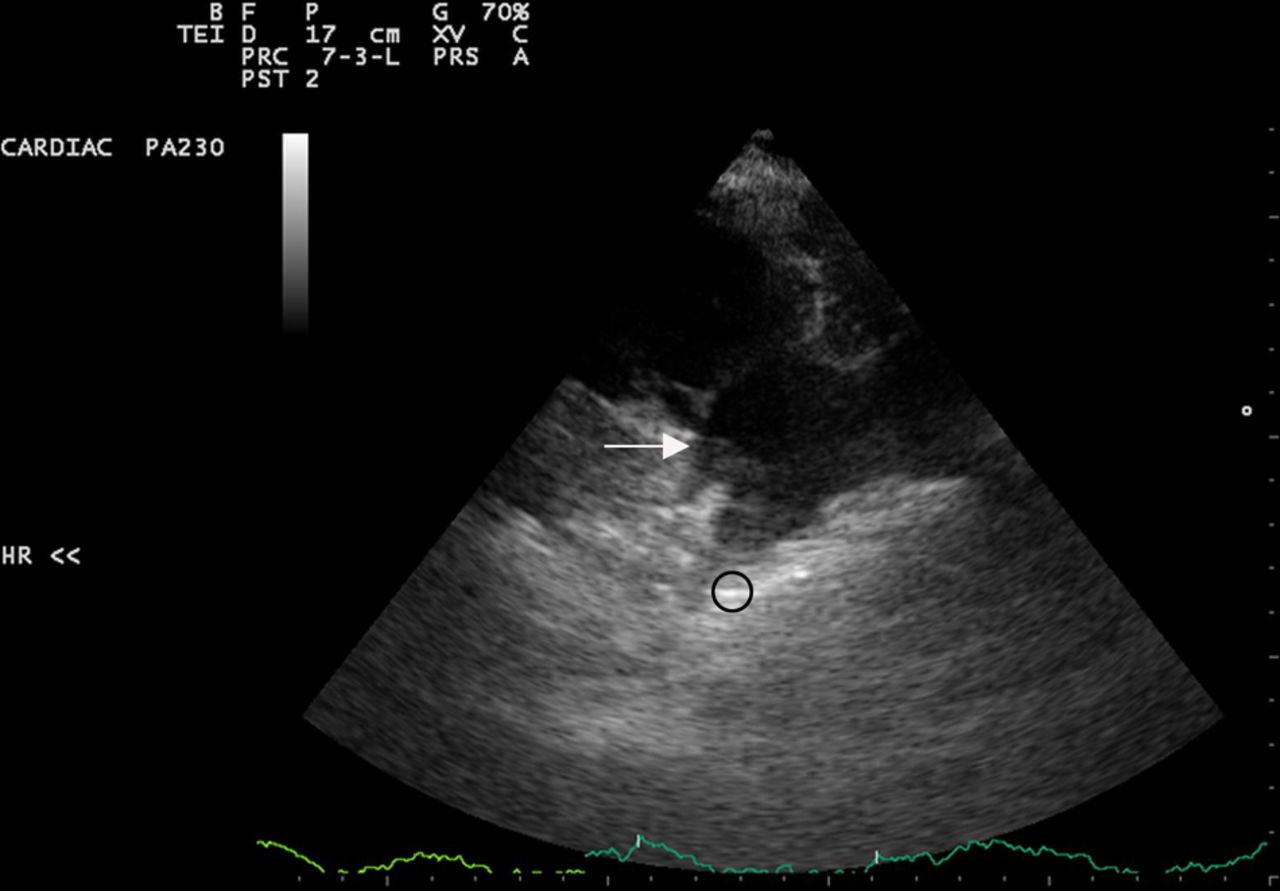
Right ventricular inflow view showing the coronary sinus drainage (arrow) close to the septal tricuspid valve leaflet. Inferior vena caval drainage is also shown (circled).
{kind=link}
{kind=link}
{kind=link}
Right ventricular inflow view with pulsed-wave Doppler sample placed within 1 cm of the opening of the coronary sinus into the right atrium. Coronary sinus flow pattern with measurement of velocity, pressure gradient and time velocity integral shown.
One hundred and eight patients with ACS were divided into two groups based on the presentation and treatment received: 28 patients with AMI, who presented early, underwent thrombolysis with IV streptokinase and were analysed for percentage change in the CSBF values before and after thrombolysis. Eighty patients had either delayed presentation of AMI (not thrombolysed), or had unstable angina and hence were heparinised. In the latter group of patients, the CSBF values were measured within 24 h of admission.
Among the 80 patients with symptomatic CAD with a previous MI who had CAG, the correlation, if any, between the CSBF values and the angiographic severity of coronary artery lesions was studied.
The 44 patients with AWMI who underwent elective PTCA with bare metal stenting were also evaluated for percentage change, if any, in CSBF, before and after PTCA with stenting.
Collected variables between the two groups were analysed using SPSS V.11.5 statistical package. Continuous parameters are expressed as mean and SD. Comparisons between the continuous variables recorded from the control and AMI groups were made by an independent samples t test. Categorical variables between the two groups were analysed with a χ2 or Fisher's exact test, as appropriate. Variables before and after thrombolysis and PTCA with stenting were analysed by one-way analysis of variance, paired t test and repeated measurement. A p value of ≤ 0.05 was considered to be statistically significant.
Results
The CS diameter was 8.73±2.08 mm for the control group, in contrast to the patients with CAD who had a smaller mean diameter (7.42±1.69 mm; p=0.0274). The CSBF per beat was 5.64±2.24 mL in the control group and 3.93±1.9 mL in the patients with CAD ( p=0.0103). The control group had a mean CSBF of 441±172 mL/min (range 280–620). So, a rounded cut-off value of 300 mL/min was taken and CSBF value <300 mL/min was considered abnormal. The mean CSBF among patients with CAD was also significantly reduced to 298.11±133.87 mL/min (p=0.0031).
Among patients with delayed presentation MI, the CSBF values were <300 mL/min in 32/36 (89%) patients with AWMI (table 1). Up to 50% of these patients had multiple risk factors such as diabetes mellitus, systemic hypertension, smoking and alcohol consumption. Compared with this, 20/28 (71%) of patients with IWMI had CSBF values >300 mL/min. The study group had 16 patients with unstable angina, with four (25%) having CSBF values <300 mL/min.
Acute coronary syndrome (delayed myocardial infarctions and unstable angina) and coronary sinus blood flow distribution
The group of patients with AMI (AWMI and IWMI) who were thrombolysed, when analysed within their group showed only a marginal improvement in the CSBF parameters after thrombolysis, which was not statistically significant (table 2). However, when patients with AWMI were compared with those with IWMI (table 3), the former showed a greater percentage increase in the mean CSBF per minute after thrombolysis (61.8±57.2% vs 8.9±6.7%; p=0.0159). The LVEF (%) also increased by an average of 1.5% after thrombolysis but no statistical significance was noted (47.57±10.78 vs 49.33±8.14; p=0.273).
Coronary sinus blood flow changes before and after thrombolysis among all patients with acute myocardial infarction (n=28)
Percentage change in coronary sinus blood flow in patients undergoing thrombolysis
Among the patients with AWMI who underwent PTCA with bare metal stenting to left anterior descending coronary artery lesions, those patients with an initial CSBF value <300 mL/min had a statistically significant increase in the CS VTI, CSBF per beat and mean CSBF per minute values after stenting compared with patients who had higher baseline CSBF values >300 mL/min (table 4). Also, the mean percentage increase in CSBF per minute was also significant in the former group compared with the latter group (37.55±35% vs 18.12±14.03%; p=0.0248) (table 5). The LVEF (%) increased by an average of 2% in the patients with CSBF <300 mL/min compared with an average increase of 1% in the patients with CSBF >300 mL/min. However, the improvements in LVEF did not show statistical significance (table 4).
Coronary sinus blood flow (CSBF) changes in patients undergoing percutaneous transluminal coronary angioplasty (PTCA) with stenting
Coronary sinus blood flow (CSBF) percentage increase after percutaneous transluminal coronary angioplasty (PTCA) with bare metal stenting in patients with AWMI
In the 80 patients with symptomatic CAD with a previous MI who underwent diagnostic CAG, the extent of disease in CAG was assessed and relationship, if any, with CSBF was also determined. All those patients with AWMI who had CSBF values <300 mL/min (total=24) had significant CAD angiographically. Eight patients each had single, double and triple vessel disease, respectively (table 6). Patients with AWMI with CSBF >300 mL/min had predominantly single vessel disease (20/36 patients) and eight patients also had normal coronary angiographies. Compared with these findings, patients with IWMI who underwent CAG mostly had normal coronaries (16/20) and 4/8 patients with CSBF <300 mL/min had single vessel disease.
Coronary sinus blood flow (CSBF) and angiographic correlation (n=80)
Discussion
The CS, located about 1 cm above, and parallel to, the left atrioventricular junction is the major venous drainage of the heart and normally measures 2–3 cm in length and 1 cm in diameter.4 The CSBF has been shown to be reduced in patients with AMI in various studies. In most of these studies, assessment was done in the cardiac catheterisation laboratory using thermodilution methods. Recently, a few studies have shown the usefulness of transoesophageal echocardiography in the assessment of CSBF in patients with AMI and patients undergoing CABG.1 ,5
Terekhov et al assessed CSBF in 42 patients using a continuous thermodilution technique in the presence of thrombolytic treatment. The coronary venous flow was shown to have increased by ≥20% in 17 patients, >30% in 15 and >40% in 10 after treatment with streptokinase.6 Bogatyrev et al by continuous CS thermodilution showed that patients with anterior MI had a significantly less blood flow in the vena cordis magna than did those with posterolateral infarction.7
Toufan et al,3 studied the use of TTE in CSBF assessment in patients with AMI and showed good correlation between measured CSBF and CS VTI by two-dimensional, Doppler TTE and LVEF, wall motion score index (WMSI), in-hospital mortality and also tissue Doppler imaging findings; they also found that CSBF and CS VTI were independent predictors in patients with AMI.
In our study also, we used TTE for assessing CSBF in patients with CAD of various categories including patients with ACS, patients with AMI undergoing thrombolysis, symptomatic patients with CAD with a previous MI admitted for diagnostic CAG and patients with AWMI awaiting elective PTCA with bare metal stenting.
In patients with ACS, the mean CSBF values were significantly lower in patients with AWMI than in those with IWMI or patients with unstable angina. Similarly, among patients with AMI who underwent thrombolysis, those patients with AWMI had greater percentage increase in CSBF levels after thrombolysis than patients with IWMI. Similarly, patients with AWMI who had initial lower CSBF values (<300 mL/min), had a greater percentage increase after PTCA than patients with higher initial values. Also, patients with AWMI with CSBF <300 mL/min had a higher incidence of double or triple vessel disease on diagnostic angiography than patients with AWMI with CSBF >300 mL/min, or patients with IWMI.
Among the two groups of patients treated (patients with MI—thrombolysed and patients with MI—with PTCA/bare metal stenting), the improvements in CSBF after treatment were associated with an increase in the LVEF (%) by an average of 1.5–2% during the hospital stay. However, statistical significance was not achieved in both the groups. Long-term follow up and serial echocardiographic assessment are beneficial in these groups.
The cut-off value of CSBF of 300 mL/min had a good correlation between significant CAD, particularly among patients with AWMI with significant CAD. Thus, simple bedside assessment of CSBF by TTE may help in predicting prognostic outcomes in patients with AMI and in risk stratification for further management.
Conclusion
Non-invasive assessment of CSBF by TTE is a potentially simple, repeatable, cost-effective, non-cumbersome imaging modality for the assessment of CSBF in patients with CAD, and especially for those with AWMI. It can also be used to assess the effectiveness of treatment in patients with CAD.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table
Footnotes
-
Contributors KM: echocardiography and study design; SS: compilation of the manuscript; RM: statistics and record maintenance.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Madras Medical College ethical committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.