Article Text

Abstract
For several decades, coronary artery bypass grafting (CABG) has been considered as the gold standard treatment of unprotected left main coronary artery (LMCA) disease. The marked improvement in technique and technology makes percutaneous coronary interventions (PCIs) feasible for patients with unprotected LMCA stenosis. The recent introduction of drug-eluting stents (DESs), together with advances in periprocedural and postprocedural adjunctive pharmacotherapies, has improved outcomes of PCIs of these lesions. Recent studies comparing efficacy and safety of PCIs using drug-eluting stents and CABG revealed comparable results in terms of safety and a lower need for repeat revascularisation for CABG. Patient selection for both the techniques directly impacts clinical outcome. Despite improvement in stent technology and operator experience, management can be challenging especially in LMCA bifurcation lesions and, therefore, an integrated approach combining advanced devices, tailored techniques, adjunctive support of physiological evaluation, and adjunctive pharmacological agents should be reinforced to improve clinical outcome.
- Allied Specialities
- Interventional Cardiology
Statistics from Altmetric.com
Introduction
Significant unprotected left main coronary artery disease (LMCA) occurs in 5–10% patients undergoing coronary angiography.1 ,2 Compared with medical treatment, coronary artery bypass grafting (CABG) of LMCA lesion has shown significant benefit.3–6 CABG has been the gold standard therapy for LMCA disease until recently. Percutaneous coronary intervention (PCI) of LMCA disease has gained popularity mainly as a result of improvement of intervention techniques and stent technology.
Importance of LMCA stenosis
The LMCA supplies 75% of the left ventricular (LV) cardiac mass in patients with right dominant type and 100% in the case of left dominant type. As a result, severe LMCA disease would reduce flow to large portion of the myocardium, placing the patient at high risk for life-threatening LV dysfunction and arrhythmias.7 It is anatomically divided into three regions: the ostium, the mid-shaft and the distal portion.8 The distal LMCA, by definition, always ends in a bifurcation, or even trifurcation, giving rise to the left anterior descending (LAD) and left circumflex (LCx) arteries, and probably an intermedius artery. Greater elastic content of this artery explains elastic recoil and high restenosis following balloon angioplasty.9 Seventy per cent of significant LMCA lesions involve the distal bifurcation. Intimal atherosclerosis in the LMCA bifurcation is accelerated primarily in area of low shear stress in the lateral wall close to the LAD and LCx bifurcation. Thus, carina is usually free of disease, which can explain why single-stent strategy can be successfully performed in patients with no or moderate disease by angiography. There are many unresolved issues to optimally treat bifurcational lesions as PCI procedures continue to evolve for this complex lesion:
-
Are increased rates of repeat revasculaisation at bifurcation versus shaft/ostial lesions
-
due to anatomical or technical factors or both?
-
Should single-stent or double-stent strategies be used routinely for bifurcations?
-
Which technique should be preferred among double-stent strategies?
-
Whether intravascular ultrasound (IVUS) is to be routinely used for the procedure?
-
What would be the optimal duration of antiplatelet therapy for patients getting distal LMCA stenting?
With the above in mind, the author reviews the evidence supporting PCI for LMCA stenosis as compared with CABG, and discusses various interventional techniques, as well as adjunctive devices and pharmacotherapy.
Evidence of PCI with drug-eluting stent in LMCA stenosis
The evolution of drug-eluting stent (DES) has been a major breakthrough in PCI of LMCA stenosis which has led to significant reduction in restenosis and target lesion revascularisation when compared with initial experiences with bare-metal stents limited by higher rates of restenosis and in some series sudden deaths.10–29
Three single-centre studies11–13 showed high procedural success rates, low procedural complication rates, and encouraging long-term outcome. The results were confirmed by the French multicentre Registry for stenting uNprotecteD LMCA stenosis (FRIEND) registry.14 DES in LMCA PCI has been evaluated in several single-centre and multicentre registries showing good safety and efficacy profile.10–12 ,16 ,19–29
Comparison between CABG and PCI with DES
To date, a large body of data from observational registries to clinical trials supports the feasibility, efficacy and safety of stenting as compared with CABG for treatment of unprotected LMCA disease. Several observational studies revealed that the early clinical events of LMCA stenting were similar or superior to those of CABG because of significant increase in periprocedural myocardial infarction (MI) or stroke in CABG patients, and that mortality between 30 days and 3 years was similar in both the groups.28 ,30–32 However, the risk of target vessel revascularisation was higher with PCI than CABG. Recent results from the MAIN–COMPARE (Revascularisation for Unprotected Left main Coronary Artery Stenosis: Comparison of Percutaneous Coronary Angioplasty vs Surgical Revascularisation) showed similar findings.28 Recent data from ASAN-MAIN (ASAN Medical Centre-Left MAIN Revascularisation) registry, demonstrated that stenting showed similar long-term mortality and rates of death, Q wave MI, or stroke.33
The evidence from randomised trials comparing CABG and PCI in LMCA disease is limited. The Study of Unprotected Left main Stenting Versus Bypass Surgery (LEMANS) trial showed a significant benefit of ejection fraction improvement and favourable clinical outcomes after PCI than after CABG.34 In the LMCA subgroup analysis from the SYNTAX (Synergy Between PCI with TAXUS and Cardiac Surgery) trial,35 PCI demonstrated the 12 month rate of major adverse cardiac or cerebrovascular events, death, MI or stroke, similar to those seen after CABG, but higher rate of target vessel revascularisation was found in DES arm.
Risk stratification for procedural and long-term outcomes
The SYNTAX score35 could be an effective tool for stratification of patients with complex LMCA disease into several levels of risk, which might decide appropriateness of revascularisation strategy. In the LMCA subgroup of SYNTAX trial, the patients with a low SYNTAX score have a higher rate of non-distal LMCA lesions with mainly isolated LMCA disease or LMCA disease associated with single vessel disease where PCI could be favoured over CABG. In contrast, the patients with a high SYNTAX score have a higher rate of distal LMCA lesions and a majority of them are associated with two or three vessels disease where CABG might stand better than PCI. Combining the SYNTAX and the EuroSCORE into a common risk model (Global Risk Classification) was correlated with a significant improvement in predicting cardiac mortality in patients undergoing PCI for LMCA.36 Another score, the New Risk stratification Score showed a higher sensitivity and specificity to predict clinical outcome.37
DES choice in treating LMCA
Few observational data and a large randomised trial (the ISAR-LEFT MAIN trial) found that sirolimus-eluting stents and paclitaxel-eluting stents were equally effective and safe in patients undergoing unprotected LMCA stenting, showing comparable risks of death, MI, repeat revascularisation and stent thrombosis.38–41 Since second generation DES show better safety and efficacy to first generation DES, the relative long-term benefits of new generation compared with first generation DES or CABG should be tested for LMCA revascularisation.
Who is the good candidate for LMCA stenting?
The first step in safely performing PCI is careful patient selection. The choice of PCI or CABG for treatment of unprotected LMCA stenosis depends on several clinical and anatomical features. LMCA disease is often associated with lesions in the other coronary arteries the treatment of which needs to be addressed when deciding on the treatment strategy of this subset and the feasibility of a complete revascularisation approach. Following are the group of patients with unprotected LMCA disease that are likely to have favourable clinical outcomes with PCI as that of CABG.
-
Ostial and/ or mid-shaft LMCA disease
-
Isolated LMCA disease
-
LMCA disease plus single-vessel disease
-
LMCA bifurcational disease treatable by single stent approach
-
Low or intermediate Syntax score (Syntax score <33)
Stenting strategies and techniques
Ostial and mid-shaft lesions
These lesions can essentially be stented as in any other artery and be stented with single-stent strategy with good immediate and long-term outcomes.
Careful imaging must be performed to ensure adequate visualisation of the ostium and adjacent aorta. Usually anterior-posterior cranial and (or) slightly left anterior oblique cranial projections give the best view. The guide catheter may be occlusive with severe stenosis. After the angioplasty wire is in position in the distal vessel, the guide should be disengaged slightly from the ostium by pushing gently on the wire. This will minimise coronary ischaemia. The guide can then be gently moved towards the ostium, by slight traction on the wire, to allow contrast injection and imaging. The guide catheter should be short-tipped with side holes. The Amplatz guides should be avoided in ostial lesions. Ostial lesions are often predilated. The stent needs to be placed carefully with 1–2 mm protruding into the aorta. After deployment, the balloon should be withdrawn slightly into the aorta and the proximal part of the stent postdilated to flare it which ensures good stent apposition at the ostium. IVUS may be used to ensure a satisfactory result.
LMCA bifurcation lesion
Distal LMCA lesions are mostly treated as true bifurcation. The exception to this is when one branch is small (usually the LCx), when one branch is chronically occluded or if protected by a patent graft. In these circumstances the distal lesion may be addressed with a single-stent technique across the ostium of the other vessel. True bifurcation lesions may be treated either by single-stent or by a two-stent strategy. Choice of strategy depends on vessel and lesion characteristics (plaque distribution, the diameter of the branches, the angle between them and anatomy of side branch). The provisional stenting is a single-stent strategy, although it allows the placement of a second stent if required (T, T and protrusion (TAP), culotte technique). More complex lesions may require double-stent strategy (T stenting, TAP, mini-crush, culotte, V stenting).
Strategic mapping
In deciding the strategy, the size of the side branch (SB), which is always LCx and anatomy of the ostium are two important features. The size of the LCx and the anatomy of the ostium are two important features. If the LCx is either occluded, its diameter <2.5 mm, it can be ignored and a stent can be placed between the LMCA and the LAD.42 A wire placed in a small LCx may help to maintain flow after a single stent is placed across the ostium. For a non-diseased LCx ostium, if the angle of bifurcation is of T shape, it is the operator's choice to place a protective wire but it is often not necessary. However, if the bifurcation angle is of Y shape, a protective wire is recommended. For a significant and diseased LCx ostium, there are several techniques depending on the angle of bifurcation, if the angle is of T shape, the T-stent or mini-crush kissing stent technique is recommended whereas if the angle is of Y shape, the culotte, mini-crush or Double Kiss (DK) crush technique is recommended, while T stenting is not.43
When double stents are used, a final simultaneous inflation of both stents (kissing balloon inflation) at medium pressure (8–10 atm) with non-compliant balloons is considered critical to optimise outcomes. Whatever technique is chosen, a final examination using IVUS should be performed to ensure adequate stent expansion, complete stent strut apposition to the vessel wall, and absence of peristent dissection.
Single-stent strategy
The provisional T-stenting
This is a single-stent strategy but allows the positioning of a second stent if required (figure 1).

Provisional stenting. (A) Baseline angiogram showing tight distal left main (LM) lesion with near normal (left circumflex) LCx ostium. (B) Intravascular ultrasound (IVUS) showing severely diseased left anterior descending (LAD) ostium. (C) IVUS revealing minimally diseased LCx ostium. (D) Stenting left main coronary artery (LMCA-LAD) crossover. (E) In-stent dilatation with bigger non-complaint balloon. (F)Final result after kissing balloon inflation. (G) IVUS showing well expanded stent at LAD ostium. (H) No carina shift from main branch stent as reflected by IVUS.
The LAD and LCx are wired. A stent is positioned from LMCA to the LAD to fully cover the lesion and then deployed at 12–14 atm. The wires are then exchanged, the LAD wire can be withdrawn and passed through the stent struts to the LCx, and the ‘jailed’ wire in the LCx can be withdrawn and advanced to the LAD. High pressure postdilatation may be applied if it is necessary. If the ostium of the LCx is compromised, a kissing balloon technique can be performed. If the ostium of the LCx is severely compromised, the provisional T stenting, TAP or culotte technique may be applied. Final kissing inflation (FKI) is performed if two stents have been used.
Double-stent strategy
The culotte stenting
This technique is suitable for lesions where ostium of LCx is diseased, the angulation between LAD and LCx is <60° and when two vessels are of similar diameter. The main branch (MB) usually the LMCA-LAD is stented. The LCx is rewired through the stent struts and dilated. A second stent is advanced through the struts of the first into the side vessel. The LMCA-LCx stent is deployed. Each limb of the culotte is dilated at high pressure (16 atm) using non-compliant balloon followed by FKI at 8–12 atm (figure 2). This technique gives near-perfect coverage of the carina and SB ostium. The main disadvantage of the technique is that rewiring both branches through stent struts can be technically demanding, and time-consuming. Open-cell stents are preferred for this technique.

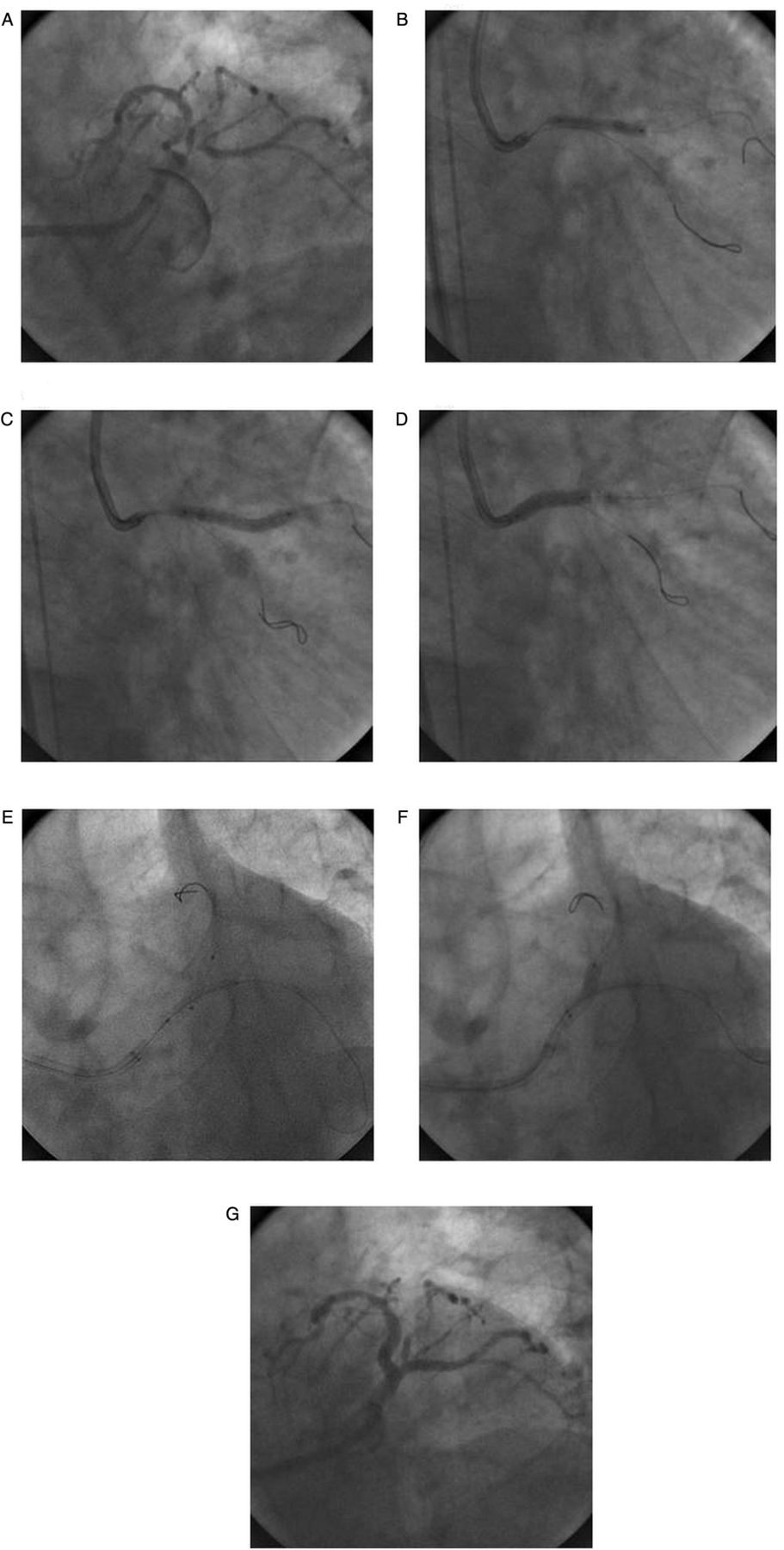
Culotte stenting. (A) Baseline angiogram. (B) Predilataion of left main-left anterior descending (LM-LAD) artery. (C) First stent deployed in LM-left circumflex (LCx) artery. (D) Second stent deployment in LM-LCx artery after wire exchange and predilation. (E) Kissing balloon inflation. (F) Final result.
The classical T stenting
This technique is suited when the angle between the two vessels is close to 90°. A stent is deployed in LCx, making sure to cover the ostium with minimal protrusion into the LAD. The LMCA- LAD lesion is then stented. LCx is rewired and dilated followed by FKI. This technique provides good reconstruction of distal LMCA bifurcation, but is associated with the risk of leaving a small gap between the branches, hence restenosis at the ostium of LCx. For this reason, this technique has largely been replaced by the modified T stenting technique. The T technique is most frequently used to cross over from provisional stenting to stenting the SB.
The modified T stenting
It is a variation performed by simultaneously positioning stents at LCx and LAD with LCx stent minimally protruding into the LAD, when the angulations between the branches approach 90°. The LCx stent is deployed first, and then after removal of the wire and balloon from LCx, the LAD stent is deployed. The procedure is completed with FKI.
The T and protrusion (TAP) stenting
This modification of the T stenting technique can be used in majority of the bifurcation lesions. It can provide good reconstruction of distal LMCA bifurcation with minimal stent overlap.
The MB (LMCA-LAD) is stented jailing the SB (LCx) wire. Kissing balloon inflation is performed after rewiring the SB. After positioning the proximal edge of the SB stent 1–2 mm inside the MB stent, the SB stent is deployed at high pressure with deflated balloon kept in the MB stent. Then, SB balloon is slightly retrieved and aligned to the MB balloon. Afterwards, a FKI is performed in order to reshape the carina (figure 3).

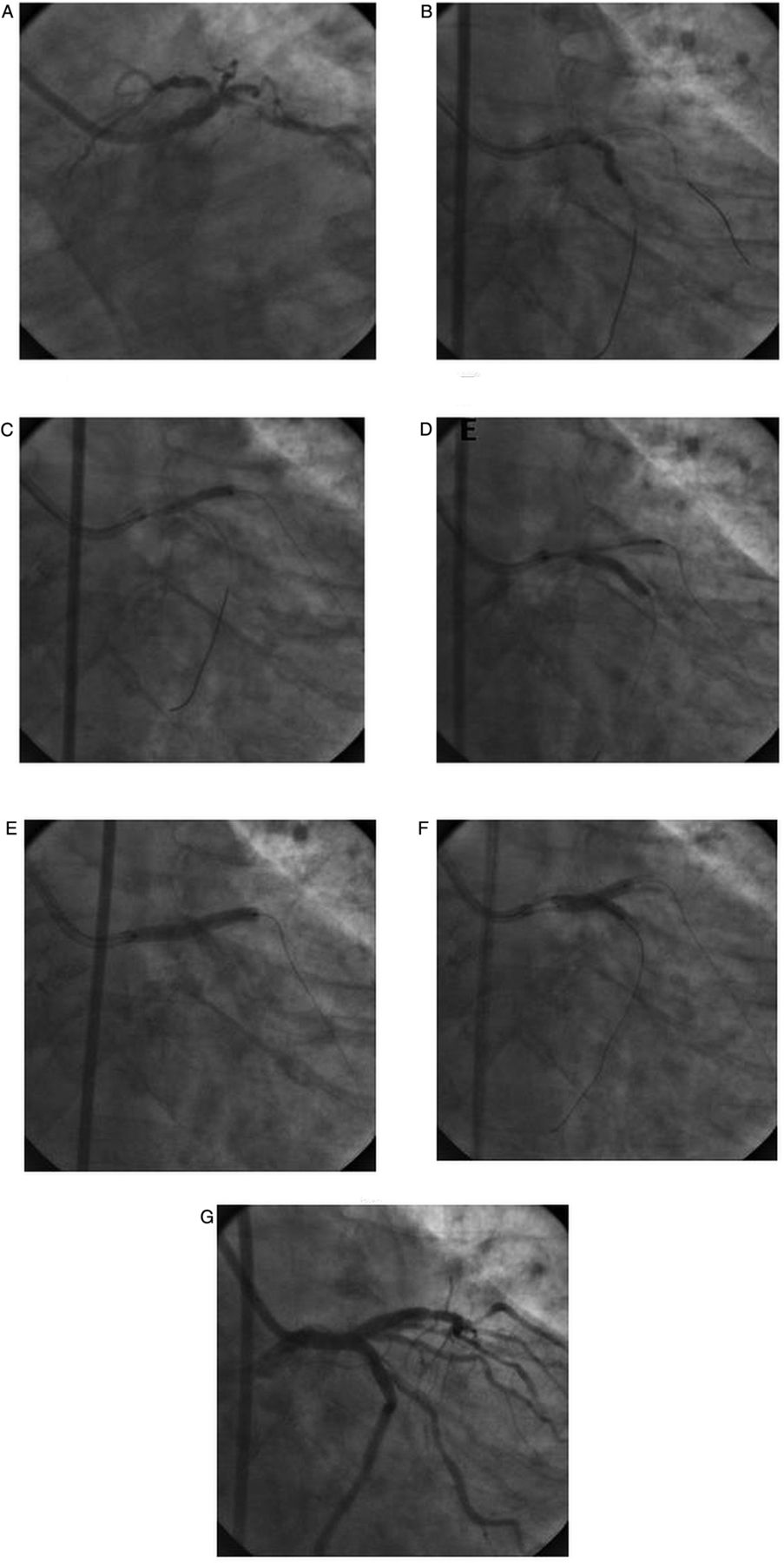
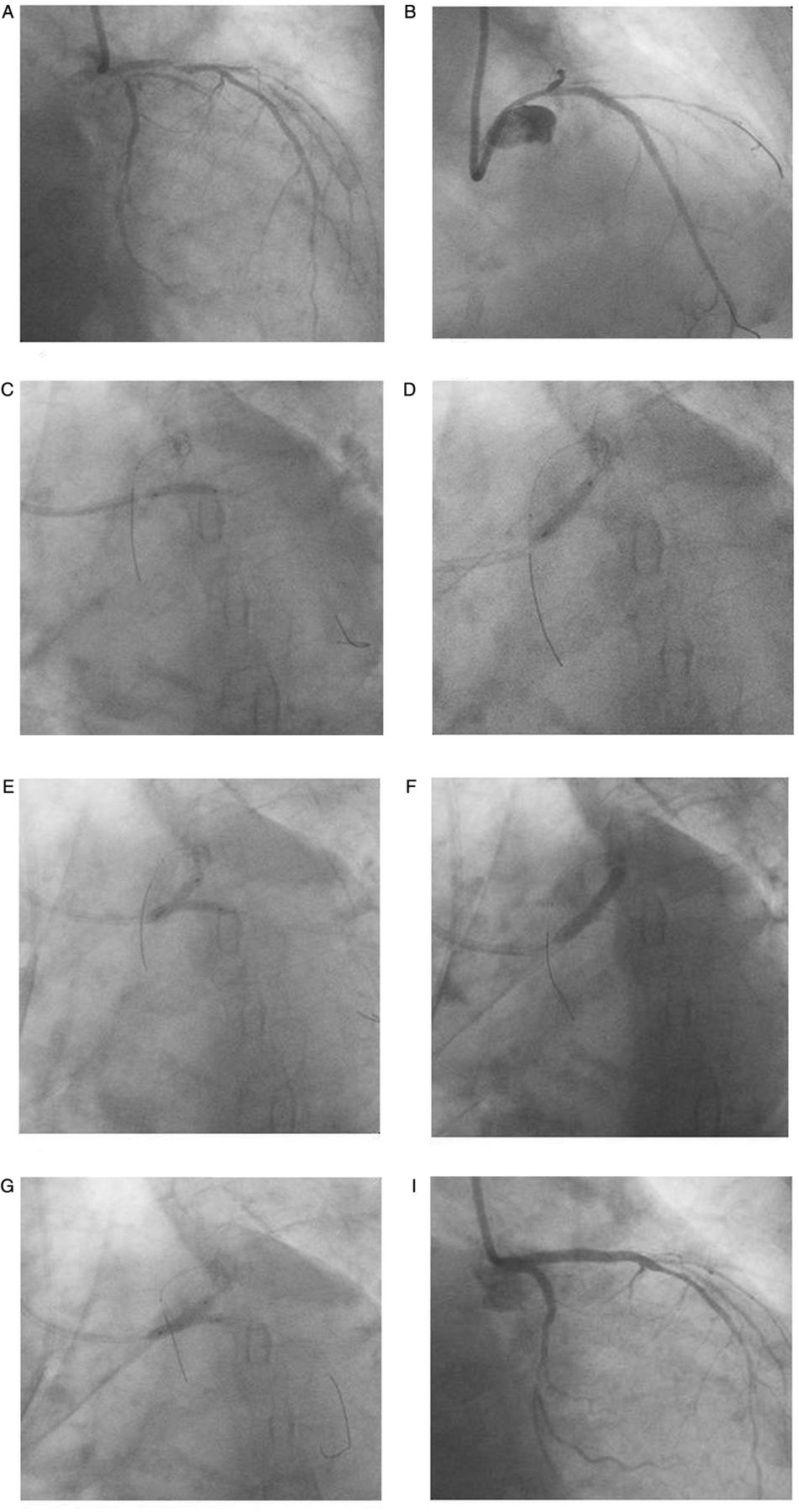
T and protrusion technique. (A) Baseline angiogram showing significant stenosis of ostium and distal trifurcation of left main (LM), ostioproximal left anterior descending (LAD) and left circumflex (LCx). (B) Predilataion of LAD and left main coronary artery (LMCA) with 3.0X20 mm balloon. (C) 3.5×23 mm drug-eluting stent (DES) implanted at proximal LAD. (D) Implantation of 3.5×18 mm DES into LM-LAD artery. (E) After predilation of LM-LCx artery with 2.5×20 mm balloon through stent struts, implantation of 2.75×18 mm DES in LCx with proximal edge inside LM and deflated 3.5×18 mm balloon in LM artery. (F) Final kissing balloon inflation. (G) Final result.
The mini-crush stenting
The mini-crush technique is suitable for LM bifurcation for a patient with ostial and proximal stenosis of the MB (LAD) and SB (LCx), in which the diameter of LAD is greater than LCx and the angle between LAD and LCx is less than 60°. The immediate patency of both branches is assured and therefore it should be used in conditions of instability or complex anatomy. This technique provides excellent coverage of the ostium of the SB. This technique can be used in almost all true bifurcation lesions but must be avoided in wide angle bifurcations. The main disadvantage is that in order to perform FKI, there is need to recross multiple struts with wire and a balloon.
The SB stent is positioned in the SB followed by advancement of MB stent. The SB stent is pulled back into the MB about 1–2 mm and is deployed at least at 12 atm. The MB is stented at high pressure, usually above 12 atm that crushes the proximal SB stent against the LMCA wall. LCx is rewired through the stent struts of LAD and crushed LCx stent to perform FKI (figure 4).
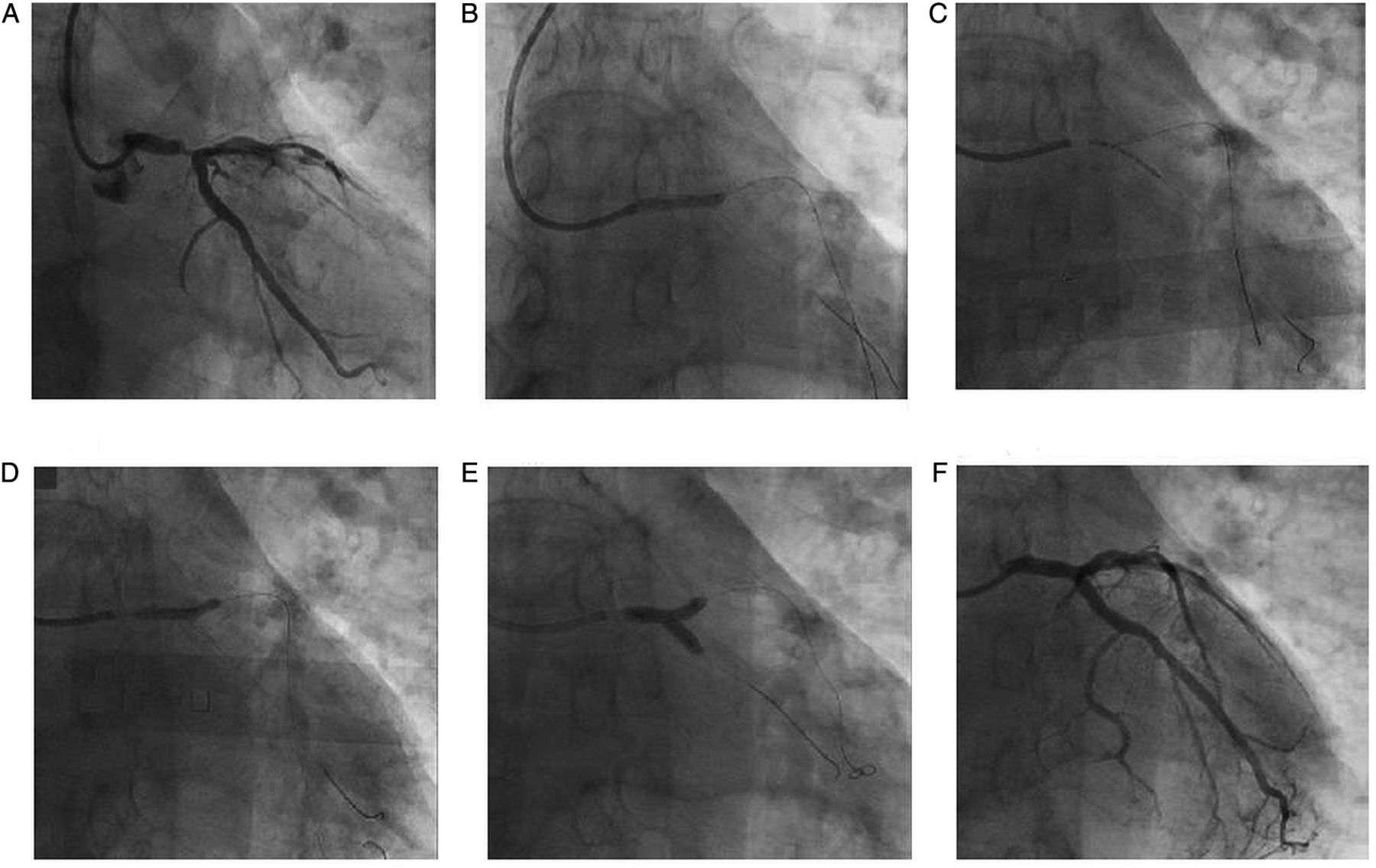
Mini-crush technique (figure 4 in new folder). (A) Baseline angiogram revealing significant stenosis of left-main (LM) bifurcation involving proximal left anterior descending (LAD) and left circumflex (LCx) artery. (B) Predilatation of LCx artery. (C) Predilatation of LAD artery. (D) Stent to LCx with protrusion into LAD artery. (E) Crushing of LCx stent with left main coronary artery (LMCA) to LAD stent. (F) Rewiring of LCx followed by final kissing balloon inflation. (G) Final angiographic result.
The DK crush stenting
A stent is placed into LCx and a balloon placed in LMCA-LAD. The stent and balloon are positioned as in the standard crush technique. The LCx stent is deployed and then the wire and balloon from the LCx are removed. The prepositioned balloon in LMCA-LAD is inflated to crush the protruding segment of LCx stent against the vessel wall of the LM. The balloon is removed and a stent is deployed in the LMCA-LAD. The wire is then recrossed into the LCx and FKI is applied to finish the procedure (figure 5). DK Crush technique results in less stent distortion, improved stent apposition, and facilitates FKI. It may be superior to classic crushing optimising acute procedural results and possibly improves clinical outcomes by facilitating FKI.44 DK-CRUSH II is the only randomised trial to suggest that double stenting may be superior to provisional stenting and associated with a lower rate of restenosis and repeat revascularisation.45
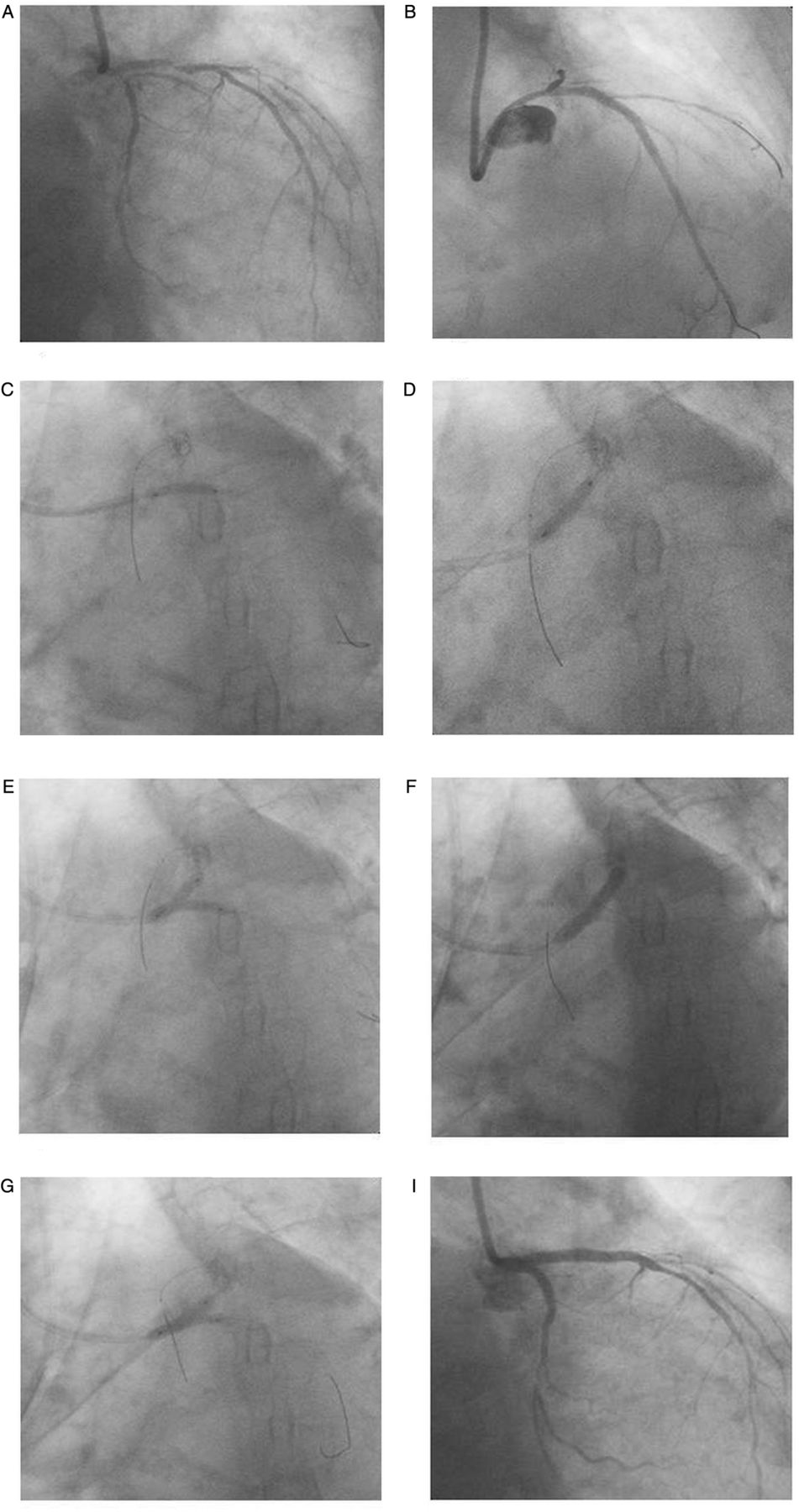
Double kiss crush technique. (A) Baseline angiography showing critical distal left main (LM), proximal left anterior descending (LAD) and ostioproximal left circumflex (LCx) artery. (B) Predilatation followed by stenting of proximal LAD. (C) Predilatation followed by subsequent stenting of LM-LCx. (D) Crushing of LCx stent with non-compliant balloon placed in LM-LAD artery. (E) First kissing balloon inflation. (F) Deployment of stent from LM-LAD with second crushing of LCx stent. (G) Second kissing balloon inflation. (H) Final result.
The V and the simultaneous kissing stent (SKS)
The V and SKS techniques are performed by placing and deploying two stents together.46 ,47
Wires are placed in LAD and LCx, with or without predilatation, The two stents are placed into the LMCA and the respective branches and deployed by simultaneous inflation. Some operators allow a variable amount of protrusion creating a rather long double barrel; the technique is called SKS. The main advantage of this technique is that access to both branches is always preserved with no need for rewiring. V stenting is relatively easy and fast and thus ideal in emergencies. It is indicated in patients with a short LMCA-free disease and critical disease of the LAD and LCx ostia. Proponents of the SKS technique are of the view that it can be performed even if the LMCA is long and has significant disease that extends into the bifurcation. SKS can also be applied when the LMCA is very large resulting in a significant diameter mismatch with the LAD and LCx, as this technique will ensure apposition and full coverage of the large LMCA with drug (figure 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
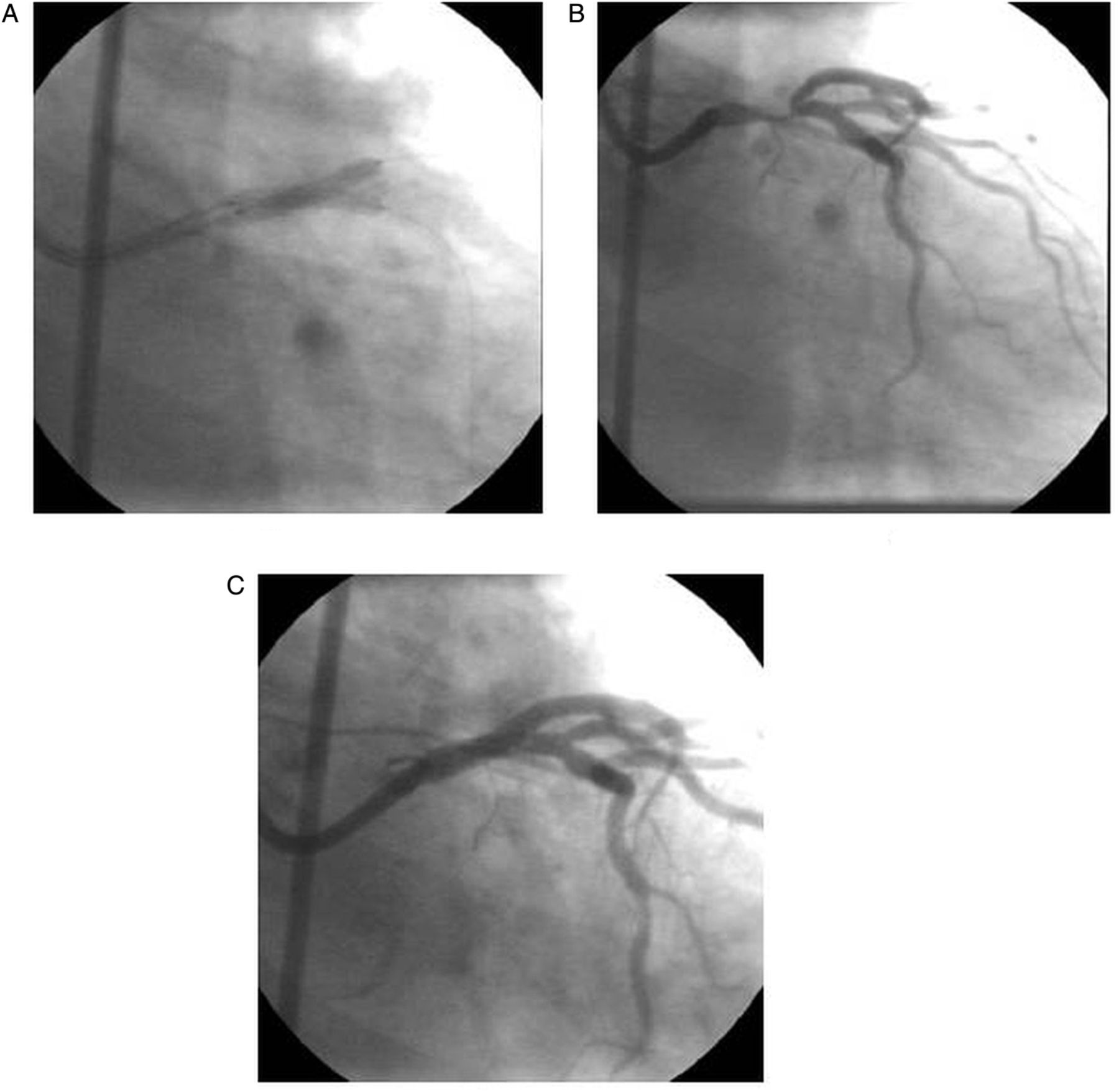
Simultaneous kissing stent technique (figure 6 in new folder). (A) Baseline angiogram showing tight stenosis at left main (LM) bifurcation. (B) Implantation of two drug-eluting stents (DES) in left anterior descending (LAD) and left circumflex (LCx) artery simultaneously. (C) Following sequential postdilatation and kissing balloon inflation.
Primary PCI in patients with LMCA occlusion
Limited data are available on patients undergoing primary PCI of LMCA. Clinical presentations of acute LMCA occlusion are usually catastrophic and include cardiogenic shock with severe LV dysfunction, malignant arrhythmia, pulmonary oedema, and acute respiratory failure requiring mechanical ventilator support. These patients unlike other forms of acute myocardial infarction, have high inhospital mortality and morbidity because of LV pump failure. With acute LMCA occlusion, haemodynamic deterioration usually follows quickly and sudden death may ensue. It is also impossible for us to identify an acute LMCA occlusion until the patients are in the catheterisation laboratory undergoing coronary angiography. Therefore, there may not be enough time for emergency CABG in this setting. Primary PCI can offer immediate restoration of coronary flow in such cases and saves lives. Every effort should be made to decrease the time from the first medical contact to balloon inflation. Intra-aortic balloon pump (IABP) should be implemented before or immediately after urgent coronary angiography prior to PCI. Such strategy may reduce adverse events such as incidence of ventricular tachycardia/fibrillation and need for cardiopulmonary resuscitation during the intervention. Simple catheter thrombus aspiration instead of standard balloon predilatation has been shown to improve microvascular reperfusion. One must avoid stent oversising and high-pressure postdilatation to avoid ‘slow’ or ‘no-reflow’ phenomenon, which may be detrimental especially for a patient in a cardiogenic shock with LM occlusion.
Adjunctive management
IVUS and optical coherence tomography
IVUS is the ideal method for confirming the presence of significant LMCA lesion and also for stent size, assessing the presence of calcification, and documenting the involvement of the distal LMCA and its branches. Knowledge of reference lumen diameter, plaque composition and position of the carina in relation to the major portion of the plaque volume are vital information prior to PCI of LMCA.43 It is also considered to be a useful modality in selecting treatment strategy, and helpful in optimally expanding the stent, with or without poststent balloon dilatation, to avoid understretch or overstretch of the stent diameter, and might contribute to better long-term outcomes as compared with conventional angiography guidance.48
Optical coherence tomography has recently been reported to assess vascular response to LMCA stenting.49
Fractional flow reserve
Fractional flow reserve (FFR) has been used to distinguish which LM patients require revascularisation. It may be reasonable to defer LM revascularisation in patients with a FFR >0.80. The application of FFR for LMCA assessment has potential drawbacks. In the presence of concomitant lesions in the LAD and LCx without repairing the downstream lesions, the FFR may underestimate the true significance of the LM lesion. Furthermore, in ostial LM lesions with catheter-induced damping upon engagement, uncomfortable manoeuvres are sometimes repetitively required to engage, inject intracoronary adenosine and disengage the guide. The administration of intravenous adenosine should be considered under these circumstances. There may be a discrepancy between angiographic per cent diameter stenosis and FFR in jailed LCx lesions after LMCA-LAD stenting. One study reports that the need for revascularisation of the ostial LCX after LMCA-LAD crossover stenting may be reduced, if the additional procedure is guided by FFR.50 However, further studies are needed to evaluate the efficacy of this strategy.
Debulking
After the introduction of DES, the role of debulking is diminished due to the benefit of restenosis reduction significantly. There is no evidence to show debulking prior to stenting with DES can further improve the long-term outcomes. Directional atherectomy may be preferable in LMCA bifurcations to aid the provisional single-stenting strategy. Similarly rotablator is used when calcification prevents stent delivery or calcified target lesion is not significantly dilated.
Haemodynamic support
Patients with unstable haemodynamic condition need pharmacological or device-based haemodynamic support. LMCA lesions with old age, MI cardiogenic shock, and decreased LV ejection fraction are common conditions requiring elective or provisional haemodynamic support. Out of many support devices, IABP has been used most extensively. Its elective use needs to be considered for high-risk conditions, having multivessel disease, complex LMCA anatomy, low ejection fraction or unstable presentations. Other new support devices, such as Impella LP 2.5 and LP 5.0 may be a preliminary answer to the need for a minimally invasive and easily deployable mechanical assist device that provides superior haemodynamic support compared with IABP.
Antithrombotics
Careful administration of antiplatelet agents is important to prevent the occurrence of stent thrombosis. Despite the lack of evidence, many clinicians have suggested indefinite use of dual antiplatelet therapy (DAPT) for patients of LMCA treated with DES in high-risk patients (diabetes mellitus, multiple stents, chronic renal failure or presentation with MI). Park et al reported that continuing dual antiplatelet therapy beyond 1 year was no more effective in reducing major adverse events than aspirin monotherapy.51 Another study suggested routine use of platelet function testing with recommendation to increase clopidogrel dose to 150 mg if platelet aggregation is more than 50%.52 The new antiplatelet agents (prasugrel and ticagrelor) should be evaluated in patients with complex LMCA intervention. Even the additive role of glycoprotein IIb/IIIa inhibitor, cilostazole, low-molecular-weight heparin, direct thrombin inhibitor or new drugs need to be investigated in future studies.
Future perspectives
New generation of DES, dedicated bifurcation stents, tailored procedural techniques, advanced devices and novel imaging techniques will improve the clinical outcomes. The new antiplatelet agents (prasugrel and ticagrelor) might improve the safety of PCI in complex LMCA lesions. Upcoming randomised EXCEL trial (evaluation of Xience Prime or Xience-V eluting stent vs CABG for effectiveness of LM revascularisation) will evaluate the long-term safety, durability and efficacy of PCI as compared with CABG in patients with unprotected LMCA disease with low or intermediate SYNTAX score (<33). The results of this trial might impact the current practice.
Conclusion
LMCA stenting is a different animal. One must think before embarking. Current guidelines indicate CABG as the optimal treatment for LMCA lesions. However, data from worldwide registries and left main subset of SYNTAX are encouraging towards a non-inferiority of PCI with DES versus CABG with regard to MI, death and cardiovascular events at medium-term follow-up. LMCA stenting is feasible and is generally technically safe although there are some special considerations during the stenting process. Stenting of ostial and shaft of LMCA can be achieved without major technical difficulties and with good immediate and long-term results. Distal LMCA bifurcational lesions continue to pose a considerable challenge and require expertise and performance of unique approaches for optimal results. An integrated approach that combines advanced devices, specialised techniques, adjunctive imaging support, as well as adjunctive pharmacological agents would continue to improve PCI success rate and long-term outcomes for these complex subsets. The EXCEL trial will demonstrate whether PCI with new generation of DES will compete with CABG as regards safety endpoint.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; internally peer reviewed.