Article Text

Abstract
Background Peripartum cardiomyopathy (PPCM) is a rare disease entity of unknown aetiology. High rates of mortality or poor overall clinical outcome are reported in women with this condition. Certain characteristics are risk factors for this disease. In Asia, there are limited data, especially in the Southeast Asian region. In the Philippines, no data exist regarding the prevalence or risk factors.
Objectives To determine the prevalence, profile and outcomes of PPCM in Philippine General Hospital and to describe their echocardiographic findings.
Methods All patients diagnosed with PPCM in the period of 1 January 2009–31 December 2010 were seen and examined. Demographic data and echocardiogram of the patients were reviewed.
Results 9 were diagnosed with PPCM during the study period. The prevalence is 1 in 1270 live births. Mean age was 29. 78% presented with moderate to severe heart failure symptoms in the prepartum period. Among purported risk factors for PPCM, obesity, multiparity and pre-eclampsia were seen in most. Conversely, only one patient admitted to having more than a single sexual partner. Only one patient had multifetal pregnancy. None were smokers. 44% underwent caesarean section for maternal indication. No mortality was seen. Fetal outcomes were good with all resulting in live births and most were appropriate for gestational age. Echocardiographic findings showed global wall motion abnormalities in the majority, mean ejection fraction of 34% and mean fractional shortening of 20%.
Conclusions PPCM is rare in the Philippines. Compared with international data, our patients are younger with low percentages of promiscuity, multifetal pregnancy, smoking history and tocolytic use. Similar to previous studies, obesity, multiparity and pre-eclampsia were also present in our PPCM patients. Immediate maternal and fetal outcomes were generally good. Adherence to standard heart failure management is high.
- HEART FAILURE
Statistics from Altmetric.com
Introduction
Peripartum cardiomyopathy (PPCM) is a rare disease entity of unknown aetiology. High rates of mortality or poor overall clinical outcome are reported in women with this condition.1–3 The incidence of PPCM is variable across the different regions of the world. Haiti reported approximately 1 case per 300 live births and some parts of Africa reported a higher incidence compared with America with as many as an estimated 1 case per 3000–4000 live births.4–6 In Asia, limited data were reported for PPCM in countries such as India and Turkey.7 In the Philippines, no data exist regarding the incidence of PPCM.
PPCM is diagnosed if these four criteria are met: (1) development of cardiac failure in the last month of pregnancy or within 5 months of delivery, (2) absence of an identifiable cause of the cardiac failure, (3) absence of recognisable heart disease prior to the last month of pregnancy and (4) echocardiographic finding of left ventricular systolic dysfunction (depressed shortening fraction or ejection fraction).
Different centres worldwide have reported various risk factors for PPCM such as advanced maternal age, multiparity, twin pregnancy, gestational hypertension, use of tocolytic therapy and even socioeconomic status.8 Despite continuing research, the aetiology of this disease and preventive measures remain elusive. In our country, there is a paucity of data on the prevalence of PPCM as well as associated risk factors.
Research objectives
Primary objectives
-
To determine the prevalence of PPCM among those who delivered in Philippine General Hospital (PGH) from 1 January 2009 to 31 December 2010.
-
To determine clinical profile of patients with PPCM in PGH admitted from 1 January 2009 to 31 December 2010.
-
To describe the echocardiographic profile of patients diagnosed with PPCM in the inhospital setting.
Secondary objectives
-
To identify associated risk factors and inhospital outcomes of patients with PPCM referred to cardiology service for the period 1 January 2009–31 December 2010.
Methodology
All patients referred to cardiology service for suspected PPCM during the period 1 January 2009–31 December 2010 were considered in the study. Sources of referrals were from the general medicine wards and intensive care unit, obstetrics admitting section, intensive maternal unit and pay services of the PGH. A diagnosis of PPCM was based on clinical and echocardiographic criteria as given by the National Heart, Lung, and Blood Institute and Office of Rare Diseases (National Institutes of Health) as follows: (1) New York Heart Association (NYHA) functional Class II–IV; (2) symptoms of heart failure developing in the last month of pregnancy or the first 5 months postpartum; (3) LV ejection fraction less than 45% or M-mode fractional shortening less than 30%, or both and end diastolic dimension more than 2.7 cm/m2 on transthoracic echocardiography; and (4) no other identifiable cause for heart failure. All participants should have normal functional capacity prior to pregnancy.
Patients with the following comorbidities were excluded from this study: chronic obstructive pulmonary disease, significant organic valvular heart disease, severe anaemia, liver cirrhosis and mean arterial pressure (MAP) abuse.
Medical records of patients identified with PPCM in the period 1 January 2009–31 December 2010 were reviewed. All data were gathered from the chart of patients diagnosed with PPCM referred to cardiology service. The data were mainly taken from a standard form from the Section of Cardiology, designed for PPCM. The data were gathered mostly by cardiology fellows-in-training and recorded in a standard data collection form (see online supplementary appendix A).
All the echocardiograms were retrieved from the Section of Cardiology Echocardiogram archives. Each of the videos was reviewed and read by three different adjudicators (cardiology consultants and fellows) from the UP-PGH Section of Cardiology. Findings were tabulated and recorded.
The following demographic data were extracted: age, parity, presence of multifetal pregnancy, socioeconomic status, smoking and alcohol intake, presence of coexisting hypertension and body mass index. Diabetes mellitus and hypertension (pre-eclampsia, eclampsia, chronic hypertension) were also noted. Functional capacity, echocardiographic parameters and medications were also documented. And last, complications of pregnancy, fetal (age of gestation, live birth, fetal death) and maternal outcomes (mortality, functional capacity on discharge—NYHA functional classification) were recorded.
Statistical analysis
Descriptive statistics were used for the demographics and echocardiographic data.
Results
Nine patients were diagnosed with PPCM during the study period. The prevalence is 1 in 1270 live births. Table 1 shows the demographic profile of PPCM patients. Median age was 27 years. Most were term deliveries save for one preterm birth. Almost all (78%) presented with moderate to severe heart failure (NYHA Class III and IV) symptoms in the prepartum period. Among purported risk factors for PPCM, obesity and multiparity were seen in most patients (78% each). Conversely, only one patient admitted to having more than a single sexual partner. Only one patient had multifetal (twin) pregnancy. Fetal outcomes were generally good with all resulting in live births and most (71%) were appropriate for gestational age. No maternal mortality occurred.
Demographic characteristics of patients with peripartum cardiomyopathy
Table 2 shows concomitant conditions of the PPCM patients. Pre-eclampsia was common at 78%. Type 1 diabetes mellitus was seen in one patient. None of the patients were smokers. No patient underwent tocolysis. Table 3 shows the echocardiographic findings of the patients. The majority showed global wall motion abnormalities. The majority had severely depressed (<30%) ejection fraction with mean fractional shortening of 20%. Most had normal left ventricular dimension. Table 4 shows the medications used for all the PPCM patients. Diuretics, oxygen support and salt and fluid restriction were employed for all patients. The use of β-blockers and ACE inhibitor were also high.
Associated comorbid conditions of PPCM patients
Echocardiographic profile of PPCM patients
Medications given for patients
Discussion
Prevalence and risk factors
Compared with US data which reported an incidence of 1:3000–1:4000 live births, our study demonstrated that PPCM is more common among Filipinos. This frequency, however, is less than that of other third world countries such as Haiti and African countries which reported an incidence of 1:300 live births. This relatively high prevalence of PPCM in the Philippines would possibly support the association of PPCM and geographical location, that is, being a tropical country with increased heat and humidity as suggested in other reports.9 ,10 Tendency for PPCM to occur among low socioeconomic status countries supports the hypothesis of a possible infectious cause of this condition. Poor hygiene and poor prenatal care may be contributory.
Most PPCM occur among multiparous women more than 30 years of age.11 ,12 Most of our patients were multiparous. Why multiparity may be associated with PPCM remains unclear. There are reported possible reasons for recurrence of PPCM in subsequent pregnancies. One reported that the risk of irreversible cardiac damage may increase with each subsequent pregnancy.13 Also, the contractile reserve is impaired, even though the left ventricular size and function return to normal in the prior affected pregnancy.14 None of the multiparous patients in the study had a past history of PPCM. One possible reason is that, during previous pregnancies, cardiac changes were already present but did not manifest clinically. Alternatively, subtle symptoms of heart failure were already felt but were dismissed as typical symptoms of pregnancy precluding further diagnostic work up.
Contrary to previous reports of association of PPCM and advance maternal age, our patients were of a wide age range with the youngest mother at 19-years-old and oldest at 45-years-old. Half of them were <30-years-old.
Promiscuity resulting in sexually transmitted disease has been reported to be correlated with presence of PPCM.15 The reason for this is hypothesised to be exposure to an infectious agent, that is, viral infection or Chlamydia infection which may largely affect the heart through impaired immune response mechanism that leads to PPCM. In our study, report of promiscuity is low.
There is a strong association noted between PPCM and gestational hypertension. In our study, pre-eclampsia was very common (78%) and even higher in prevalence compared with published reports.11 ,16 ,17
Twin pregnancy is reported to be considerably associated with the development of PPCM. An autoimmune process has been proposed by Ansari et al18 who found high titres of autoantibodies against normal human cardiac tissue proteins in the sera of PPCM patients. This finding may be due to haematopoietic lineage cell traffic (chimerism) from the fetus to the mother during gestation, which is increased in twin pregnancies.19 Twinning was seen in only one of our patients.
Another suggested risk factor for PPCM is the use of tocolytic therapy such as terbutaline.11 ,20 This association is likely a reflection of the increased incidence of premature labour. No patient in our study underwent tocolysis.
Maternal outcome
Four of our patients (44%) underwent caesarean section for maternal indication, mostly because of heart failure. This is similar with the rate of caesarean delivery of 40% in patients with PPCM as reported by Elkayam et al.11 Potential reasons for the high rate of caesarean section are a high incidence of gestational hypertension, twin pregnancy and older maternal age.21–23
Preterm delivery is common among PPCM patients.11 The high incidence is thought to be due to the increased incidence of gestational hypertension and twin pregnancies.21 ,22 Only one patient in our study delivered preterm.
Complicated maternal course as influenced by heart failure, uncontrolled hypertension and multifetal gestation may confer a higher mortality risk for PPCM mothers. Mortality as high as 18%24 immediately postpartum and 32% within 6 months was described in the USA and Africa, respectively. Recent studies showed lower mortality of <10% probably reflecting improved medical therapy for heart failure.11 ,25
Fetal outcome
Cardiomyopathy is believed to affect the fetus. In the study by Witlin et al,26 there were no fetal deaths, but there was an increased incidence of premature and low birthweight infants. These findings suggest that the underlying disease process may begin much earlier than the clinical signs and symptoms are manifested. The development of PPCM in the mother may be a marker of high risk for the baby. In our study, no fetal death was observed. Preterm delivery occurred with one patient who carried twins and both babies were small for gestational age. One baby was large for gestational age due to diabetes in the mother. Four babies had poor APGAR score at 1 min (≤7) but all improved to APGAR score 9 after appropriate neonatal resuscitation after 5 min.
Echocardiographic profile
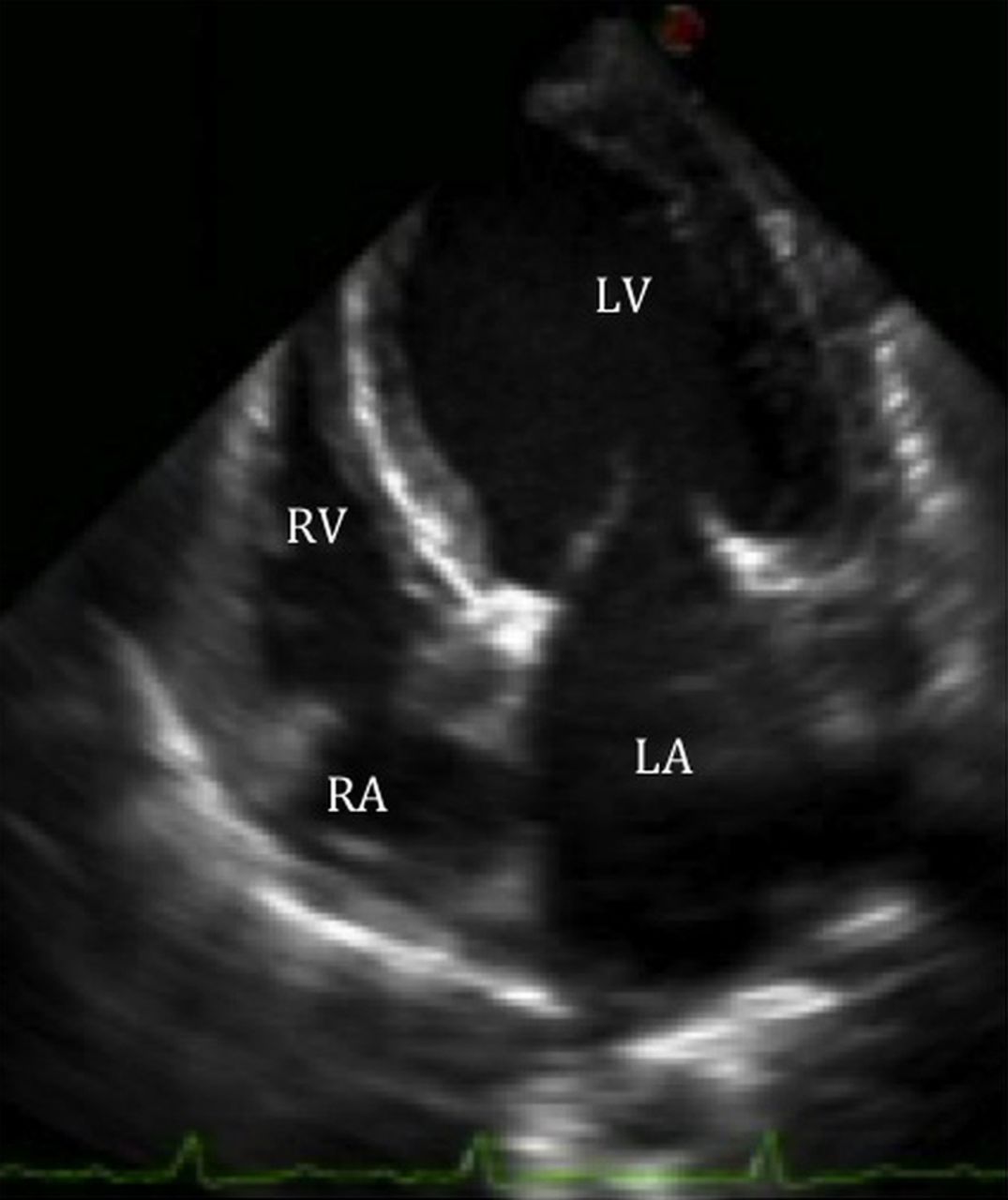
The left ventricular end diastolic dimension of our PPCM patients were within normal with a mean of 51 mm based on current international standards. This is in contrast with the findings of Witlin et al26 who reported mean left ventricular end diastolic diameter (LVEDD) of 55–68 mm. The fractional shortening of our PPCM patients were similarly depressed at a mean of 18% with that of Witlin et al who reported 14%–22%. Likewise, the ejection fractions were consistent with moderately to severely depressed overall systolic function at a mean of 35%. Severely depressed ejection fraction was seen in 44% of our patients. These echocardiographic findings are consistent with the criteria set by Demakis et al16 as supporting evidence to the classic clinical picture of PPCM. The discrepancy in the LVEDD between this study and that of Witlin et al26 is likely because of anatomic variation in left ventricular dimension of Asian and Caucasian population. Figures 1⇓–3 demonstrate some pertinent echocardiographic findings.

Four chamber view on transthoracic echocardiography of patient #2. Left ventricular end diastolic diameter is noted to be 51 mm. There is also note of global hypokinesia. Ejection fraction via Simpson's method is computed at 33%.

Four chamber view on transthoracic echocardiography of patient #4. There is note of global hypokinesia. Ejection fraction via Simpson's method is computed at 26%.

{kind=link}
{kind=link}
{kind=link}
Four chamber view on transthoracic echocardiography of patient #9. There is global hypokinesia. Ejection fraction via Simpson's method is computed at 49%. This echocardiogram also demonstrates a moderate mitral regurgitation on Doppler.
Limitation of the study
Only immediate maternal and fetal outcomes were included in the study. Documentation of resolution or persistence of clinical and echocardiographic parameters is not part of the study.
There is also a referral bias since PGH is the major referral centre for complicated pregnancy cases in the Philippines.
Conclusions
PPCM is a rare entity in the Philippines. Our patients have varied age with low percentages of promiscuity, multifetal pregnancy, smoking history and tocolytic use. Similar to previous studies, obesity, multiparity and pre-eclampsia were also present in our PPCM patients. Inhospital maternal and fetal outcomes were generally good. Last, adherence to standard heart failure management is high.
Recommendation
Our study may be considered as the first in the Philippines. This may serve as a good start in making a registry for patients with PPCM that is a very important step to improve medical characterisation of PPCM. Epidemiological analysis on Filipino patients could allow a better understanding of risk and predisposing factors as well as natural history, diagnosis and treatment efficacy of PPCM. Thus, a more extensive data collection and study for PPCM is recommended. In doing so, we can have our own Philippine data that can be used by international experts to come up with an up-to-date population based clinical guidelines for the use of the entire medical community.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
This paper is based on a presentation made at the 16th Annual Scientific Meeting of the Heart Failure Society of America in September 2012. The conference abstract was published in Journal of Cardiac Failure.
-
Contributors VIS: Conception and design of the study, analysis and interpretation of the data, and drafting the manuscript. QGN: Conception of the study, analysis and interpretation of the data, and drafting the manuscript. GDBM and JAMA: Analysis and interpretation of the data, drafting of the manuscript. ER and FERP: Drafting and revising the manuscript and final approval of the manuscript submitted.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Philippine General Hospital Ethics Review Board.
-
Provenance and peer review Not commissioned; internally peer reviewed.