Article Text

Abstract
Background Dual antiplatelet therapy with clopidogrel and aspirin is the standard of care for patients undergoing percutaneous coronary intervention (PCI).
Objective To determine the clinical characteristics associated with high on-treatment platelet reactivity (HPR) of patients undergoing PCI after a 300 mg loading dose of clopidogrel, measured by thrombelastography (TEG).
Methods and results 394 consecutive patients were enrolled in this prospective observational study. All had been receiving aspirin 100 mg/day for more than 7 days, but were clopidogrel naïve. A 300 mg loading dose of clopidogrel was given more than 12 h before the procedure. The cut-off point for HPR was defined as ≥70% adenosine-5-diphosphate-induced aggregation. The prevalence of HPR was 21% as measured by TEG. More women than men (41.7% vs 27.1%, p=0.01) were found in the HPR group. Raised glycosylated haemoglobin (HbA1c) was more prevalent in the HPR group than in the group with normal on-treatment platelet reactivity (NPR) (45.2% vs 30.0%, p=0.009). Patients with HPR had a higher level of total plasma cholesterol (4.8±1.5 mmol/l vs 4.3±1.1 mmol/l, p=0.002) and low-density lipoprotein cholesterol (2.8±1.1 mmol/l vs 2.5±0.9 mmol/l, p=0.022) than those with NPR. Multivariable logistic regression analysis showed that female gender (OR=3.175, 95% CI 1.428 to 7.059, p=0.005) and raised HbA1c (OR=1.911, 95% CI 1.066 to 3.428, p=0.03) independently predicted the occurrence of HPR.
Conclusions Despite pretreatment with aspirin and a 300 mg loading dose of clopidogrel, 21% patients undergoing PCI exhibited HPR measured by TEG. A raised level of HbA1c and female gender independently predicted the findings.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Introduction
Platelet activation and thrombin generation are central processes in the development of ischaemic complications after percutaneous coronary intervention (PCI).1 Dual antiplatelet therapy with clopidogrel and aspirin is the standard of care for patients undergoing PCI. Clinical studies have shown that high postprocedural on-treatment platelet reactivity is associated with increased recurrent ischaemic events, including stent thrombosis.2–4 Furthermore, multiple studies have demonstrated a clear association between high on-treatment platelet reactivity (HPR) to adenosine-5-diphosphate (ADP) measured by various methods and the occurrence of adverse clinical events. Despite this, the routine measurement of on-treatment platelet reactivity has not been widely implemented and recommended in the guidelines.
An earlier study had suggested that patients with HPR had a higher prevalence of hypertension, diabetes, and use of calcium channel blockers.5 It was also shown that there is a strong association between clopidogrel resistance and female gender in patients with coronary artery disease when platelet activity was tested using ADP-induced aggregometry.6 Thrombelastography (TEG) platelet mapping can be used to assess the responses of circulating platelets to both aspirin and clopidogrel in whole blood. A single TEG assay can provide information on both the overall tendency to thrombosis and the response to antiplatelet therapy. The aim of this study was to use TEG to evaluate clinical characteristics associated with HPR in patients receiving dual antiplatelet therapy undergoing non-emergent PCI.
Patients and methods
Patients
Three hundred and ninety-four consecutive patients undergoing non-emergent PCI were enrolled in this prospective observational study from February 2011 to January 2012. All patients were aged >18 years, had been receiving aspirin 100 mg/day for more than 7 days and were clopidogrel naïve. Exclusion criteria included a history of bleeding diathesis, acute myocardial infarction within 48 h before enrolment, a history of previous coronary artery bypass surgery or PCI and administration of glycoprotein IIb/IIIa inhibitors before the procedure. A 300 mg clopidogrel loading dose was administered at least 12h before the index procedure. The patients were maintained on aspirin 100 mg/day and clopidogrel 75 mg/day dose after the procedure.
Blood sampling and TEG analysis
Baseline fasting blood samples were obtained from patients before PCI. Samples were collected in separate Vacutainer blood collecting tubes and sent for determination of number of platelets, glycosylated haemoglobin (HbA1c), fasting plasma glucose, C-reactive protein, plasma triglyceride, cholesterol and cardiac enzymes.
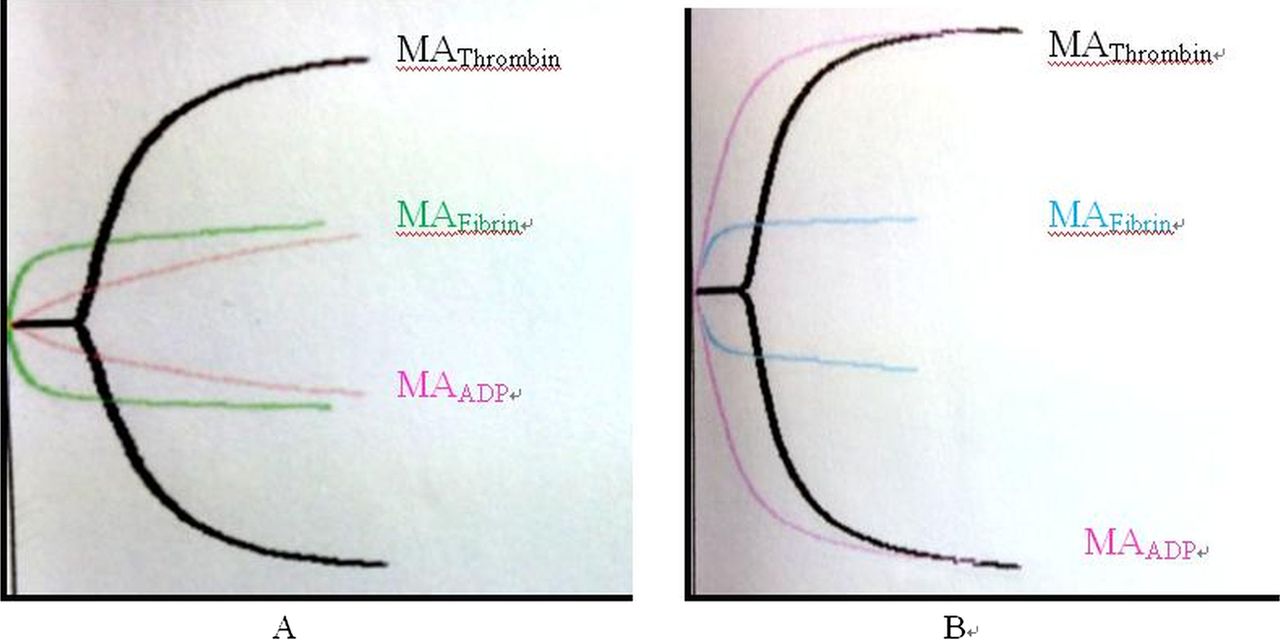
TEG samples were obtained 18–24 h after PCI by venipuncture at the antecubital fossa. The first 2 ml of each blood sample was discarded to avoid platelets activated by endothelial trauma. Samples for TEG analysis were then obtained and placed into plain or heparin-containing tubes depending on the reagent to be added subsequently. Samples were analysed using a four-channel computerised TEG analyser (Haemonetics Corporation, Braintree, Massachusetts, USA). The four channels used were (1) kaolin; (2) activator F alone; (3) activator F+arachidonic acid (AA) and (4) activator F+ADP. For the kaolin channel 1 ml of whole blood was mixed with 1% kaolin solution. The mixed sample (360 μl) was then placed in the kaolin cup and analysed immediately. For the other three channels, 10 μl activator F, a mixture of reptilase and factor XIII was placed in each cup, respectively. AA 100 ml (1 mM) was placed in the third channel cup and 100 ml of ADP (2 μM) was placed in the remaining channel cup. All reagents were prepared at room temperature. A total of 360 ml heparinised blood was then added to the activator F, AA and ADP channel cups and mixed with the reagents. The TEG analyser was then started and left to run for 1 h to produce a trace, which became the subject for subsequent analysis. For each trace, the standard TEG parameter—that is, maximum amplitude (MA), was determined by the TEG software (figure 1).
{kind=link}
Thrombelastograph platelet mapping analysis parameters. (A) ADP-induced platelet aggregation=0%, (B) ADP-induced platelet aggregation=97.2%. MAThrombin, measure of maximum thrombin-induced platelet-fibrin clot strength; MAFibrin, contribution of fibrin to clot strength; MAADP, clot strength after ADP stimulation. ADP, adenosine-5-diphosphate; MA, maximum amplitude.
Definitions
Platelet aggregation in response to ADP or AA is calculated with computerised software on the basis of the formula: %Aggregation=[(MAADP or AA − MAFibrin)/(MAThrombin − MAFibrin)]×100%. The cut-off points for HPR were defined as ≥70% ADP-induced aggregation with 2 μmol ADP as measured by TEG.6 All patients below the cut-off point were defined as exhibiting normal on-treatment platelet reactivity (NPR).
Statistical analysis
Statistical analysis was performed using SPSS V.16.0 (SPSS, Chicago, Illinois, USA). Categorical variables are expressed as n (%) and continuous variables as mean±SD with p<0.05 considered statistically significant. The χ2 test was used for comparison of categorical variables and the Student t test was used for comparison of continuous variables between groups. Demographic and procedural variables with p values <0.1 in the univariate analysis were entered by stepwise forward selection in a multivariate logistic regression analysis.
Results
Three hundred and ninety-four consecutive patients undergoing non-emergent PCI with aspirin treatment and clopidogrel naïve were enrolled. Of these patients, 204 were admitted with unstable angina, and 21 had myocardial infarction (enrolled ≥48 h after infarction). The remainder had stable angina.
Demographics
Clinical characteristics of the study population are presented in table 1. There were more female patients in the HPR group than in NPR group (41.7% vs 27.1%, p=0.01). The prevalence of raised HbA1c was higher in the HPR group (45.2% vs 30.0%, p=0.009). Additionally, a higher level of total plasma cholesterol (4.8±1.5 mmol/l vs 4.3±1.1 mmol/l, p=0.002) and low-density lipoprotein cholesterol (LDL-C; 2.8±1.1 mmol/l vs 2.5±0.9 mmol/l, p=0.022) were more common in the HPR group. No significant differences were found in age, left ventricular function, hypertension, current smoking, diabetes, cardiac enzyme and platelet counting between the groups.
Patient demographics
Procedural characteristics are shown in table 2. Briefly, multivessel interventions were common and all patients were implanted with drug-eluting stents. There were no significant differences in the number of vessels treated, lesion location, number of stents and lesion length between the two groups.
Procedural characteristics
Platelet aggregation
All 394 patients had blood samples analysed by TEG. Mean ADP-induced post-treatment platelet aggregation was 45±9% and mean TEG-MAADP was 35±8 mm. In 84 patients (21%) ADP-induced aggregation measured by TEG was ≥70%. Mean AA-induced post-treatment platelet aggregation was 11±7% and mean TEG-MAAA was 19±6 mm. AA-induced aggregation was ≥50% in only nine (2.3%) patients.
Relation of HPR and clinical characteristics
Multivariable logistic regression analysis (table 3) showed that female gender (OR=3.175, 95% CI 1.428 to 7.059, p=0.005) and raised HbA1c (OR=1.911, 95% CI 1.066 to 3.428, p=0.03) independently predicted the risk of HPR.
Logistic regression analysis
Discussion
The fixed dose, ‘one size fits all’ clopidogrel treatment strategy, which has been used in clinical trials and is recommended by current guidelines, does not take into account the interindividual pharmacodynamic variability of clopidogrel treatment.7–9 Earlier studies reported wide variations in HPR to ADP of between 5% and 44%.10 In this study, the prevalence of HPR was 21% measured by TEG, which was comparable to the results of earlier studies by Bliden et al6 (30%) and Müller et al11 (30%).
However, the optimal methods for quantifying platelet reactivity and the threshold definition for HPR to ADP have been subjects of controversy. Recently, several assays have been developed and have shown some potential as point-of-care tests of the effects of antiplatelet medication. These include the PFA-100 (Dade Behring, Deerfield, Illinois, USA), the Accumetrics VerifyNow system (Accumetrics, San Diego, California, USA), Plateletworks (Helena Laboratories, Allen Park, Michigan, USA) and the Cone and Plate (let) analyser (DiaMed, Canton, Ohio, USA), as well as the modified TEG platelet mapping system.12 Nevertheless, no single test can encompass or reflect the complexity of platelet biology and function. Modified TEG is a rapid, simple, bedside test with automated analytical software that provides an accurate, quantitative and qualitative measurement of the physical properties of a platelet-fibrin clot. The results of the PREPARE POST-STENTING study13 showed increased ADP-induced aggregation measured by TEG in patients with ischaemic events, compared with patients without events. Furthermore, Gurbel et al14 reported that MAADP>47 mm had the best predictive value of long-term ischaemic events compared with other measurements. Each of these studies supported the important role of modified TEG in optimising antiplatelet treatment and reducing adverse events.
It is not known whether HPR to ADP is a multifactorial processes influenced by clinical, demographic or procedural characteristics. Our data showed that a raised HbA1c level (>6.5%) was associated with HPR. Research data has shown that in conditions of insulin resistance, platelets are resistant to the action of insulin and also to NO and prostacyclin, indicating upregulation of platelet activity/aggregation. The mechanism behind this might be related to a disproportionate increase in intraplatelet calcium concentration (the main activator of platelets) as opposed to intraplatelet cAMP and cGMP (inhibitors of platelet function) in individuals with insulin resistance.15–18
Interestingly, our data showed that there were more female (41.7% vs 27.1%, p=0.01) patients in the HPR group than in NPR group. Moreover, multivariable logistic regression analysis showed that female gender (OR=3.175, 95% CI 1.428 to 7.059, p=0.005) independently predicted the risk of HPR. This finding was concordant with the results of Hobson et al,19 who found that women had less response to clopidogrel percentage reduction in AUC15 (area under the response curve at 15 min) with ADP 36.4±12.4 vs 64.0±13.2, p<0.01), and also higher post-treatment reactivity (AUC15 of ADP 714±161 vs 311±146, p<0.01) compared with men. Other studies also showed that baseline platelet hyper-reactivity was more common in women, and mean levels of platelet aggregation in response to stimulation with platelet agonists were consistently higher in women than in men.5 ,20 The cause of this phenomenon is unknown, but might be due to the effect of the female hormone, high baseline clotting tendency and a diminished response to clopidogrel in women.
Limitations
Our study has several potential limitations. First, the study population was small and this was a prospective observational study without randomisation. Although we found some clinical characteristics that might be associated with HPR to ADP, larger randomised clinical trials in this subset of patients are necessary to confirm our findings. Second, the short follow-up period made it impossible for us to correlate late clinical events with the markers we measured. Further evidence is needed to clarify the relationship between clinical characteristics, HPR tested by TEG and ischaemic events. Third, the antiplatelet effect of clopidogrel may fluctuate in patients even at the same dose. A single baseline measurement may not reflect the extent of platelet inhibition over long periods of time. Finally, the result of our study is limited to patients with a 300 mg loading dose of clopidogrel. It is not uncommon for patients to receive a 600 mg loading dose for non-emergent PCI, and thus a separate study is needed to study the effect of the increased dose on platelet reactivity.
Conclusions
Despite adequate pretreatment with 300 mg of clopidogrel, 21% of patients undergoing non-emergent PCI exhibited high on-treatment ADP-induced platelet aggregation measured by modified TEG. We found that raised HbA1c and female gender independently predicted the risk of HPR. The potential for clinical application of modified TEG as a point-of-care test in this group of patient requires further investigation.
References
Footnotes
-
Contributors X-MH: conception, design, and drafting of the article. W-ZH: analysis of the results. X-BQ: interpretation of the data. W-YF: final approval of the version published.
-
Competing interests None.
-
Ethics approval Obtained.
-
Provenance and peer review Not commissioned; internally peer reviewed.
-
Open Access This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/