Article Text

Statistics from Altmetric.com
Introduction
Lead perforation is one of the feared complications after transvenous permanent pacemaker implantation, which can occur during or after the procedure. Usually, a left bundle branch block (LBBB) pattern on a surface 12-lead ECG recording is observed after right ventricular (RV) apical pacing. The presence of a right bundle branch block (RBBB) pattern raises the suspicion of lead perforation. However, it can be a normal finding in RV apical pacing. Here, we report a case of an RBBB pattern on ECG after RV apical permanent pacemaker implantation, which raised a red flag, but was later found to be a needless concern.
Case description
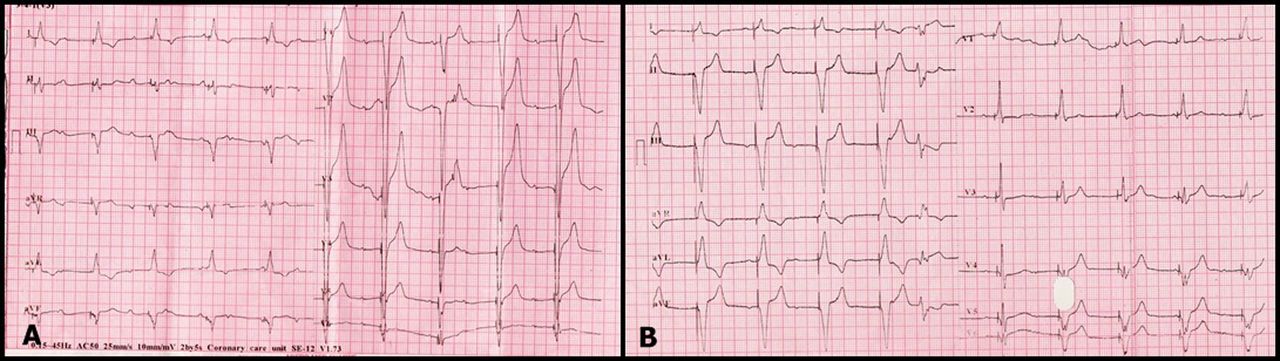
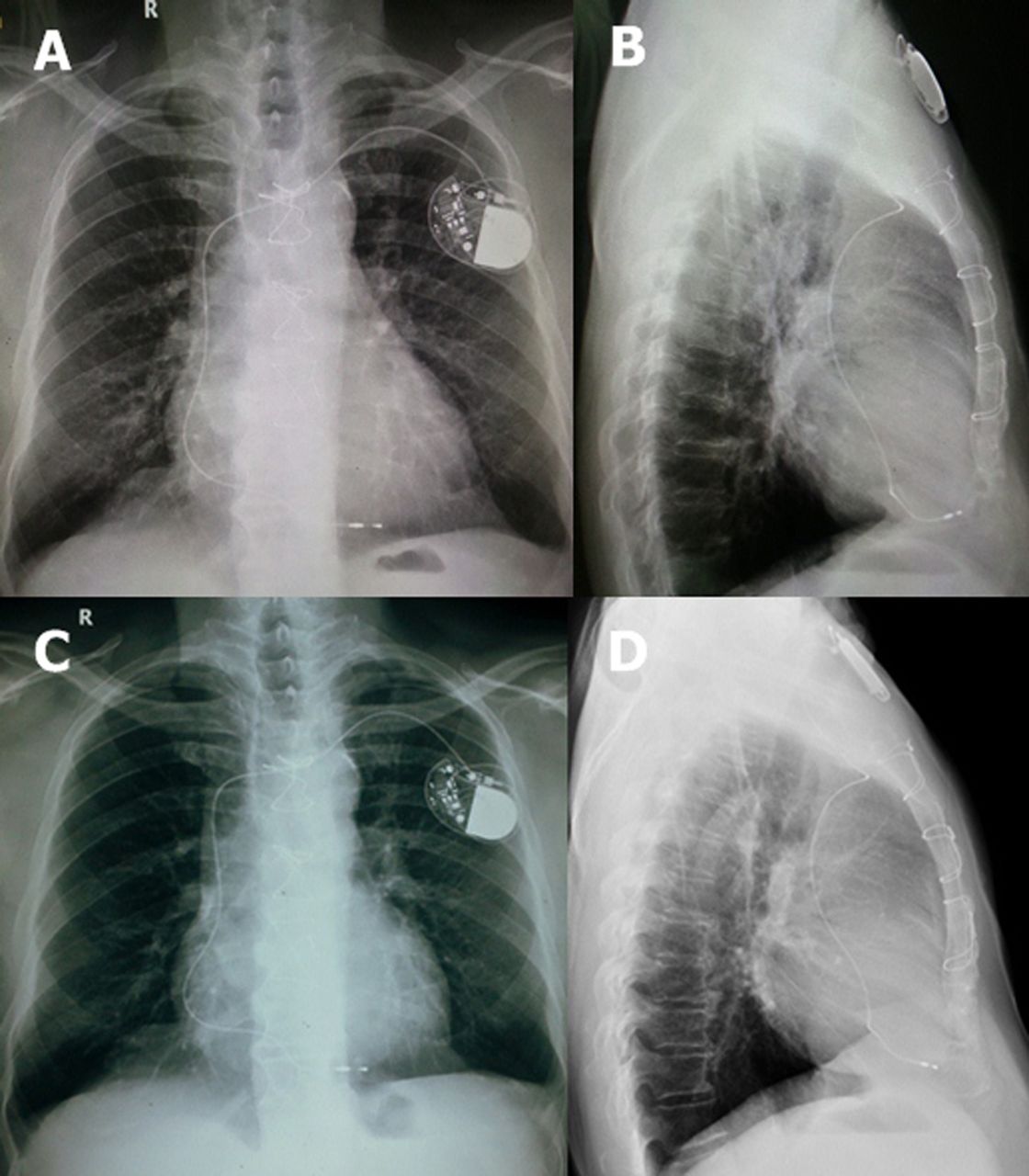
A 74-year-old man with symptomatic broad complex complete heart block with baseline RBB QRS morphology underwent successful RV apical permanent pacemaker implantation (VVI mode, bipolar lead; St Jude Medical) with an uneventful postoperative period. A 12-lead ECG showed full capture with the expected LBBB QRS morphology (figure 1A). The ventricular capture threshold was 0.5 V and lead impedance was 674 Ω. At routine follow-up at 2 months, ECG showed all captured beats but with RBBB QRS morphology (figure 1B). The QRS axis in the frontal plane was −80°. The patient was stable and had no presyncopal or syncopal events. He was admitted for evaluation and pacemaker interrogation, as lead perforation and displacement was strongly suspected. His haematological and biochemical evaluations were normal. Chest X-ray (figure 2A–D), echocardiography and fluoroscopy showed an appropriate RV apical position of the pacemaker lead. On pacemaker interrogation, all pacemaker parameters were within normal limits (ventricular threshold, 0.75 V; lead impedance, 477 Ω). The patient remained asymptomatic while under observation and was discharged after reassurance regarding the normalcy of pacemaker function. The patient is doing well on follow-up.
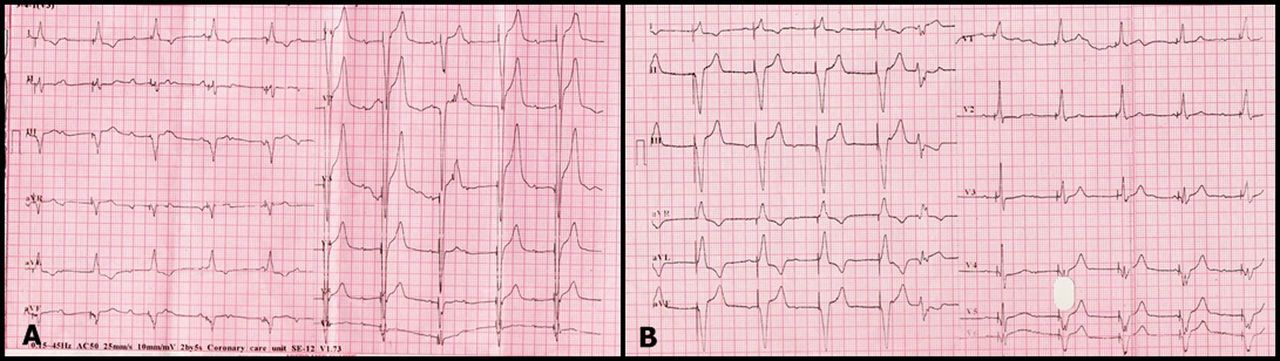
(A) Postoperative 12-lead ECG showing full capture with the expected left bundle branch block QRS morphology. (B) Right bundle branch block QRS morphology with QRS axis on the frontal plane of around −80°, V1 and V2 showing R and Rs complex, respectively.

{kind=link}
{kind=link}
Chest X-ray posterior–anterior view (A) and left lateral view (B) taken on the third postoperative day showing the pacemaker lead at the right ventricular (RV) apex. Chest X-ray posterior–anterior view (C) and left lateral view (D) taken at the 2-month follow-up showing the appropriate RV apical position of the pacemaker lead and no evidence of lead displacement.
Discussion
The universally accepted rule that RV pacing will produce LBBB and left ventricle (LV) pacing of an RBBB pattern on a surface ECG may not always be correct. Paced RBBB QRS morphology in patients with RV apical pacing is usually indicative of inadvertent LV pacing through intracardiac defects such as patent foramen ovale, a ventricular septal defect. Sometimes it may represent coronary sinus pacing.1 ,2 However, a red flag is often raised to rule out a septal or free wall perforation. Although rare, uncomplicated RV apical pacing may paradoxically show RBBB QRS morphology.3 This may be reassuring if the frontal plane maximal QRS vector orientation is to the left. Still, an alarm must be sounded if a new right inferior orientation of the QRS axis is seen.4 Degree of frontal axis plane deviation on an ECG can be used to localise the site of pacing. Uncomplicated RV apical pacing is said to be present if the frontal axis plane is between 0° and −90° and precordial transition is at V3 with a sensitivity of 86% and specificity of 99%, while a transition at V4 may indicate middle cardiac vein pacing with a sensitivity of 72% and specificity of 100%. When a frontal plane axis occurs between −90° and −180°, LV pacing is more likely.5
Although the mechanism of RBBB QRS morphology in RV apical pacing remains unknown, a possible hypothesis is that the anatomically RV part of the interventricular septum acts as part of the LV, both functionally and electrically.6 Another view is that it could be the result of severe RV conduction disease leading to its delayed activation associated with relatively early activation of the LV conduction system.7 The RV apex is the most commonly used site of pacing because of the ease of implantation. A change in QRS morphology from LBBB to RBBB has not been commonly reported and, in the clinical setting, usually raises an alarm with resultant hospitalisation. Our case exemplifies the importance of analysing the QRS axis before raising a red flag, as the patient can easily be interviewed and reassured in the outpatient setting as well.
Conclusion
We report a case of RV apical pacing where the QRS morphology shifted from RBBB to LBBB raising the suspicion of lead perforation. However, the frontal plane QRS axis of −80° suggested correct RV pacing. This was also supported by an appropriate pacemaker lead position on chest X-ray, echocardiography and fluoroscopy with no significant changes in pacemaker parameters on pacemaker interrogation. Careful analysis of the surface ECG may obviate unnecessary hospitalisation.
Footnotes
-
Contributors All the authors were equally involved in data collection, data interpretation and preparation of manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.