Article Text

Statistics from Altmetric.com
Hypertrophic cardiomyopathy (HCM) is characterised by a heterogeneous clinical expression, unique pathophysiology and diverse natural history. Longstanding left ventricular (LV) outflow tract obstruction is a strong determinant of HCM-related progressive heart failure and cardiovascular death. Here we report the clinical features and natural history of a young female with HCM and mid-cavity obstruction who became symptomatically better after apical myocardial infarction which resulted in the loss of mid-cavity obstruction.
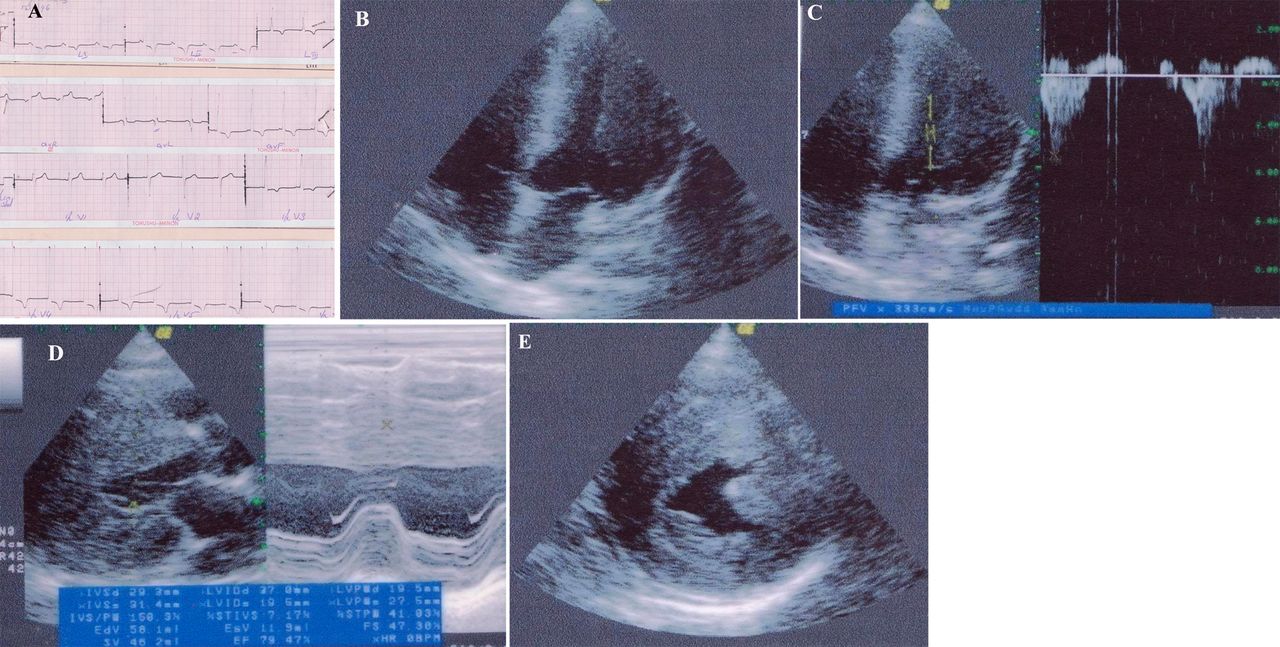
A 40-year-old woman presented with a history of progressive worsening of dyspnoea on exertion over the previous 6 months. She had been diagnosed with hypertrophic obstructive cardiomyopathy at the age of 28 years when she had recurrent episodes of syncope. Most of the syncopal episodes were exertional and started 3 years prior to the diagnosis. Her ECG at that time showed LV hypertrophy with T inversion in lateral chest leads (figure 1A) and echocardiographic examination showed severe LV hypertrophy with mid-cavity obstruction and near total obliteration of the LV apex in systole. The mid-cavity obstruction was dynamic with a peak gradient of 75 mm Hg (figure 1B–E). The patient was on oral propanolol 40 mg thrice daily. She had been lost to follow-up for the previous 10 years mainly because she felt better with no further syncope and discontinued all medications. Currently, she has NYHA class II heart failure.
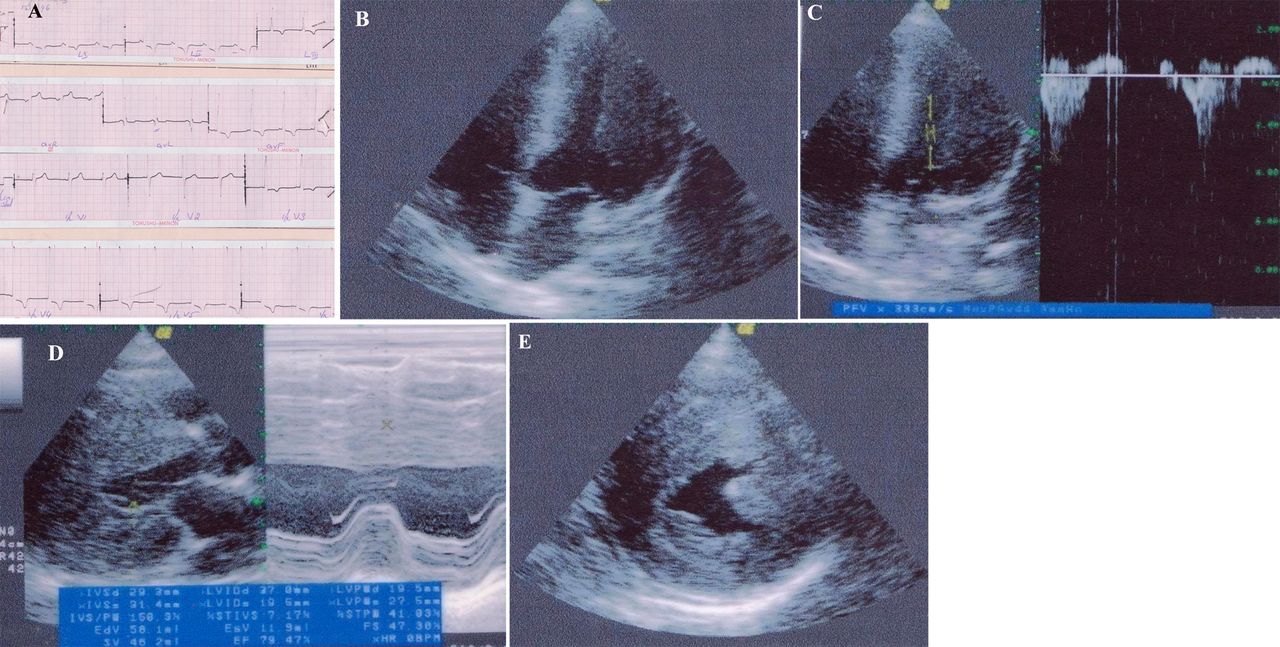
(A) 12-Lead electrocardiogram showing T wave inversion in lateral chest leads. (B–E) Transthoracic echocardiogram views showing severe concentric left ventricular hypertrophy and a mid-cavity gradient.
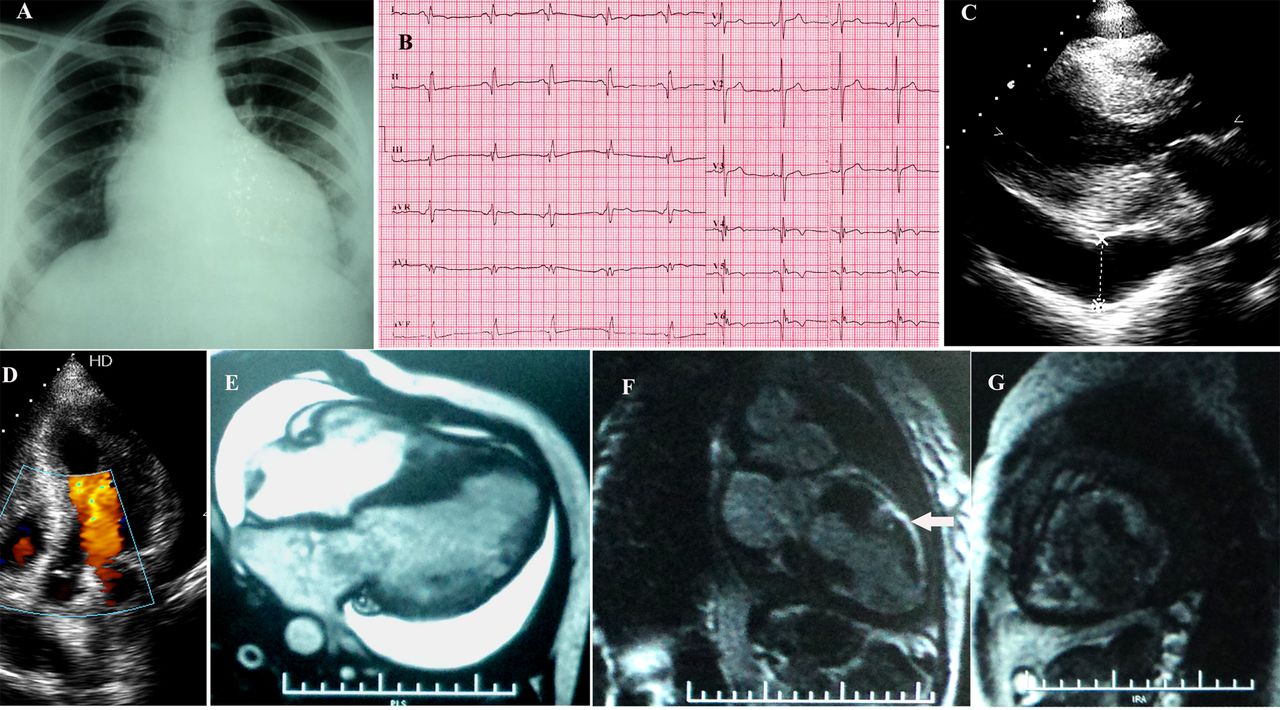
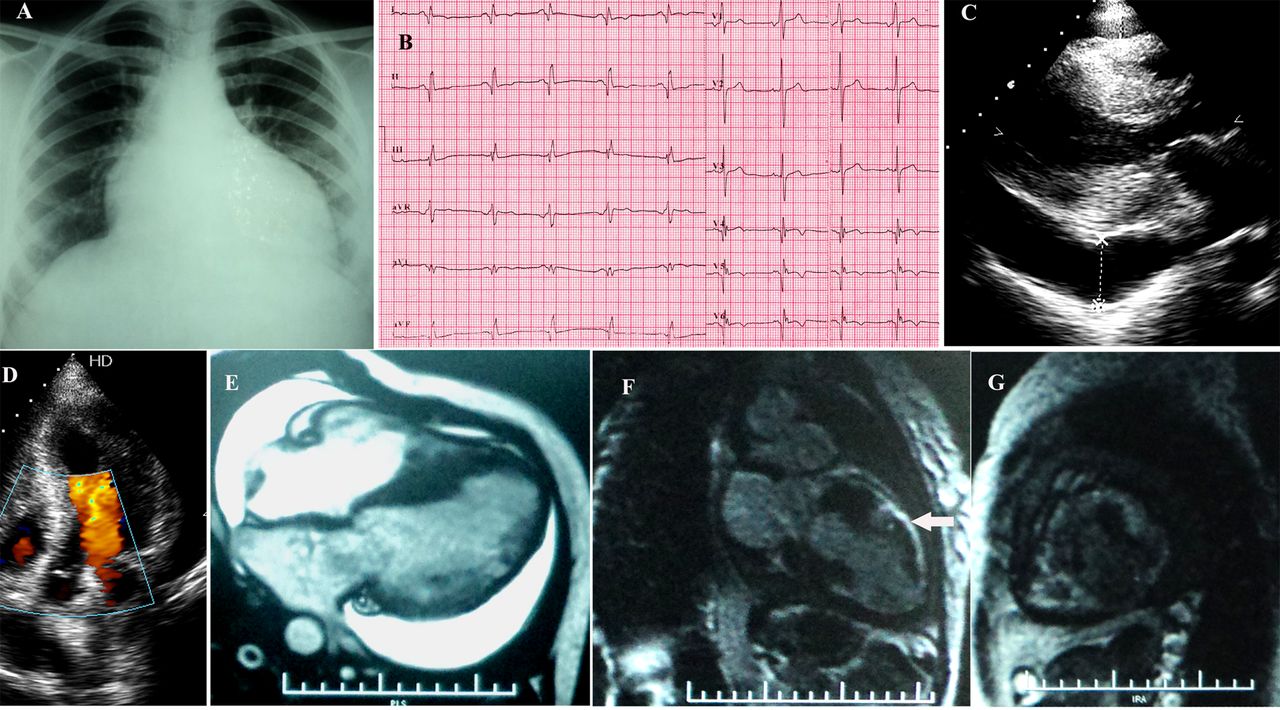
On examination her heart rate was 90/min with blood pressure of 120/80 mm Hg. She was not in heart failure and had a short mid-systolic murmur over the left sternal border. Her chest skiagram showed cardiomegaly (figure 2A). Electrocardiogram showed deep Q waves in leads V4, V5, V6 and an R/S ratio >1 in V1 and V2 suggesting an apical and postero-lateral myocardial infarction (figure 2B). Echocardiographic examination showed an akinetic apex, apical lateral wall and apical septum with moderate LV systolic dysfunction. There was a marked reduction in LV hypertrophy with no mid-cavity gradient (figure 2C,D, see online supplementary video 1). Mild pericardial effusion was present. Coronary angiogram showed normal epicardial coronary arteries. Gadolinium-enhanced cardiac MRI showed delayed subendocardial enhancement in the infero-lateral myocardium at the mid-cavity level and at the apex, suggestive of a myocardial scar (figure 2E–G). Currently, the patient is on β blockers, a statin, diuretics and antiplatelets with symptomatic improvement.
{kind=link}
{kind=link}
(A) Chest X-ray showing cardiomegaly. (B) 12-Lead ECG showing Q waves in infero-lateral leads. (C) Transthoracic echocardiogram image showing left ventricular basal hypertrophy and moderate pericardial effusion. (D) Colour Doppler echocardiogram image showing no significant intra-cavity flow turbulence. (E–G) Gadolinium-enhanced MRI showing delayed enhancement in the lateral wall (arrow).
This case highlights the natural history of HCM with mid-cavity obstruction. Mid-cavity obstruction is seen in up to 25% of HCM cases and is due to hypertrophied papillary muscle abutting on the LV free wall during systole. Outflow obstruction may be associated with mid-cavity obstruction. Apical aneurysm formation is seen in up to 35% of patients with mid-cavity obstruction, most of whom will have normal epicardial coronary arteries. Aneurysm formation is associated with focal myocardial scarring as demonstrated by delayed enhancement in contrast-enhanced cardiac MRI. Formation of these scars is attributed to increased apical wall tension due to mid-cavity obstruction. The presence of mid-cavity obstruction is an independent determinant of unfavourable outcome. In addition, apical aneurysm formation more strongly predicted HCM-related sudden death. Apical systolic dysfunction due to apical aneurysm formation may reduce the mid-cavity gradient. Our patient developed apical myocardial infarction and there was regression of hypertrophy and loss of the previous mid-cavity gradient. Moreover, the disappearance of syncopal episodes in spite of apical myocardial infarction and LV dysfunction suggests that syncope in this patient is likely due to mid-cavity obstruction.1–3
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online video
Footnotes
-
Contributors All the authors have actively contributed to writing the article and submitting it.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.