Article Text

Abstract
Objective To investigate the impact of early oral beta blockade in patients presenting with acute non-ST elevation myocardial infarction (NSTEMI).
Methods We retrospectively identified 890 consecutive patients presenting with NSTEMI to a single UK centre from 2012 to 2014. Included patients all received standardised antiplatelet therapy plus low-dose oral bisoprolol (1.25–2.5 mg) within 4 h (mean 2.2±1.36; ‘Early Group’) or within 5–24 h (mean 15.4±5.7; ‘Late Group’) of presentation. Patients were followed up for the duration of hospital stay with the incidence of major adverse cardiovascular events (MACE—defined as ventricular arrhythmia, cardiac death or repeat infarction) set as the primary outcome. Multivariate logistic regression models analysed early versus late bisoprolol administration and adjusted for potential confounders.
Results 399 patients were included. Of the patient parameters, only the GRACE score was significantly different between the early (n=99, GRACE 164.5±29.6) and late (n=300, GRACE 156.7±31.4) groups (p=0.033). The early group had significantly fewer ventricular arrhythmias (1 vs 20, p=0.034), cardiac deaths (0 vs 13, p=0.044) and consequently MACE (1 vs 27, p=0.005) than the late group. After adjusting for the confounders of pulse, blood pressure, smoking and creatinine, logistic regression analysis identified early bisoprolol administration as protective for ventricular arrhythmia (p=0.038, OR 0.114, CI 0.015 to 0.885) and MACE (p=0.011, OR 0.064, CI 0.008 to 0.527). There was one episode of symptomatic bradycardia in the late group.
Conclusions This study suggests that low-dose oral bisoprolol administered to patients with NSTEMI within 4 h of admission may be protective and lead to reduced inpatient MACE.
Statistics from Altmetric.com
Introduction
Acute coronary syndrome (ACS) is a leading cause of morbidity and mortality worldwide, with an estimated annual incidence of 233 600 in England.1 Of these, 176 100 (75.4%) are diagnosed with unstable angina or non-ST elevation myocardial infarction (NSTEMI). In-hospital management of this cohort involves initial medical treatment with antiplatelets, anticoagulants and antianginal therapies, followed by consideration of coronary angiography and revascularisation as appropriate.1–3
The benefits of beta blockers in acute myocardial infarction (MI) are well established,4 although the mode and timing by which they are given remain debated, as indeed does the question of whether all patients within the expanding definition of MI benefit equally. They exert their therapeutic effect through a reduction in heart rate, myocardial contractility and systemic blood pressure, all of which serve to reduce myocardial oxygen requirements.
Early beta blockade (within 24 h of presentation) in acute MI has been shown to improve patient outcomes.5 ,6 The First International Study of Infarct Survival (ISIS-1) found that patients receiving intravenous atenolol within 12 h of infarction followed by 7 days oral treatment had a significantly reduced 7-day mortality compared with controls (3.7% vs 4.6%).6 Other randomised controlled trials suggest no improvement in short-term mortality, but a reduction in reinfarction and ventricular arrhythmias.7–11 Recently, a cohort study of patients with ST elevation myocardial infarction (STEMI) by Hirschl et al12 found that administering 2.5 mg of oral bisoprolol within 30 min of presentation reduced all-cause and cardiovascular mortality compared with conventional bisoprolol therapy given at 24 h.12 However, a meta-analysis of 18 studies (72 249 patients) failed to demonstrate a significant in-hospital mortality benefit for using beta blockers within 8 h of presentation in patients with acute or suspected MI.13
Beta blockers can also be harmful. There is a higher incidence of shock, bradycardia and acute heart failure in higher risk patients, particularly when administered intravenously.8 This has led to some hesitation in routine beta blockade early in the course of infarction, with one contemporary study demonstrating rates as low as one in five eligible patients with ACS receiving beta blockers within 24 h of presentation.14
Until now, a large number of these MI studies have included patients with both ST elevation and non-ST elevation infarcts, and so decisions guiding therapy have been extrapolated from heterogeneous populations. There are a limited number of focused studies, and no dedicated randomised controlled trials, investigating the effect of early beta blocker use in NSTEMI.15 ,16 An analysis of 72 054 patients with acute NSTEMI from the CRUSADE (Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA guidelines) registry found that beta blocker use in the first 24 h of admission was associated with improved outcomes and lower in-hospital mortality (3.9% vs 6.9%, p<0.001).16 The most recent European Society of Cardiology (ESC) and American Heart Association (AHA)/American College of Cardiology (ACC) guidelines for the management of NSTEMI recommend initiation of beta blocker therapy within 24 h of presentation in all patients without contraindication (box 1).2 ,3
European Society of Cardiology (ESC) and American Heart Association/American College of Cardiology (AHA/ACC) guidelines
ESC guidelines1
Patients on chronic beta blocker therapy admitted with acute coronary syndrome should be continued on beta blocker therapy if not in Killip class >II
Oral β blocker treatment is indicated in all patients with left ventricular (LV) dysfunction without contraindications
Intravenous beta blocker treatment at the time of admission should be considered for patients in a stable haemodynamic condition (Killip class <III) with hypertension and/or tachycardia
AHA/ACC guidelines2
Oral beta blocker therapy should be initiated within the first 24 h in patients who do not have any of the following: (1) signs of heart failure (HF), (2) evidence of low-output state, (3) increased risk for cardiogenic shock or (4) other contraindications to beta blockade (eg, PR interval >0.24 s, second-degree or third-degree heart block without a cardiac pacemaker, active asthma or reactive airway disease)
In patients with concomitant non-ST elevation myocardial infarction (NSTEMI), stabilised HF and reduced systolic function, it is recommended to continue beta blocker therapy with one of the three drugs proven to reduce mortality in patients with HF: sustained-release metoprolol succinate, carvedilol or bisoprolol
Patients with documented contraindications to beta blockers in the first 24 h of NSTEMI should be re-evaluated to determine their subsequent eligibility
This retrospective cohort study set out to determine if the benefits of early beta blockade in patients with NSTEMI demonstrated in large multinational registries could be seen in everyday UK practice. We additionally set out to determine if early administration of oral beta blockers (within 4 h of admission) provided any additional clinical benefit over patients treated after 4 h.
A cut-off of 4 h was prespecified to coincide with the UK Department of Health's target regarding the time taken to triage patients through the emergency department; this was felt to be an important window of opportunity for the early administration of beta blockers in a closely monitored environment. We set the null hypothesis as ‘early oral beta blocker therapy will have no effect on inpatient outcomes.’
Methods
Recruitment
Patients were identified from the Myocardial Ischaemic National Audit Project (MINAP) database for The Medway Maritime Hospital, a percutaneous coronary intervention-capable (PCI) Secondary Care Centre serving a population of 450 000 people in the south-east of England. Data were extracted for patients with a diagnosis of NSTEMI in accordance with the universal definition of MI outlined in the National Institute for Health and Care Excellence (NICE) Quality Standard 68.17 Patients with coexistent acute illnesses such as pneumonia were only included if they were diagnosed with and treated for confirmed NSTEMI. Eight hundred and ninety consecutive patients with NSTEMI were identified between 1 August 2012 and 31 July 2014, and their records were analysed for inclusion and exclusion criteria. Only patients treated with oral bisoprolol within 24 h of admission were included for analysis.
Parameters
The following parameters were recorded for each patient: age, gender, ethnicity, smoking status, presence of diabetes, admission Killip class, pulse and blood pressure, Global Registry of Acute Coronary Events (GRACE) score, serum creatinine, dose of bisoprolol given, time to antiplatelets, time to angiography, admission to a specialist cardiac bed and the presence of left ventricular (LV) impairment—defined as an ejection fraction of <40% on inpatient echo.
Exclusion criteria
The following individuals were excluded: patients with contraindications to beta blockade; patients who did not receive beta blockers within 24 h of admission; patients who suffered ventricular arrhythmia or cardiac death before prescribed beta blockers could be given; patients with previous MI; patients already on beta blockers or oral anticoagulants at the time of admission and patients with a final diagnosis other than NSTEMI, such as those with troponin release in the context of sepsis or renal impairment.
Intervention and outcomes
All included patients were treated with antithrombotic drugs—including aspirin, clopidogrel and fondaparinux—at the point of diagnosis. These agents were administered in line with the local hospital ACS protocol derived from the NICE guidelines. Patients additionally received 1.25–2.5 mg of oral bisoprolol in the emergency department within 4 h of presentation (‘Early’ group) or in the admitting ward within 5–24 h of presentation (‘Late’ group). Treatment with beta blockers was at the discretion of the admitting doctor. Patients were admitted to either specialist cardiac or non-specialist wards and were followed up for the duration of their hospital stay. All inpatient beds had access to either telemetry or bedside cardiac monitoring facilities.
The primary outcome was set as the incidence of in-hospital major adverse cardiac events (MACE—defined in this case as death, ventricular arrhythmia or repeat infarction). Ventricular arrhythmia included any documented incidences of monomorphic or polymorphic ventricular tachycardia, with or without haemodynamic compromise, or ventricular fibrillation. Arrhythmias were recorded via 12-lead ECGs, telemetry or bedside monitoring or, in the event of cardiac arrest, documented in the hospital's cardiac arrest audit proforma. Secondary outcomes included: (1) adverse drug-related events—defined as symptomatic bradycardia or hypotension (associated with presyncopal or syncopal symptoms); (2) cardiogenic shock and (3) time to bisoprolol administration.
Statistical analysis
Statistical analysis was performed using SPSS software. The Shapiro–Wilk test distinguished normally and non-normally distributed data. Categorical group parameters were compared using Z-tests. Continuous parameters were analysed using two-tailed unpaired t tests for normally distributed data or the Mann–Whitney U test for non-normally distributed data. Group outcomes were compared using Fisher's exact test, with inpatient ventricular arrhythmia and inpatient cardiac death analysed both separately and combined as MACE. Step-down, multivariate binary logistic regression models were constructed with inpatient ventricular arrhythmia or MACE as dichotomous outcome variables, and patient parameters and time to bisoprolol (h) as covariates. ‘Early bisoprolol given’ (<4 h) was also introduced as a binary exposure. Normally distributed data are presented as mean±SD and non-normally distributed data as median (IQR). ORs are provided with 95% CIs; the level of significance for all tests was set at p<0.05.
Results
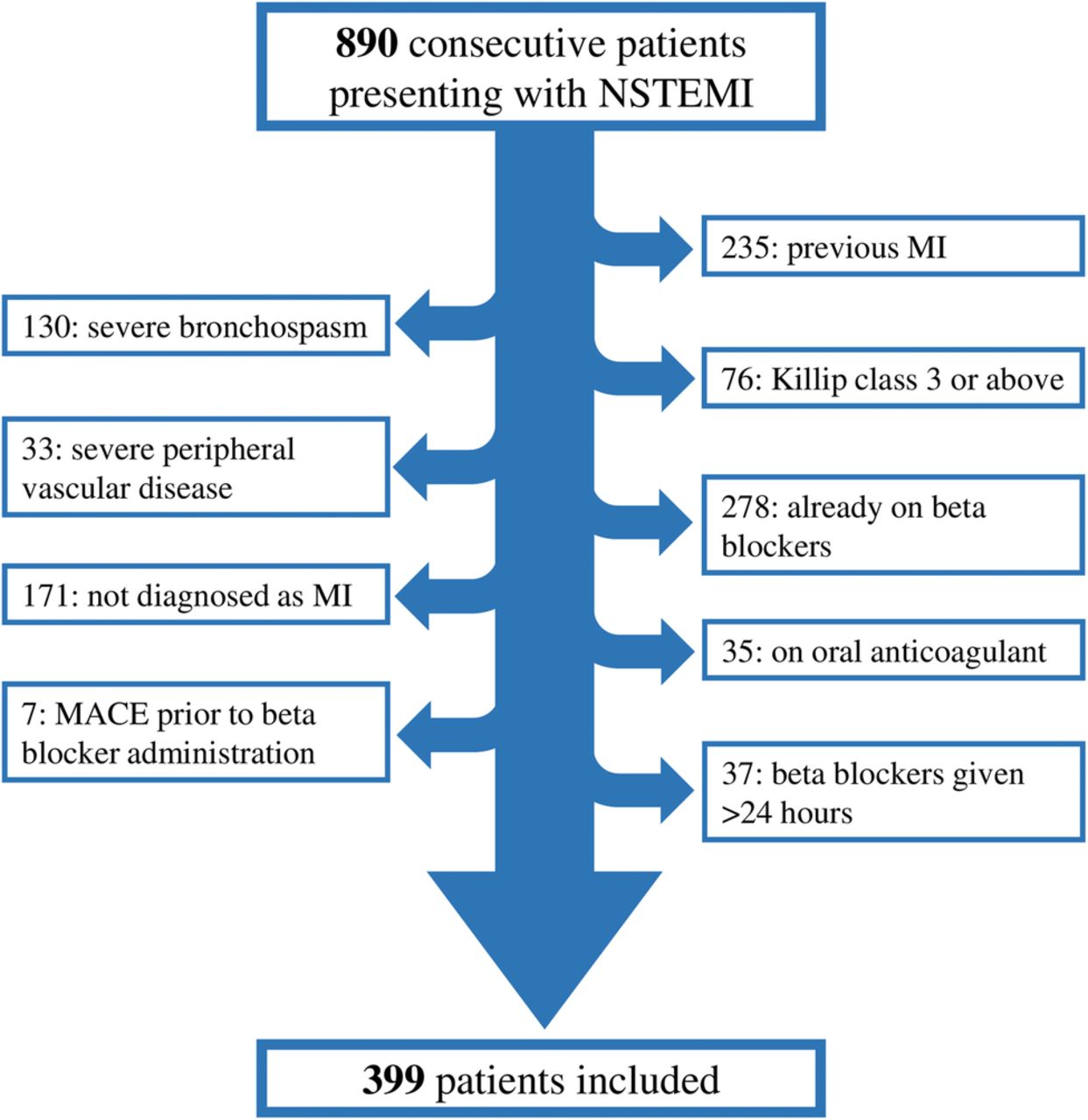
Three hundred and ninety-nine patients with NSTEMI were included in this study (figure 1). Ninety-nine patients received bisoprolol within 4 h (‘Early’ group) and 300 received bisoprolol between 5 and 24 h (‘Late’ group) of admission. All patients received concurrent triple antithrombotic therapy for 5 days or until the point of angiography or death. Patient parameters are shown in table 1. The mean time to bisoprolol was 2.2 (±1.36) h in the early group versus 15.4 (±5.7) h in the late group (p=0.001). Outcomes are shown in table 2. There were 21 occurrences of ventricular arrhythmia (15 ventricular tachycardia and 6 ventricular fibrillation) and 13 cardiac deaths. Six ventricular arrhythmias were fatal; to avoid duplication, these cases were considered as single adverse cardiac events, giving 28 MACE in total. Ninety-eight patients (24.5%) were admitted to specialist cardiac beds; on average, these patients received bisoprolol more than 4 h earlier than those admitted to non-specialist wards (8.77±6.75 h vs 13.2±7.49 h, p=0.0001).
Patient parameters in the early and late groups
Patient outcomes in the early and late groups
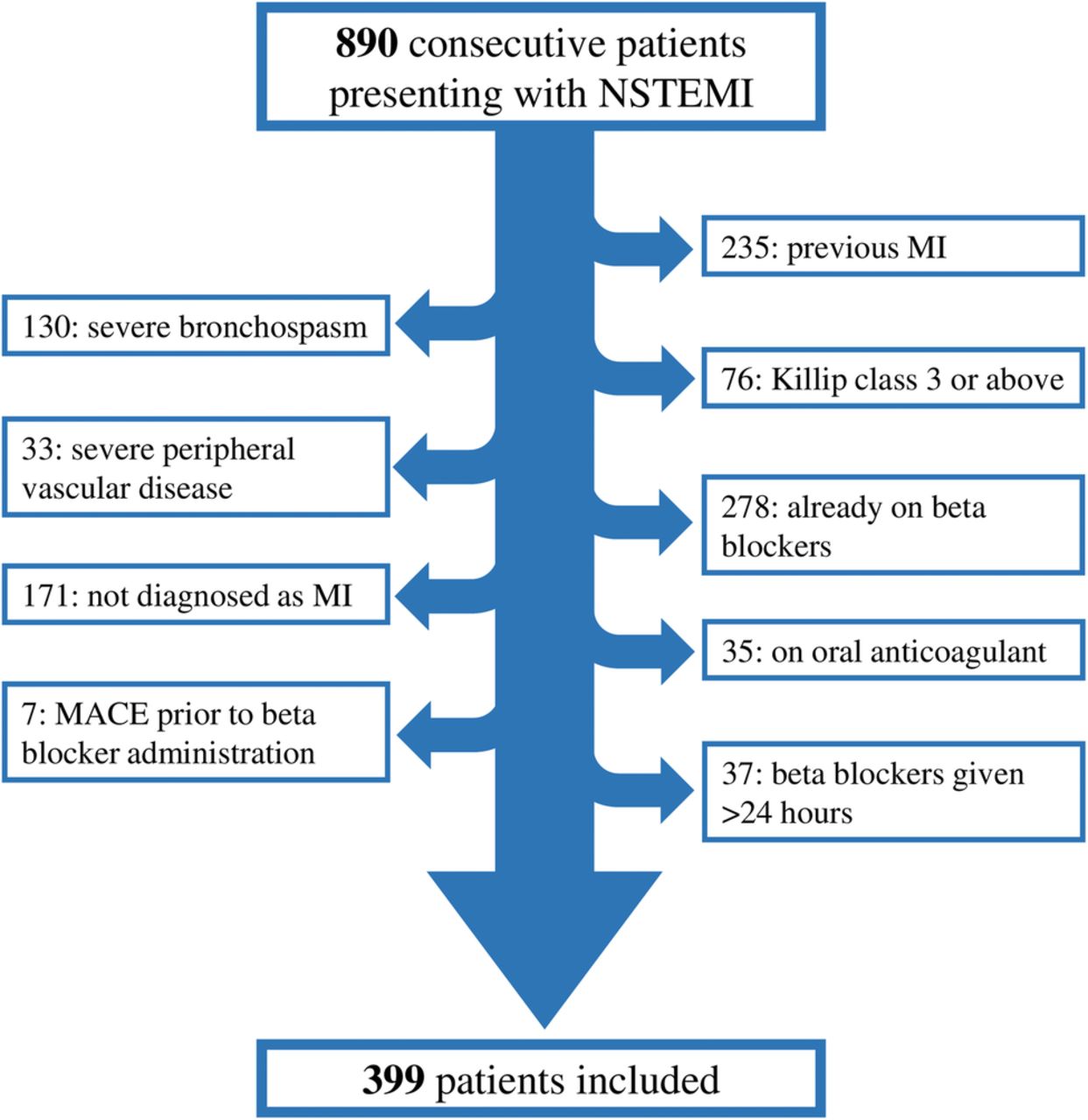
Flow diagram of patient selection. MACE, major adverse cardiovascular events; MI, myocardial infarction; NSTEMI, non-ST elevation myocardial infarction.
When compared with the late group, the early group had significantly fewer inpatient ventricular arrhythmias (1 vs 20, p=0.034), cardiac deaths (0 vs 13, p=0.044) and MACE (1 vs 27, p=0.005). All-cause mortality was not significantly different between the early (9/99=9.1%) and late (37/300=12.3%) groups (p=0.469). Admission to specialist cardiac beds was associated with reduced cardiac death (0 vs 13, p=0.044) but not ventricular arrhythmia (3 vs 18, p=0.31).
Stepwise binary logistic regression modelling of all patient parameters identified smoking status (p=0.043, OR 1.62, CI 0.128 to 16.057) and blood pressure (p<0.001, OR 0.97, CI 0.949 to 0.992) as significant predictors of ventricular arrhythmia. When adjusting for these confounders, hours to bisoprolol administration was also a significant predictor of ventricular arrhythmia (p=0.047, OR 1.071, CI 1.001 to 1.175) with R2=0.262. For predicting MACE as a whole, blood pressure (p<0.001, OR 0.961, CI 0.940 to 0.981), creatinine (p=0.028, OR 0.981, CI 0.985 to 0.998) and pulse (p=0.006, OR 1.025, CI 1.007 to 1.044) were significant. Adjusting for these confounders, hours to bisoprolol was also a significant predictor of MACE (p=0.016, OR 1.080, CI 1.014 to 1.150) with R2=0.337. Adjusted multivariate analysis did not identify admission to a specialist cardiac bed as predictive of MACE.
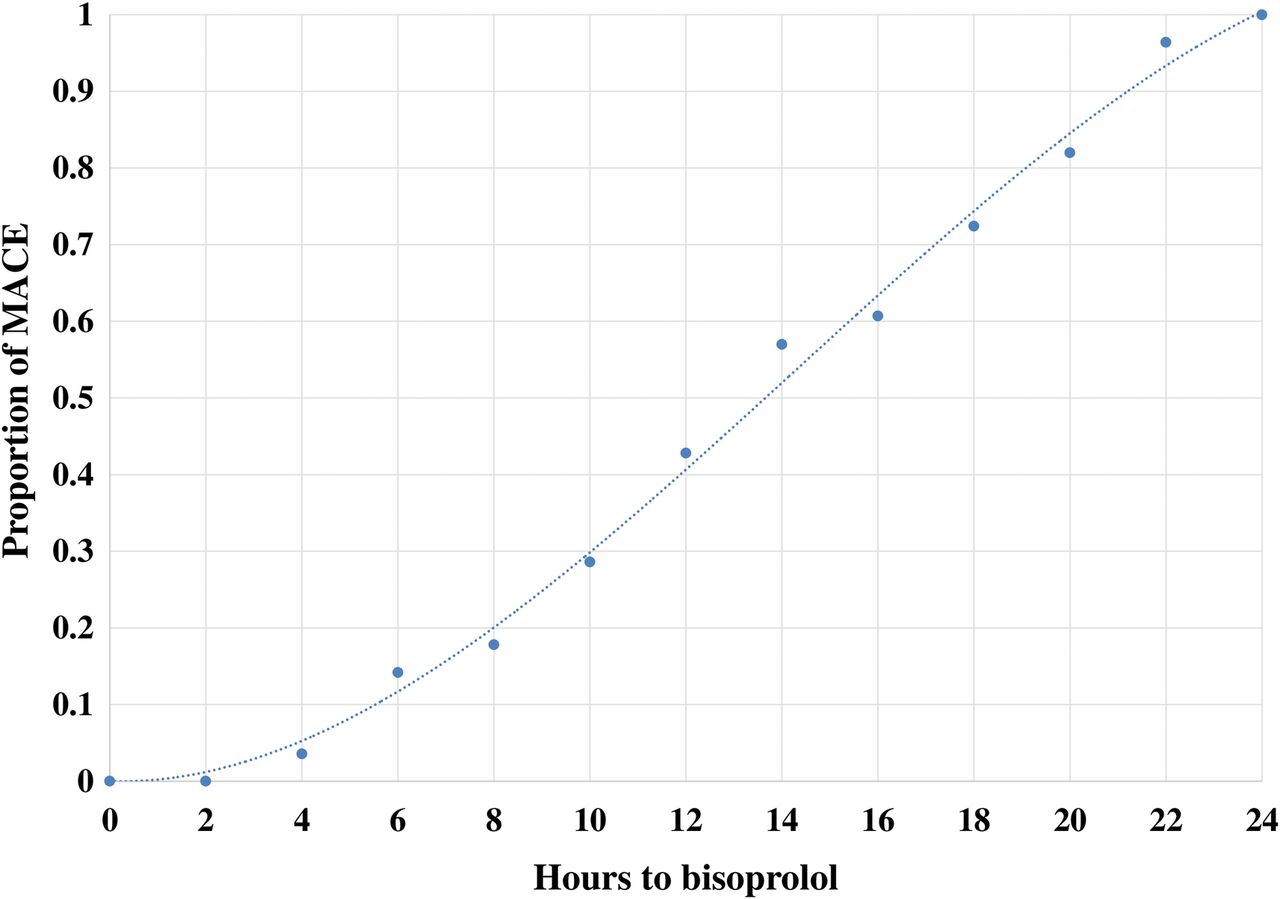
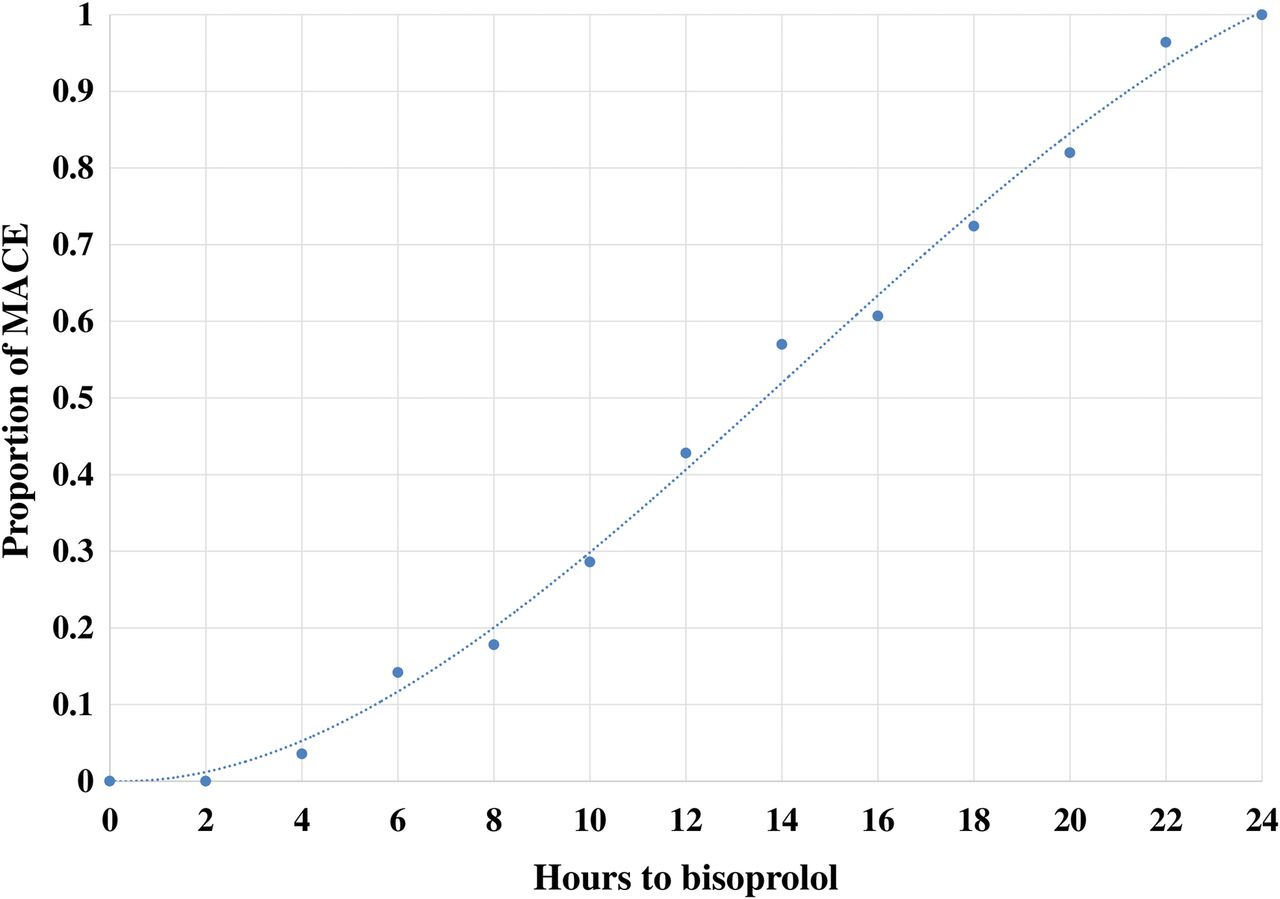
A regression plot (figure 2) was produced showing hours to bisoprolol versus the proportion of subsequent inpatient MACE (Equation: y=−1×10−04E–04x3+0.0041x2−0.0018x, R2=0.9953).
{kind=link}
{kind=link}
Regression plot showing hours to bisoprolol versus the proportion of subsequent inpatient major adverse cardiovascular events (MACE).
When substituting ‘hours to bisoprolol’ with ‘early bisoprolol given’ (<4 h) as a binary exposure, early bisoprolol administration was a significant predictor for MACE (p=0.011, OR 0.064, CI 0.008 to 0.527) and arrhythmia (p=0.038, OR 0.114, CI 0.015 to 0.885). When repeated with an 8 h cut-off, this trend attenuated for arrhythmia (p=0.092) although continued for MACE (p=0.024).
GRACE score was significantly higher in the early group (164.5±29.6) compared with the late group (156.7±31.4) (p=0.033) and was predictive of death from other causes (p<0.001, OR 1.029, CI 1.013 to 1.046). Given the difference in GRACE score between early and late groups, subgroup analysis comparing patients with low (≤139) GRACE score and high (≥140) GRACE score was performed. This showed that patients with higher GRACE (n=290) score were given bisoprolol significantly earlier than patients with lower GRACE (n=109) score (11.46±7.53 h vs 13.83±7.35 h, p=0.005). There was no significant difference in MACE between patients with higher and lower GRACE scores (23 vs 5, p=0.28).
Bisoprolol administration within 4 h reduced absolute risk of ventricular arrhythmia by 5.66% (CI 2.21% to 9.1%) with a number needed to treat of 18 (CI 11 to 45.2). For cardiac death, absolute risk reduction was 4.3% (CI 2.03% to 6.64%) with a number needed to treat of 24 (CI 15.1 to 49.3).
A single adverse event of symptomatic bradycardia requiring cessation of bisoprolol was recorded in the late group.
Discussion
This retrospective cohort study suggests that patients with NSTEMI treated with early (≤4 h) low-dose oral bisoprolol may have better in-hospital outcomes than those patients treated later (5–24 h). Our data suggest that for each hour that bisoprolol administration was delayed, the risk of subsequent inpatient MACE increased by 8%. In this patient population, bisoprolol was very well tolerated and was also cost-effective: drug administration costs £0.05 per dose, and a number needed to treat of 18 results in a cost of preventing an event of £0.90. Bisoprolol administration occurred significantly earlier in patients managed in specialist cardiac beds and in those with higher GRACE scores.
The protective effect of early bisoprolol in this patient group is likely multifactorial. Beta blockers in heterogeneous ACS populations have been shown to reduce short-term cardiac death, reinfarction and end infarct size, as well as suppress automaticity and increase ventricular fibrillation threshold.4–6 ,18–20 However, much of the key evidence for beta blockers in acute MI stems from trials using short-acting agents such as metoprolol, which have also been associated with increased incidence of cardiogenic shock, particularly following intravenous use.8 Bisoprolol shows high β1 selectivity, demonstrates excellent oral bioavailability with stable pharmacokinetics and has a half-life of 10–12 h. There is little evidence as to whether a dose–response relationship exists between the anti-ischaemic and antiarrhythmic effects of bisoprolol. Animal studies have shown that the beta blocker-mediated reduction in post-infarction ventricular arrhythmia occurs in part via central nervous system modulation,1 ,8 ,20 particularly in lipophilic agents such as bisoprolol. Accordingly, in pigs, direct injection of propranolol into the fourth ventricle of the brain is more effective in preventing ventricular fibrillation than intravenous administration, despite the latter route being associated with higher concentrations of cardiac beta blockade.21 Our very low adverse drug-related event ratio may suggest that the protective effects of early, low-dose bisoprolol occur predominantly via the vagal suppression of ventricular arrhythmia rather than by large alterations in haemodynamic status. We did not demonstrate any significant difference in outcomes between patients initially treated with 1.25 mg versus 2.5 mg of bisoprolol.
There are recognised limitations to this study. This is a retrospective, single-centre analysis of a small number of patients; however, post hoc analysis shows study power to be high with a power statistic of 0.87 (α=0.05). While our study's event ratio (28/399=7.01%) mirrors that of similar populations,15 all-cause mortality is higher. This is in line with the higher than expected mortality rates recorded at Medway Maritime Hospital;22 however, we acknowledge that this may compromise the generalisability of our study findings to other populations. Treatment with or without beta blockers was at the discretion of the admitting physician in a non-randomised fashion, and additional confounding variables not included in the multivariate analysis cannot be fully excluded. It could be speculated that the reduction in cardiac death seen in patients admitted to specialist cardiac beds may confound the protective effect of beta blockers; however, no significant association was demonstrated during regression modelling. There is discrepancy between group sizes, although patient parameters are closely matched for variance. A large number of patients (491) were excluded; the majority of these as a consequence of contraindications established in international guidelines; however, patients presenting on oral anticoagulant therapy were also excluded to ensure equal exposure to antithrombotic therapy between groups. Patients with previous MI have a higher incidence of ventricular arrhythmia and were therefore also identified as potential confounders and excluded. Previous trials suggest that the protective effect of beta blockade on mortality may be mediated by cardiac rupture;6 in our study, postmortem examination was not performed in all cases and consequently we do not have sufficient data to investigate this association. The decision to include patients with proven NSTEMI and coexistent presenting illnesses such as pneumonia reflects our efforts to provide data that are generalisable to everyday patient populations.
Conclusions
This retrospective analysis of patients with NSTEMI admitted to a single UK centre demonstrates that early treatment with 1.25–2.5 mg of oral bisoprolol within 4 h of presentation was shown to be safe and was associated with significantly improved inpatient outcomes compared with patients treated after 4 h. Further randomised controlled studies are now required to address this relationship.
Key messages
What is already known about this subject?
Early beta blockade in acute myocardial infarction has been shown to improve survival, reduce infarct size and suppress ventricular arrhythmia. Much of these data are from the thrombolysis era involving higher risk patients with ST elevation myocardial infarction. Furthermore, some studies have found an increased incidence of cardiogenic shock following early administration. Data on early beta blockade in pure non-ST elevation myocardial infarction (NSTEMI) populations, particularly using oral bisoprolol, are limited.
What does this study add?
Current European Society of Cardiology (ESC) guidelines recommend early beta blockade in eligible patients with NSTEMI, with the American Heart Association/American College of Cardiology (AHA/ACC) recommending treatment within 24 h of presentation. Our data suggest that low-dose oral bisoprolol administration to patients with NSTEMI within 4 h of presentation is safe and is associated with reduced in-hospital major adverse cardiovascular events compared with conventional therapy.
How might this impact on clinical practice?
This study suggests that low-dose oral bisoprolol should be considered in all patients presenting with a diagnosis of NSTEMI in the emergency department.
Acknowledgments
The authors thank acute coronary nurse specialist Liz Duncan (Medway Maritime Hospital) for her assistance with data collection and Dr Yanzhong Wang (King's College, London) for assistance with statistical analysis.
References
Footnotes
EM and SZ share responsibility as first author.
Contributors All authors were involved in drafting the manuscript, agree with the data analysis and the conclusions drawn and are accountable for all aspects of the work.
Competing interests None declared.
Ethics approval Medway Maritime Hospital local research ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.