Article Text

Abstract
Hypertension is a common disease, and hypertensive patients are at increased risk of cardiovascular events. The prevalence and socioeconomic burden of hypertension in the Asia-Pacific region are predicted to increase in the coming decades. Effective blood pressure lowering reduces overall cardiovascular morbidity and mortality in patients, yet doubt has been raised regarding the use of (mainly older generation) β-blockers as initial therapy in hypertension. Consequently, several international treatment guidelines do not recommend β-blockers for the treatment of hypertension. However, in contrast to first-generation and second-generation β-blockers, the third-generation, vasodilating β-blocker nebivolol has a considerably better metabolic, haemodynamic and side effect profile. In addition to providing effective blood pressure control similar to other β-blockers and drugs from other antihypertensive classes, nebivolol exerts a dual mechanism for increasing the bioavailability of the naturally occurring vasodilator nitric oxide. The clinical benefits and significance of enhancing nitric oxide levels in hypertensive patients have been shown in direct comparisons of nebivolol with other β-blockers. While β-blockers generally provide comparable blood pressure reductions, only nebivolol demonstrated enhanced vasodilation and blood flow by increasing the expression of endothelial nitric oxide synthase and therefore increasing nitric oxide release from the endothelium. In contrast to other β-blockers, therefore, it has been suggested that nebivolol has beneficial effects in several hypertensive subgroups due to its vasodilating properties. Considering the existing data, it may be timely for treatment guidelines to recommend third-generation vasodilating β-blockers as a first-line option for the pharmacotherapy of hypertension.
Statistics from Altmetric.com
Introduction
Hypertension is the most common health problem detected by primary healthcare physicians.1 Hypertensive patients are at an increased risk of cardiovascular events, especially heart disease, myocardial infarction and stroke, as well as kidney disease.2 It has been shown that 47% of ischaemic heart disease and 54% of strokes worldwide can be attributed to hypertension.3 In 2010, high blood pressure (BP) accounted for 9.4 million deaths globally, and >1.5 billion adults in the world are predicted to suffer from hypertension in 2025.4 ,5 The prevalence of hypertension ranges in the Southeast Asia and Pacific regions from 5% to 47% in men and from 7% to 38% in women, respectively,6 and is expected to further increase due to the adoption of unfavourable (Western) lifestyles and population ageing.7 Although prolonged high BP causes significant—and often irreversible—adverse health effects on various organ systems in the human body, most patients remain asymptomatic for many years. Furthermore, hypertension treatment and BP control rates in the Asia-Pacific region are generally suboptimal.7 ,8 As effective BP lowering has consistently been demonstrated to reduce overall cardiovascular morbidity and mortality,1 ,9 early detection and consequent intervention are essential.4
In 1962, based on the rationale that chest pain of ischaemic heart disease should improve by reducing catecholamine-induced effects of myocardial β-adrenoreceptor activation, Sir James Black, while at ICI pharmaceuticals (UK), made a pivotal contribution to pharmacology and clinical medicine with the development of the first β-blocker.10 Today, the class of β-blockers is typically grouped in generations. First-generation β-blockers (eg, propranolol, pindolol) are non-selective and show no vasodilation effect. Second-generation β-blockers (eg, atenolol, bisoprolol) are considered β1-selective while third-generation β-blockers (eg, carvedilol, nebivolol) show additional vasodilatory properties.
Since the early 1990s, doubt has been raised regarding the use of β-blockers as initial therapy in hypertension.11 ,12 However, it should be noted that most of the studies reporting unfavourable effects of β-blockers in hypertension therapy were conducted with atenolol.13 In contrast to first-generation and second-generation β-blockers, those of the third generation exert considerably better metabolic and haemodynamic profiles.14 Nebivolol (figure 1), as a β-blocker with β1-selectivity and nitric oxide (NO)—mediated vasodilatory benefits, is of particular interest.2 ,15
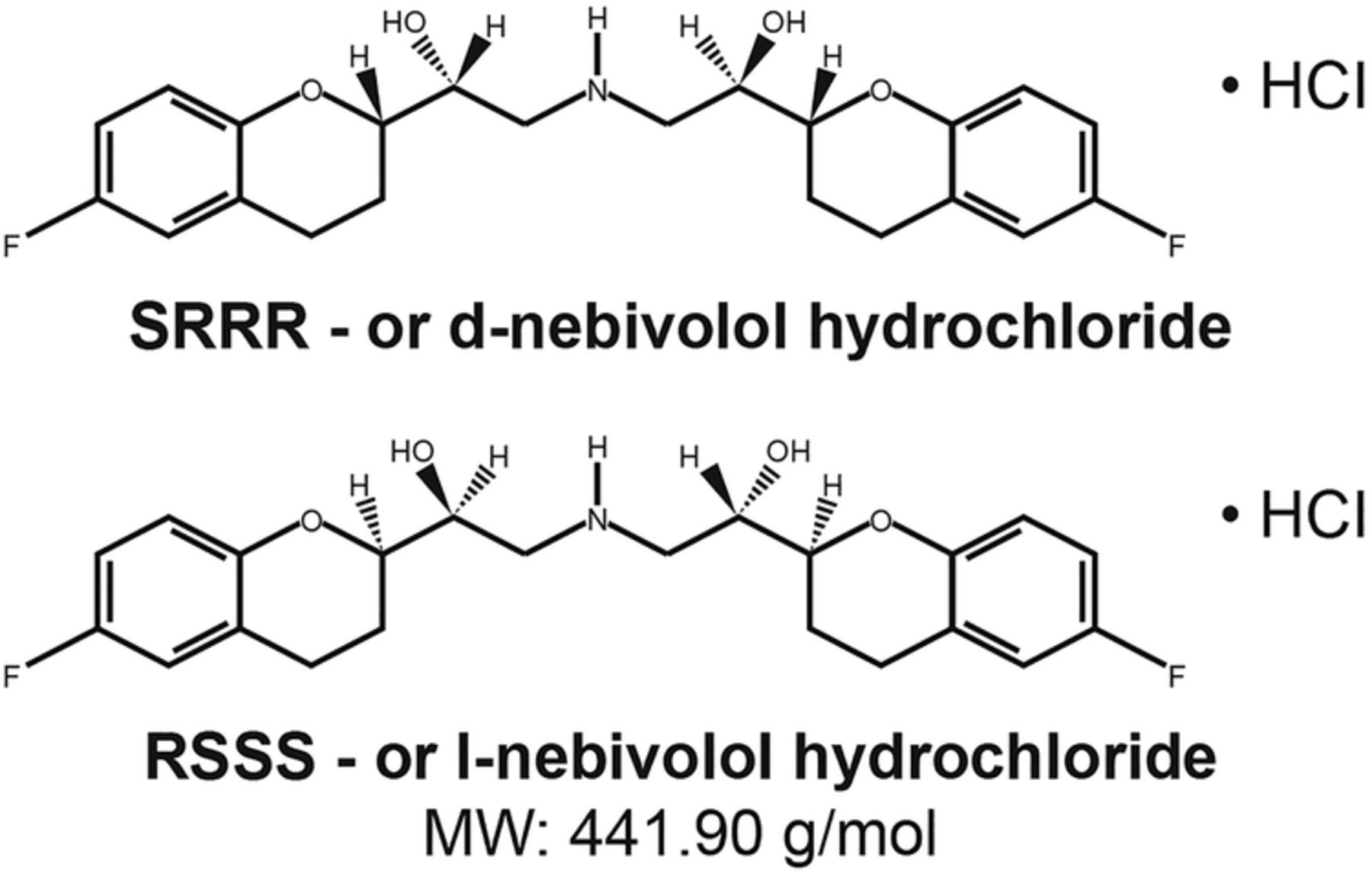
Structure of third-generation β-blocker nebivolol.
On 22 February 2014, 10 hypertension experts from the Asia-Pacific region convened for the Advisory Panel on Nebivolol in Hypertension Care meeting in Singapore. The purpose of the meeting was to analyse the role of β-blockers in BP regulation, review the current hypertension management guidelines and develop a consensus on indications for the safe and effective use of nebivolol in hypertension care.
The β-blocker setback in hypertension care
Early evidence
In 1992, a large study conducted by the Medical Research Council on British elderly patients found no benefit of atenolol against coronary events and only little protection against stroke.11 In 1998, a systematic review of trials in the elderly by Messerli et al12 revealed that the use of β-blockers as monotherapy in hypertension resulted in worse outcomes compared with diuretics.
Recent evidence
In 2005, a meta-analysis by Lindholm et al of 13 randomised clinical trials compared β-blockers (atenolol, metoprolol, propranolol and oxprenolol) to other hypertensive drugs in the treatment of hypertension. The authors found a 16% increase in relative risk of stroke with β-blockers compared with other drugs. In comparison to placebo or no treatment, the risk reduction for stroke using β-blockers was only about half in comparison to other antihypertensive medication.16 An increase of new-onset diabetes in β-blocker-treated patients was reported in 2007.17 Furthermore, Bangalore et al18 noticed greater reduction in heart rate was associated with higher risk of cardiovascular events. Finally, two recent large-scale hypertension trials (LIFE and ASCOT studies) demonstrated a clear superiority of newer antihypertensives over atenolol and the combination with diuretics.19 Likewise, a meta-analysis by Khan and McAlister provides no evidence for a reduction in mortality, myocardial infarction or stroke in younger patients treated with β-blockers.20 Box 1 summarises the main reasons for the lack of cardiovascular protection provided by older generation β-blockers.
Suggested main reasons for the lack of cardiovascular protection provided by (older) β-blockers21
Suboptimal antihypertensive effects
Unfavourable haemodynamics
Reduced compliance due to many adverse effects
Reduced effect on left ventricular hypertrophy
Unfavourable metabolic effects (lipid and glucose metabolism)
Guidelines for the management of high BP
The 2014 evidence-based guidelines for the management of high BP in adults, based on a report from the panel members appointed to the Eighth Joint National Committee (JNC8), do not recommend β-blockers as first-line therapy for hypertension (Recommendation 6). The negative evaluation of β-blockers was mainly due to their unfavourable effects compared with angiotensin II receptor blocker (ARB).1 Similarly, the British Hypertension Society stated in their 2011 National Institute for Health and Care Excellence (NICE) guidelines that “β-blockers are not a preferred initial therapy for hypertension”. However, the guidelines also indicated that β-blockers may be considered in younger people, particularly in certain subpopulations, for example, those with an intolerance or contraindication to angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor antagonists; women of childbearing age; or people with evidence of increased sympathetic drive.21
In contrast, the Canadian guidelines recommend all drug classes as suitable for initial hypertension therapy with the exception of patients older ≥60 years for whom β-blockers are not recommended.22 Likewise, in contrast to the British and American JNC8 recommendations, the 2013 European Society of Cardiology/European Society of Hypertension (ESC/ESH) guidelines recommend that ACE inhibitors, ARBs, β-blockers, calcium channel blockers (CCBs) and diuretics are all suitable for both the initiation and maintenance of antihypertensive therapy either as monotherapy or in certain combinations.23 Also in agreement with the above recommendations are hypertension guidelines from several Asian countries, for example, China, Korea, India, Indonesia and Singapore, which all consider β-blockers as a potential first-line option for hypertension.8 Box 2 summarises the recommendations common to current hypertension guidelines.
Recommendations common to all contemporary hypertension guidelines (adapted from Jennings and Touyz (2013) with slight modifications)24
Blood pressure (BP) is a continuous variable but for practical purposes is broken down into grades
Measure BP carefully
High BP is associated with adverse prognosis
High BP is especially adverse for people who have extensive vascular disease, multiple cardiovascular risk factors, diabetes mellitus or renal disease
Assess total cardiovascular risk
Lifestyle measures come first when attempting to lower BP, cardiovascular risk and improving responses to antihypertensive drugs
Drugs come next, generally initial monotherapy followed by combinations
Combinations from different drug classes are generally good; combinations sharing similar actions are generally not advised
Taken together, recommendations in certain hypertension management guidelines have been based on negative clinical data with some β-blockers, and atenolol in particular.13 The widely existing ‘β-blocker phobia’ is largely due to unfavourable outcome results of specific β-blockers in clinical trials, especially those of the first and second generation. However, not all β-blockers are the same. In fact, the 2009 reappraisal of the ESH/ESC guidelines highlighted that β-blockers are indeed suitable for initial therapy in hypertension and that highly β1-selective blockers or those with vasodilatory effects may be preferred as first-line antihypertensive agents.24
The third-generation β-blocker nebivolol has both the highest β1-cardioselectivity and vasodilatory benefits that are mediated by the l-arginine/NO pathway. As discussed in detail below, nebivolol shows similar efficacy compared with other monotherapies in hypertension treatment, often with fewer adverse effects.2 ,25 In addition, the antioxidant and NO-releasing properties of nebivolol have been suggested to attenuate oxidative stress and endothelial dysfunction and thus to provide added benefits for patients receiving antihypertensive treatment.2 ,25
Nebivolol: mechanisms of action and clinical efficacy in BP regulation
Basic pharmacokinetic and pharmacodynamic data for nebivolol
Nebivolol is a racemic mixture made up of equal amounts of d- and l-nebivolol. Compared with other currently available β-blockers (such as metoprolol, bisoprolol and carvedilol), nebivolol is the most selective β1-adrenoreceptor antagonist in the human myocardium with a 321-fold higher selectivity for β1-adrenoreceptors compared with β2-adrenoreceptors.26 The D-isomer of nebivolol is mainly responsible for the selective β1-adrenoreceptor antagonist activity, while the L-isomer primarily contributes to the vasodilating properties of nebivolol.27
Whereas carvedilol exerts vasodilating effects via α1-receptor blockade, nebivolol stimulates the endothelial l-arginine/NO pathway and thus increases the bioavailability of the naturally occurring vasodilator NO (figure 2).2 ,25 This effect was first demonstrated in isolated canine coronary arteries where vasodilation by nebivolol was shown to be endothelium-dependent and sensitive to blockade by NO inhibitors.28

{kind=link}
{kind=link}
Dual mechanism of action for the antihypertensive effects of nebivolol. eNOS, endothelial nitric oxide synthase; NO, nitric oxide.
A starting dose of nebivolol 5 mg once daily is recommended for most patients with hypertension.29 A single dose of nebivolol allows 24 h control of BP, exerting a constant antihypertensive action that respects the physiological circadian rhythm.30 ,31 Upon oral administration, nebivolol is absorbed rapidly and unaffected by food.27 In the circulation, approximately 98% of nebivolol is protein bound.27
Clinical efficacy and tolerability of nebivolol
Several studies have clearly established that the antihypertensive efficacy of nebivolol is similar to that of other β-blockers, for example, atenolol and bisoprolol.32 ,33 In addition, a study has also demonstrated that intervention with nebivolol, but not with metoprolol succinate, resulted in significantly reduced central systolic and diastolic BPs, central pulse pressure and left ventricular wall thickness in hypertensive patients (aged 30–65 years) treated for 1 year.34 Furthermore, whereas no significant difference has been found between bisoprolol and atenolol in terms of reduction of aortic pulse pressure after 12 weeks of treatment,35 nebivolol reduced aortic pulse pressure to a greater extent than atenolol,36 and yet affects a less pronounced impact on augmentation index (AIx).37 In fact, in contrast to most other antihypertensive drugs, the majority of ß-blockers cause an increase in AIx values.38 However, recent data strongly indicate an AIx-reducing potential for nebivolol. Compared with carvedilol and metoprolol, nebivolol treatment resulted in a statistically significant reduction of heart rate-adjusted AIx values.39 Results from the Conduit Artery Function Evaluation (CAFÉ) study indicate that even a 3 mm Hg reduction in central pulse pressure has been associated with better cardiovascular outcomes40; hence, these observations may be of substantial clinical relevance. While conventional brachial BP measurement is simple and has remained the gold standard for the measurement of BP, data on central BP are of particular interest as this parameter has been suggested to be a more accurate predictor of cardiovascular risk and response to antihypertensive therapy.41
In vivo, the clinical significance of the ability to modify NO levels has been shown in a direct comparison of nebivolol with atenolol in hypertensive patients. Whereas treatment with both β-blockers resulted in comparable BP reduction, only nebivolol enhanced vasodilation and blood flow by increasing the expression of endothelial nitric oxide synthase and therefore increasing NO release from the endothelium.42 Similarly, nebivolol, but not bisoprolol, significantly increased flow-mediated endothelial-dependent vasodilation and thus endothelial function.43
Because of its vasodilating properties, nebivolol also offers beneficial hemodynamic effects in hypertensive patients. Unlike non-vasodilating β-blockers, nebivolol increased stroke volume at preserved cardiac output in several clinical trials.44 ,45 Furthermore, in contrast to bisoprolol, nebivolol does not lead to a reduction in cardiac index (ie, the ratio of cardiac output to body surface area).45 The favourable haemodynamic profile of nebivolol (ie, preservation of cardiac output and index, reduction of peripheral resistance and improved diastolic function) might thus provide hypertensive patients with clinically relevant benefits regarding the impairment of systolic and/or diastolic function.46
The efficacy and side effect profile of nebivolol has also been tested against several other antihypertensive drug classes. In trials comparing nebivolol against CCBs (eg, amlodipine), similar response rates in the BP-lowering effects between the active treatment groups were found. However, side effect rates were significantly lower for nebivolol.47 In two separate studies, the reduction of diastolic BP with nebivolol (5 mg/day) was similar to that achieved with lisinopril (20 mg/day)48 but greater than that achieved with enalapril (10 mg/day).49 In comparison to losartan (50 mg/day), the number of patients with normalised BP was significantly higher with nebivolol (5 mg/day) after 6 weeks, although after 12 weeks, the results were similar between treatment groups. Of note, patients treated with nebivolol benefited not only from a significantly greater reduction of diastolic BP but also from a better quality of life compared with those in the losartan group.50
Support for the efficacy and favourable side effect profile of nebivolol also originates from a recent meta-analysis of 13 randomised controlled trials in which nebivolol was compared in nine studies with a variety of other antihypertensive drugs (ACE inhibitors (enalapril, lisinopril), other β-blockers (atenolol, bisoprolol, metoprolol), an ARB (losartan) and CCBs (amlodipine, nifedipine)) and in other studies with placebo. Overall, nebivolol achieved similar or better rates of treatment response and BP normalisation than drugs from other classes and other antihypertensive drugs combined, with similar tolerability to placebo and significantly better tolerability.51 Due to its vasodilating properties, nebivolol has shown beneficial effects in minimising erectile dysfunction in contrast to other β-blockers.52
Furthermore, disturbance of lipid metabolism, carbohydrate metabolism/insulin signalling and risk of new-onset diabetes are significantly lower in nebivolol-treated patients compared with other β-blockers.2 ,25 In the SENIORS trial, nebivolol was associated with fewer cases of new-onset diabetes mellitus than placebo (1.8% nebivolol vs 2.1% placebo); these differences, however, were not statistically significant.53 In hypertensive patients with type 2 diabetes, treatment with nebivolol did not result in any adverse effects with respect to lipid or glycaemic control.54 In an efficacy safety study of 6356 mild-to-moderate essential hypertensive patients or patients with isolated systolic hypertension, no serious adverse events were associated with nebivolol and there were no reports of cold extremities, a common side effect of other β-blockers.55 In agreement with other reports, the study further revealed a very similar efficacy of nebivolol both as mono and add-on therapy.
Treatment practice: where does nebivolol fit in?
As highlighted by ACCF/AHA 2011 Expert Consensus and the ESH/ESC reappraisal in 2009, nebivolol does not exert the adverse effects commonly seen in older generation β-blockers, particularly depression, sexual dysfunction, reduced exercise capacity, as well as lipid and glucose dyshomeostasis.56 Therefore, it is important for cardiologists and general medical practitioners to be aware that β-blockers do not comprise a homogenous class, but possess distinct strengths and weaknesses that must be carefully evaluated in order to provide hypertensive subjects with patient-tailored treatment plans. In particular, physicians of hypertensive patients need to evaluate β-blockers regarding their pharmacokinetic properties (eg, lipophilic vs hydrophilic drugs, drug clearance), mechanism of action, adverse events (eg, cardiovascular, metabolic, pulmonary, central effects, sexual dysfunction), contraindications and drug interactions. Hence, each treatment strategy should be tailored based on individual circumstances, patient preferences and drug tolerability; only then are optimised BP control rates likely to be achieved. When compared with currently available β-blockers and other antihypertensive agents, nebivolol may have advantages in several patient subgroups:
First, compelling evidence indicates that nebivolol has no negative effects on pulmonary airways and is clinically well tolerated in hypertensive patients suffering from COPD.57
Second, due to its 24 h coverage,30 ,31 nebivolol is a good choice in cases of poor compliance.
Third, in comparison to older β-blockers, nebivolol appears to have more favourable effects on erectile function in hypertensive men. Three months after switching to nebivolol, patients with no erectile dysfunction increased from 34% to 50% and those with severe erectile dysfunction decreased from 18% to 5%.52 These favourable effects are likely associated with nebivolol's effect on the bioavailability of NO.2 ,58 This makes nebivolol an ideal β-blocker for male hypertensive patients.
Fourth, based on its dual mode of action, nebivolol may be particularly beneficial in patients with difficult-to-treat hypertension (eg, the elderly, diabetics, obese patients), in whom NO-mediated endothelial dysfunction may be more pronounced.25 In 2003, Kamp et al59 reported that nebivolol not only preserved cardiac output and increased stroke volume but also induced a reduction in peripheral resistance. Due to different modes of action, these vasodilating properties are not found in older generation β-blockers.
Conclusion
Hypertension is a major risk factor for cardiovascular diseases and other end-organ damage and is thus a leading cause of morbidity and mortality.1 The prevalence, and consequently socioeconomic burden, of hypertension in the Asia-Pacific region is predicted to increase significantly in the coming decades.5 ,6 Unfortunately, current awareness of hypertension is low and the use of antihypertensive drugs is suboptimal in many countries. Although β-blockers are generally effective in reducing elevated BP either as mono or add-on therapy, several recent reviews and guidelines, especially those published by JNC8 and the British Hypertension Society (NICE guidelines), do not recommend β-blockers as first-line antihypertensive interventions,1 ,21 even though most studies on β-blockers that were included in the analysis were conducted with the second generation, only β1-selective drug atenolol.13
However, as the 2013 ESC/ESH guidelines highlight, β-blockers are not all alike; in particular, vasodilating β-blockers do not share some of the limitations of traditional β-blockers.23 Among the third-generation vasodilating β-blockers, nebivolol may be particularly suitable as a first-line treatment for hypertension. The recommendation is based on clinical data, indicating that in addition to providing effective BP control similar to other β-blockers and antihypertensive drugs, nebivolol's dual mode of action for increasing the bioavailability of the vasodilator NO may be of particular benefit to hypertensive patients.2 ,25 ,60
Acknowledgments
The authors would like to thank Ruth Schaffer of MIMS Pte Ltd for providing editorial support with collating author feedback and incorporating revisions.
References
Footnotes
Contributors All authors attended the consensus meeting and contributed to the development of consensus recommendations on use of nebivolol in hypertension. All authors reviewed and had input drafting and revising the manuscript, and approved the final version prior to submission. The manuscript is based on equal contribution of all authors present during the expert meeting: (1) pre-meeting author survey; (2) experts input during the workshop, roundtable discussions and drafting of the manuscript; (3) authors recommendation of cited references; and (4) reviewing, editing and final approval of manuscript draft.
Competing interests A. Menarini Asia-Pacific Pte Ltd provided logistic support and funding for the consensus meeting, and the authors received fair market honorarium for their time spent attending the consensus meeting and developing the manuscript. A. Menarini Asia-Pacific Pte Ltd also paid for MIMS Pte Ltd to provide editorial support. C-HK, PB, RK, CHL, S-HP and BW reports personal fees from A. Menarini Asia-Pacific Pte Ltd, during the preparation of this manuscript. NA and GR reports personal fees from A. Menarini Asia-Pacific Pte Ltd, during the preparation of this manuscript; personal fees from A. Menarini Philippines, Inc, outside the submitted work. NVP reports personal fees from A. Menarini Asia-Pacific Pte Ltd during the preparation of this manuscript, and from Servier, Sanofi, Astra Zeneca, Merck, MSD, Bayer, United Pharma International, Abbott, Pfizer, and Tedis, outside the submitted work. PLL reports personal fees from A. Menarini Asia-Pacific Pte Ltd, during the preparation of this manuscript; personal fees from Merck Serono Pharmaceuticals, outside the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.