Article Text

Abstract
Objectives There have been limited data regarding the prediction of cardiac benefits after renal artery stenting for patients with atherosclerotic renal artery disease (ARAD). The aim of this multicentre retrospective study was to identify clinical or echocardiographic factors associated with improvements of cardiac symptoms after renal artery stenting.
Methods We enrolled 58 patients with de novo ARAD undergoing successful renal artery stenting for heart failure, angina or both between January 2000 and August 2015 at 13 hospitals.
Results Improvement of cardiac symptoms was observed in 86.2% of patients during a mean follow-up of 6.0±2.7 months. Responders demonstrated significantly lower New York Heart Association functional class, higher estimated glomerular filtration rate, lower serum creatinine and lower interventricular septal wall thickness (IVS), lower left ventricular mass index, lower left atrial dimension and lower E-velocity than non-responders. Backward stepwise multivariate analysis identified IVS as an independent predictor of improvement of cardiac symptoms (OR 0.451, 95% CI 0.209 to 0.976; p=0.043). According to receiver operating characteristic curve analysis, an IVS cut-off of 11.9 mm provided the best predictive value, with sensitivity of 71.4%, specificity of 75.5% and accuracy of 73.5%. The positive predictive value was 74.5% and the negative predictive value was 72.5%.
Conclusions This multicentre retrospective study shows that the echocardiographic index of IVS is an independent predictor for improvement of cardiac symptoms after renal artery stenting.
- Renovascular Disease
- Renal Stenting
- Heart Failure
Statistics from Altmetric.com
Introduction
Cardiac disorders related to atherosclerotic renal artery disease (ARAD) are an important clinical entity in the field of cardiovascular medicine.1–3 Although recent prospective randomised studies failed to demonstrate the advantage of renal artery stenting over medical therapy in terms of controlling blood pressure and renal function and preventing cardiovascular events, it is not possible to enrol patients with fluctuating clinical conditions, who are most likely to benefit from renal artery stenting, in randomised studies.4 In the most updated statement,5 cardiac disorders such as heart failure and unstable angina are categorised as appropriate clinical indications for renal revascularisation. The aim of this study was therefore to identify predictors of cardiac benefits after renal artery stenting.
Methods
The PREMIERE registry (Predictors of Cardiac Benefits of Renal Artery Stenting from A Multicenter Retrospective Registry) is a multicentre retrospective registry consisting of patients with de novo ARAD who underwent successful renal artery stenting for the control of heart failure, angina or both between January 2000 and August 2015 at 13 vascular centres in Japan. The diagnosis of heart failure and angina pectoris was based on the physician’s clinical judgement with reference to criteria in the Framingham study and the previous guidelines.6 7 Renal artery stenting was performed according to standard procedures. All patients received dual antiplatelet therapy before the procedure. The choice of stent type and route of vascular access was left to the individual operator’s discretion. Follow-up examinations, which included evaluation of clinical symptoms and blood pressure, blood testing and echocardiography, were conducted before discharge and within 12 months.
Subjects were categorised as responders or non-responders. Responders were defined as patients demonstrating improved cardiac symptoms during the follow-up period, such as achieving a lower New York Heart Association (NYHA) functional class and no re-hospitalisation for heart failure, angina or both. Non-responders were defined as patients showing no improvement of cardiac symptoms. The institutional review boards in each institute approved the study.
Clinical and echocardiographic parameters
The preinterventional clinical and echocardiographic variables of enrolled patients were retrospectively reviewed at each institution. Clinical variables including risk factors, concomitant vascular disease, NYHA class, blood pressure, renal function and B-type natriuretic peptide (BNP) were abstracted. The echocardiographic data included the left ventricular dimension in diastole and systole, interventricular septal wall thickness (IVS), posterior wall thickness (PWT), left ventricular mass index (LVMI), left atrial dimension (LAD), left ventricular ejection fraction, peak early diastolic mitral inflow velocity (E-velocity), peak early diastolic mitral annular velocity in the septum (e′-velocity), and E/e′ ratio. LVMI was calculated as left ventricular mass (LVM)/body surface area (BSA). LVM was calculated using the modified Devereux formula.8 BSA was calculated using the formula of Du Bois and Du Bois.9
Sample size determination
Assumptions for sample size calculations were based on previous studies of the effect of renal artery stenting on angina or heart failure.10 11 Forty patients were needed with the assumption of a 10% drop out. This sample size would allow 75% effectiveness of renal artery stenting to be detected by a two-sided exact test for one proportion with power 0.9 and α=0.05 using PASS 14 (NCSS, Kaysville, Utah, USA).
Statistical analysis
Data are expressed as mean±SD or number (%). Categorical data were compared using the χ2 test or Fisher exact test. Differences between the two independent cohorts were evaluated with the Student t-test or Welch t-test for parametric continuous variables or the Mann–Whitney test for non-parametric continuous variables. Normality for distributions of continuous variables was determined using the Shapiro–Wilk test. Changes in blood pressure and renal function were assessed using one-way repeated analysis of variance with Bonferroni’s post hoc test or Friedman test. All variables tested in univariate analysis with p<0.15 were included in a multivariate logistic regression analysis with backward stepwise selection. Considering the correlations between estimated glomerular filtration rate (eGFR) and serum creatinine and between E-velocity and E/e′, serum creatinine and E-velocity were excluded from the multivariate model to avoid multicollinearity using variation inflation factors. p<0.05 was considered significant. Statistical analysis was performed with SPSS Version 22 (SPSS, Chicago, Illinois, USA).
Results
Clinical and echocardiographic characteristics
Fifty-eight patients were enrolled in the registry. The baseline clinical characteristics of the study subjects are shown in table 1. The average age was 74.4±10.2 years (range 47–90 years). The most common atherosclerotic risk factor was hypertension. As for concomitant atherosclerotic disease, coronary artery disease was most frequent, followed by peripheral artery disease. Bilateral ARAD undergoing bilateral renal artery stenting was observed in 20.7%. Baseline echocardiographic characteristics are shown in table 2. The ejection fraction was 54.3±13.7% and E-velocity/e′-velocity in the septal wall was 18.6±8.1, suggesting preservation of left ventricular systolic function and impairment of left ventricular diastolic function.
Baseline clinical characteristics
Baseline echocardiographic characteristics
Responders versus non-responders
During the mean follow-up time of 6.0±2.7 months (range 1–12 months), systolic and diastolic blood pressure significantly decreased whereas the number of antihypertensive agents and renal function remained unchanged (table 3). With respect to cardiac benefits, 50 patients (86.2%) were responders and 8 (13.8%) were non-responders. Comparisons of clinical variables between responders and non-responders are shown in table 4. Responders demonstrated significantly lower NYHA functional class, higher eGFR and lower serum creatinine than non-responders. Comparisons of echocardiographic variables between responders and non-responders are shown in table 5. Responders showed significantly lower IVS, LVMI, LAD and E-velocity than responders. The IVS:PWT ratio was numerically lower in responders than in non-responders (0.99 vs 1.10, p=0.221), but the difference was not significant. Backward stepwise multivariate analysis using these variables with p<0.15 (hypertension, diabetes mellitus, NYHA class, eGFR, IVS, LVMI, LAD and E/e′) identified a cardiac parameter, IVS, as the only independent predictor of improvement in cardiac symptoms (OR 0.451, 95% CI 0.209 to 0.976; p=0.043), and both eGFR (p=0.070) and E/e′ (p=0.097) were not significant in the final step of the analysis.
Blood pressure and renal function before and after renal artery stenting
Comparison of clinical variables between responders and non-responders
Comparison of echocardiographic variables between responders and non-responders
Receiver operating characteristic curve analysis
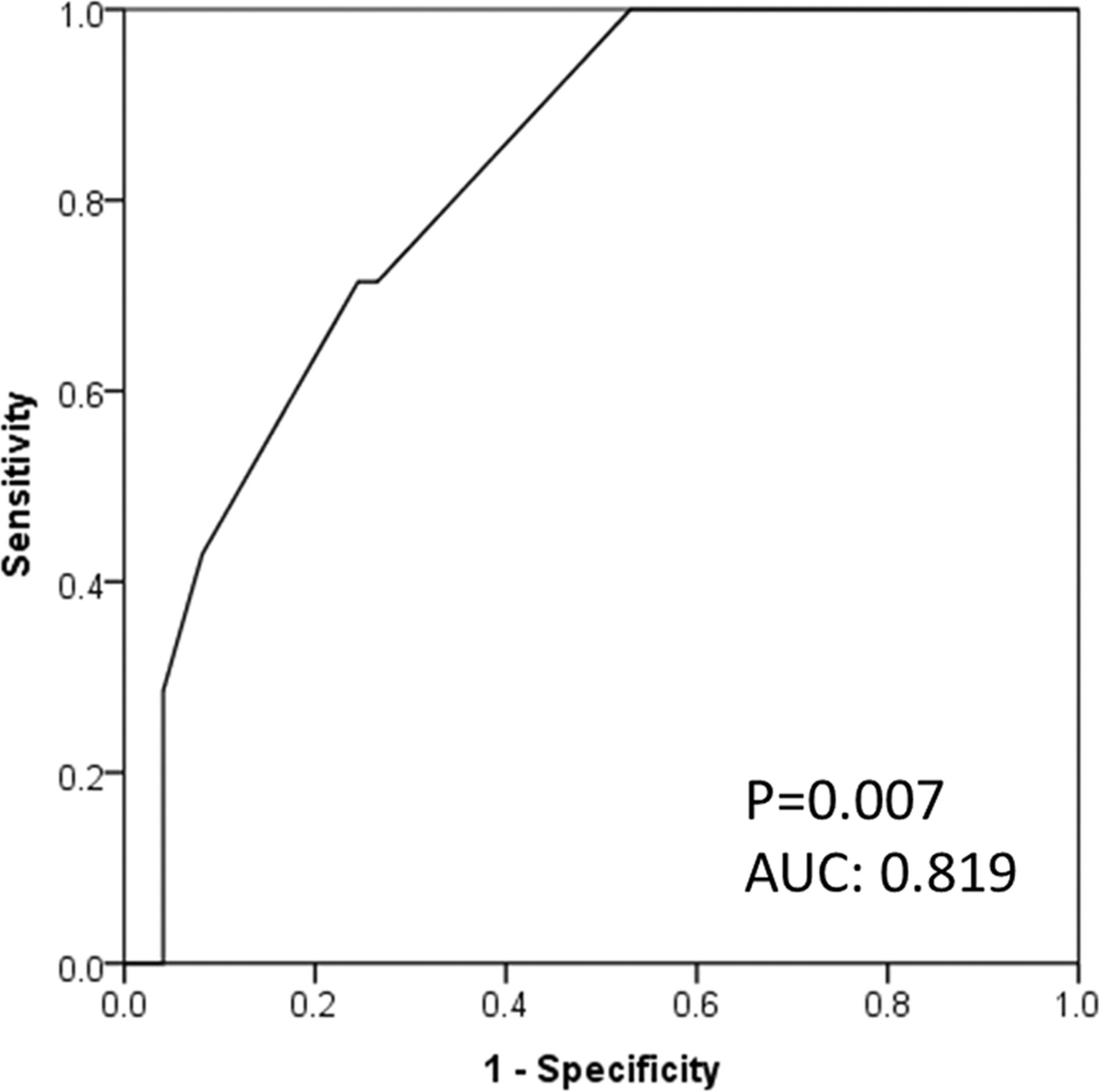
A receiver operating characteristic (ROC) curve, illustrating the accuracy of IVS for predicting the improvement of cardiac symptoms, is shown in figure 1. The area under the ROC curve was 0.819 (95% CI 0.683 to 0.956; p=0.007). An IVS cut-off value of 11.9 mm provided the best predictive value with sensitivity of 71.4%, specificity of 75.5% and accuracy of 73.5%. The positive predictive value was 74.5% and the negative predictive value was 72.5%.

{kind=link}
Receiver operator characteristic curve for interventricular septal wall thickness (IVS); a cut-off of 11.9 mm best predicted the improvement of cardiac symptoms.
Discussion
Given an increasing awareness of the relationship between ARAD and cardiac disorders and the effects of renal artery stenting on cardiac disorders,1 the present study investigated predictors of improvement of cardiac symptoms after renal artery stenting in patients with ARAD. The main findings of this study were as follows: (1) 86.2% of the patients were responders; (2) in univariate analysis, NYHA functional class, renal function (eGFR and serum creatinine) and four echocardiographic indices (IVS, LVMI, LAD and E-velocity) were significantly associated with improvement of cardiac symptoms; (3) multivariate analysis showed IVS to be the strongest independent predictor of improvement in cardiac symptoms; and (4) an IVS of 11.9 mm best predicted improvement of cardiac symptoms, with a sensitivity of 71.4%, specificity of 75.5%, and accuracy of 73.5% in ROC curve analysis.
There is discordance between the very high (>95%) procedural success rate for renal revascularisation and the moderate (60–70%) clinical response rate for the treatment of hypertension and renal failure.12 Previous investigators identified several predictors of improvement in blood pressure and renal function. Predictors of blood pressure improvement include baseline systolic or mean blood pressure, renal parenchymal thickness, number of antihypertensive agents, bilateral disease, renal fractional flow reserve, BNP, translesional pressure gradient and renal frame count. Predictors of renal function improvement include baseline serum creatinine, percentage diameter stenosis, rapid increase in serum creatinine, bilateral revascularisation and left ventricular function.13–24 These findings suggest that factors predicting a better response after renal revascularisation are distinct for different target endpoints. However, there is a paucity of data regarding the prediction of cardiac benefits after renal artery stenting.
Sutters et al and Pickering et al initially reported the cardiac benefits of balloon renal angioplasty approximately three decades ago.25 26 In the stent era, Khosla et al reported that cardiac symptoms improved by 24 hours after renal artery stenting in 88% of patients, and clinical benefits were sustained in 72.5% of patients with a mean follow-up of 253±192 days.10 Subsequent single-centre retrospective studies reported improvements in heart failure and angina symptoms, number of hospitalisations for heart failure, proportion hospitalised for heart failure and time to hospitalisation for heart failure after renal artery stenting.11 27 28 The response rate of renal artery stenting for cardiac disorders was in the range of 72.0% to 88.0%.2 10 11 27 28 In the present multicentre retrospective study, 86.2% of patients experienced improvement of cardiac symptoms during the mean follow-up period of 6.0±2.7 months, a finding consistent with the previous studies.
The present study, which employed cardiac symptoms as an endpoint in univariate analysis, found that NYHA functional class, renal function and echocardiographic indices such as IVS, LVMI, LAD and E-velocity were associated with improvement of cardiac symptoms. Furthermore, stepwise multivariate analysis found that IVS was an independent predictor (OR 0.451, 95% CI 0.209 to 0.976; p=0.043) of improvement of cardiac symptoms and eGFR yielded a trend (p=0.07) towards less improvement of cardiac symptoms. ROC curve analysis showed that an IVS cut-off of 11.9 mm was optimal in terms of sensitivity and specificity for predicting improvement of cardiac symptoms. According to the previous studies regarding cardiac morphology,29–31 ARAD affected the heart more adversely than essential hypertension, and hypertrophic responses differed between patients with and without ARAD. Losito et al reported that left ventricular hypertrophy was present more often in patients with ARAD than in those with essential hypertension (32.6% vs 10.8%, p=0.02).30 According to Wright et al, patients with ARAD have a higher prevalence of left ventricular hypertrophy (78.5% vs 46.0%, p<0.001) and higher LVMI (183±74 vs 116±33 g/m2, p<0.001) than controls.31 Of great interest, Vensel et al found that patients with ARAD had greater disproportionate hypertrophy of the IVS than those with essential hypertension.29 In the context of the cardiac geometric pattern in patients with ARAD, recent studies reported that eccentric hypertrophy was associated with renal dysfunction.32 33 Thus, greater IVS might imply a more advanced disorder-related ARAD in the heart and kidney and suggests less improvement of cardiac symptoms after renal revascularisation. The present finding that responders had less severe cardiac structural changes and better renal function indicates the clinical relevance of renal revascularisation at the early stage rather than the advanced stage, and therefore further studies are needed.
Some limitations of this study should be taken into consideration. First, our sample size was relatively small and the study was retrospective in nature. Second, the potentially disparate quality of echocardiographic evaluation might have varied among invited hospitals, depending on the machine used and on the skills of the sonographers. Third, in cases of ARAD patients with concomitant coronary artery disease, coronary revascularisation might have affected the outcomes. Finally, this study did not employ other metrics including renal duplex ultrasonography.
Conclusions
In this multicentre retrospective study, IVS was independently associated with improvement in cardiac symptoms after renal artery stenting although a large prospective study is needed to confirm the clinical significance of assessment of cardiac function in patients with ARAD.
Key messages
What is already known about this subject?
According to the most updated statement, cardiac disorders are categorised as appropriate clinical indications for renal revascularisation. Also, the response rate of renal artery stenting for cardiac disorders is in the range of 72.0–88.0%.
What does this study add?
This study reported the performance of echocardiographic indices for predicting cardiac benefits after renal artery stenting. An interventricular septal wall thickness cut-off of 11.9 mm provided the best predictive value, with a sensitivity of 71.4%, specificity of 75.5% and accuracy of 73.5%. The positive predictive value was 74.5% and the negative predictive value was 72.5%.
How might this impact on clinical practice?
This might increase awareness of the importance of cardiac function assessment in the management of atherosclerotic renal artery disease.
References
Footnotes
Contributors Each author has contributed significantly to the submitted work. Conception and design or analysis and interpretation of data, or both: YN, OK. Drafting of the manuscript or revising it critically for important intellectual content: YN, OK, SY. Data collection: YN, OK, AH, YY, KZ, HA, HD, SH, SI, TKa, TKu, YS, ST, YT, MU. Sample size determination: KN.
Competing interests None declared.
Patient consent Not needed because this study is a retrospective observational study.
Ethics approval National Cerebral and Cardiovascular Center.
Provenance and peer review Not commissioned; externally peer reviewed.