Article Text

Statistics from Altmetric.com
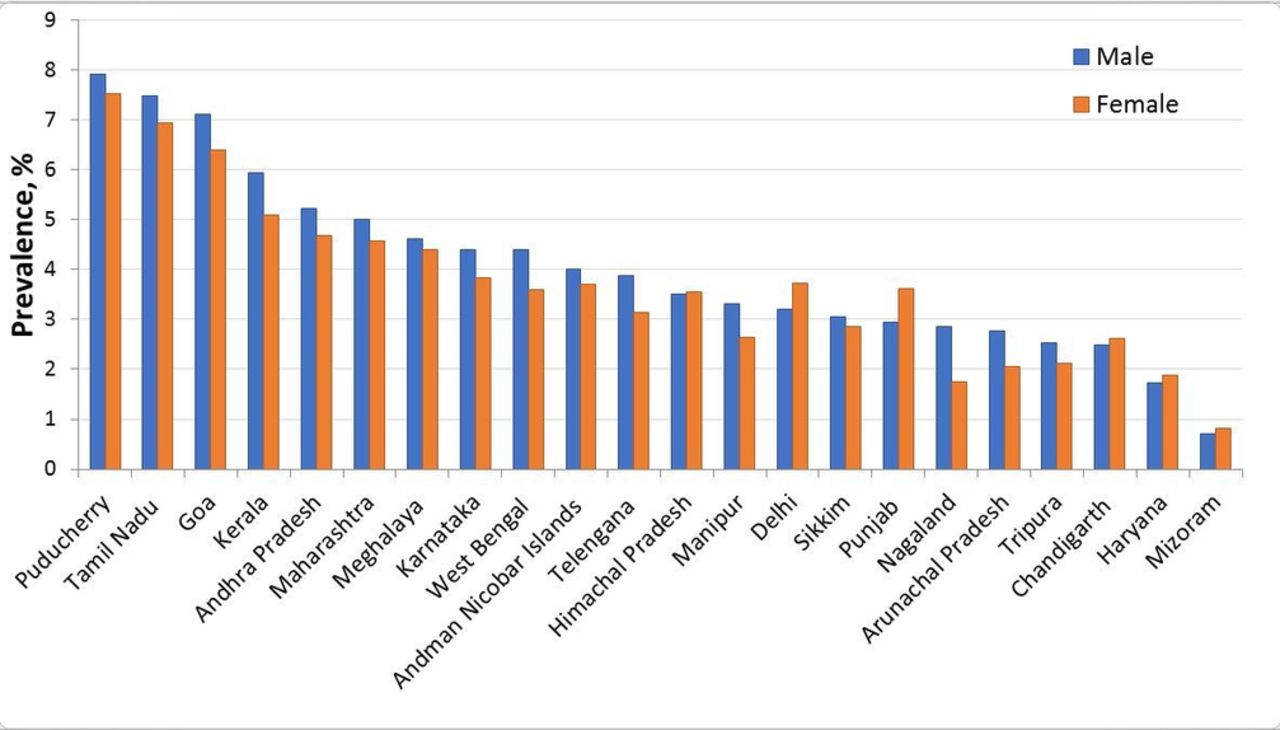
It is evident that cardiovascular disease (CVD) and its associated risk factors comprise a major and increasing burden of death and disability in India.1 In 2015, the Global Burden of Disease (GBD) study reported that ischaemic heart disease (IHD; the most common form of CVD) was the leading cause of premature mortality in India, after previously being ranked fifth a decade earlier.2 Over the decade from 2005 to 2015, premature IHD mortality increased by 11% compared with the next three leading causes: neonatal preterm birth, neonatal encephalopathy, and lower respiratory infection which, over the same period, each exhibited a greater than 30% reduction.2 This trend indicates clear changes in the burden of premature mortality away from communicable, maternal and neonatal conditions and towards CVD and other non-communicable diseases at an aggregate scale in India. Although CVD mortality may be the overall leading cause of death, summary statistics such as the GBD, while important, mask large variation in the distribution of CVD and risk factors along certain dimensions, for example, by region or state3 (figure 1) or socioeconomic status (SES),4 which have been identified by studies of the determinants and correlates among individuals.
{kind=link}
State level diabetes prevalence among men and women 18 years of age and older, 2012–2013. Authors’ calculation from the District Level Household and Facility Survey-4. Diabetes prevalence defined as fasting blood glucose 160 mg/dL or above, n=456 261.
Two papers in this issue of Heart Asia describe new data on trends and determinants of CVD, risk factors and treatment in diverse settings in rural Punjab and semiurban West Bengal.5 6 In the study by Goyal and colleagues, repeated surveys were conducted in the same rural Indian population in 1994 and 2014 focusing on coronary artery disease (CAD) and its risk factors.5 Among adults aged 30 years and older from three villages in Ludhiana district in Punjab, clinical measures of CAD, obesity, hypertension, diabetes, hypercholesterolaemia and smoking status were obtained. Over the 20-year study period, a statistically significant increase in CAD prevalence was observed (increasing from 2.8% to 4.1%) with corresponding increases in certain risk factors, although the CAD prevalence increase was not statistically significant among females. During the study period, some improvements in risk factors were noted. For instance, the prevalence of smoking and the use of desi ghee (a traditional cooking oil made from butter) decreased, although more respondents reported a sedentary lifestyle in the later survey and the decrease in the use of desi ghee was mirrored by a large increase in refined vegetable oils. A unique aspect of this survey was the repeated design that allowed investigators to determine annual percentage change in the prevalence of risk factors. This design also allowed for an examination of changes in the age and education structure of the population, which was found to be older and with a greater level of education in the later survey, either due to demographic shifts or differences in survey coverage.
The second study, by Khetan et al presents baseline data from an ongoing cluster randomised controlled trial of a community health worker model to improve the control of CVD risk factors in a community in West Bengal.6 The findings indicate that in this population with a mean age of 48 years about one-third (35%) had either hypertension, diabetes or was a current smoker.6 This study also explored risk factor associations with age, sex and SES defined by education and income. Participants with at least one risk factor were more likely to be male, older and of higher SES by wealth and education.6 Demographic and SES factors were also found to influence the control of CVD risk factors ; those with higher levels of education and income were around twice as likely to control their blood pressure and blood sugar. Females were also nearly three times as likely to report intent to quit smoking in the next 6 months, which was similar to rates of quitting found among women compared with men in a rural area of Andhra Pradesh.7
Socioeconomic gradients in CVD and risk factors
Our previous research identified empirically that, with the exception of smoking,8 CVD risk factors including obesity, diabetes, hypercholesterolaemia and hypertension show a marked gradient where the prevalence of risk factors and proportion of CVD mortality9 increase with corresponding increases in SES.4 SES gradients of similar magnitude and direction are found in the paper by Khetan and colleagues6 for CVD risk factors and control of these risk factors presumably through greater access to treatment and follow-up support among higher SES groups. Among the lowest SES group, 45% of participants had one or more CVD risk factors indicating a widespread prevalence of risk factors across the study population. Although Goyal and colleagues did not directly assess SES–risk factor associations, the increase in CVD risk factors over the study period is likely to be in part related to demographic changes in the community and improvements in the SES profile in the later survey. Many studies with SES–risk factor associations in India have been published since our original review, which has been updated as new evidence becomes available. The current database contains 114 studies and more than 900 SES–CVD and risk factor associations, covering over two times the number of studies and two and a half times the number of association as the initial review. A preliminary analysis of these data indicated that 80% of SES associations with diabetes and obesity were positive compared with 60% of associations between SES and hypertension and hypercholesterolaemia and roughly half of the SES–CVD associations. These findings indicate that although the SES gradients for risk factors are relatively stable, more studies have reported inverse gradients or null associations and the direction of association with CVD is less consistent. Although study quality was not assessed, the majority are cross-sectional and were limited to local or regional coverage and may not be representative of the whole of India.
Although determining the point at which social gradients in CVD and risk factors in India may ‘crossover’ to reflect the direction of SES associations observed in high-income countries remains an important epidemiological question, efforts need to be made to address the growing burden of CVD and risk factors across all segments of Indian society. To do so equitably, however, requires several considerations. First, resource allocation for prevention and treatment of CVD should be proportion to the burden within states or districts and by urban and rural areas. In many rural areas, the population continues to be faced with a substantial burden of communicable diseases and maternal–child under nutrition.10 Continuing efforts are required to ensure progress on improving the social circumstances and conditions in these areas while also promoting improvements in health behaviours such as smoking and poor diet that can improve the CVD risk factor profile. Second, there is an urgent need for national surveillance and monitoring of CVD and risk factors in India to appropriately prepare for any large shifts in the distribution of risk factors and disease. Khetan and colleagues present one possible model for such a surveillance system using community health workers for risk factor screening, education, follow-up and for reaching lower SES groups. Further research is needed on how to scale up such a model and whether integration is possible with existing national systems such as the Sample Registration System or Annual Health Survey. Large cross-sectional surveys such as the National Family Health Survey and District Level Health Survey are also extremely useful in quantifying the burden of disease but challenging to undertake and require commitment and resources to conduct repeat surveys at regular intervals. Finally, as the burden of CVD and risk factors increase, health systems need to develop appropriate mechanisms to ensure equal access to detection, treatment, including access to health workers and medications, and adequate control of CVD and risk factors across SES group. Data from Khetan et al 6 and elsewhere11 12 suggest that inequity in treatment and control of risk factors remains high in India. India has experienced tremendous economic growth in recent decades, but improvements have been remarkably uneven and concentrated among a small minority.13 There is a risk that healthcare resources could follow a similar trajectory amid the target of universal health coverage.
Footnotes
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.