Article Text

Abstract
Some of the highest recorded rheumatic heart disease (RHD) prevalence and mortality rates are from the World Health Organization’s Western Pacific Region (WPR). RHD burden has been well documented in much of the WPR subregion of Oceania, but less is known about RHD outside the Pacific Islands and Australasia. We aimed to review RHD burden in WPR outside Oceania to identify countries with high RHD burden and those with contemporary data gaps. We searched the peer-reviewed literature for English-language primary studies published between 1980 and April 2017 that reported RHD prevalence or mortality in the 13 WPR countries/areas outside Oceania, and Taiwan. We also searched for official government reports and health indicator documents. Results were synthesised narratively and reported stratified by 2015 Human Development Index (HDI) level. 30 peer-reviewed publications fulfilling inclusion criteria were identified, representing nine countries/areas. RHD prevalence and mortality have fallen in association with economic development, particularly in very high HDI countries. In several countries that have undergone recent economic development, RHD persists particularly among older populations. In poorer WPR countries there is a persistent RHD burden, including in young populations. Some countries had no available data. Although RHD burden has declined in many high-resource settings across the WPR, in several poorer countries, the impact of RHD appears to continue. Elsewhere, insufficient contemporary data make it difficult to gauge the current status of RHD burden and control. Concerted efforts are needed to fill information gaps and implement action to address this avoidable disease.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Rheumatic heart disease (RHD), an avoidable consequence of acute rheumatic fever (ARF), disproportionately affects the world’s most vulnerable people. It is estimated that there are approximately 33 million people living with RHD.1 In high-income countries, the burden of RHD decreased markedly during the 20th century, attributable to improved living conditions associated with socioeconomic development and advances in medical management. However, RHD continues to exact a considerable toll in many low-resource settings. The epidemiology of RHD largely parallels most indicators of poverty; there are profound disparities in disease burden globally, with prevalence increasing with increasing socioeconomic inequality.2
Some of the highest recorded RHD prevalence and mortality rates are from countries in the Western Pacific Region (WPR) of the World Health Organization (WHO). The WPR comprises an estimated 1.8 billion people, across 37 countries and areas.3 These culturally and developmentally diverse nations also exhibit marked variation in the size and capacity of their health systems, healthcare expenditures and health information infrastructures.4 5
RHD has been well documented in much of the WPR subregion of Oceania, which incorporates the 24 nations of the Pacific Islands and Australasia. Less is known about RHD in WPR nations outside Oceania. It is plausible that there are impoverished geographical areas where high RHD burden persists. Without sufficient data to inform a policy and programmatic response, RHD may be undetected, unreported and unmanaged at both the individual and population levels.
We aimed to review RHD burden in the WPR outside Oceania to identify countries with high RHD burden and those with contemporary data gaps.
Methods
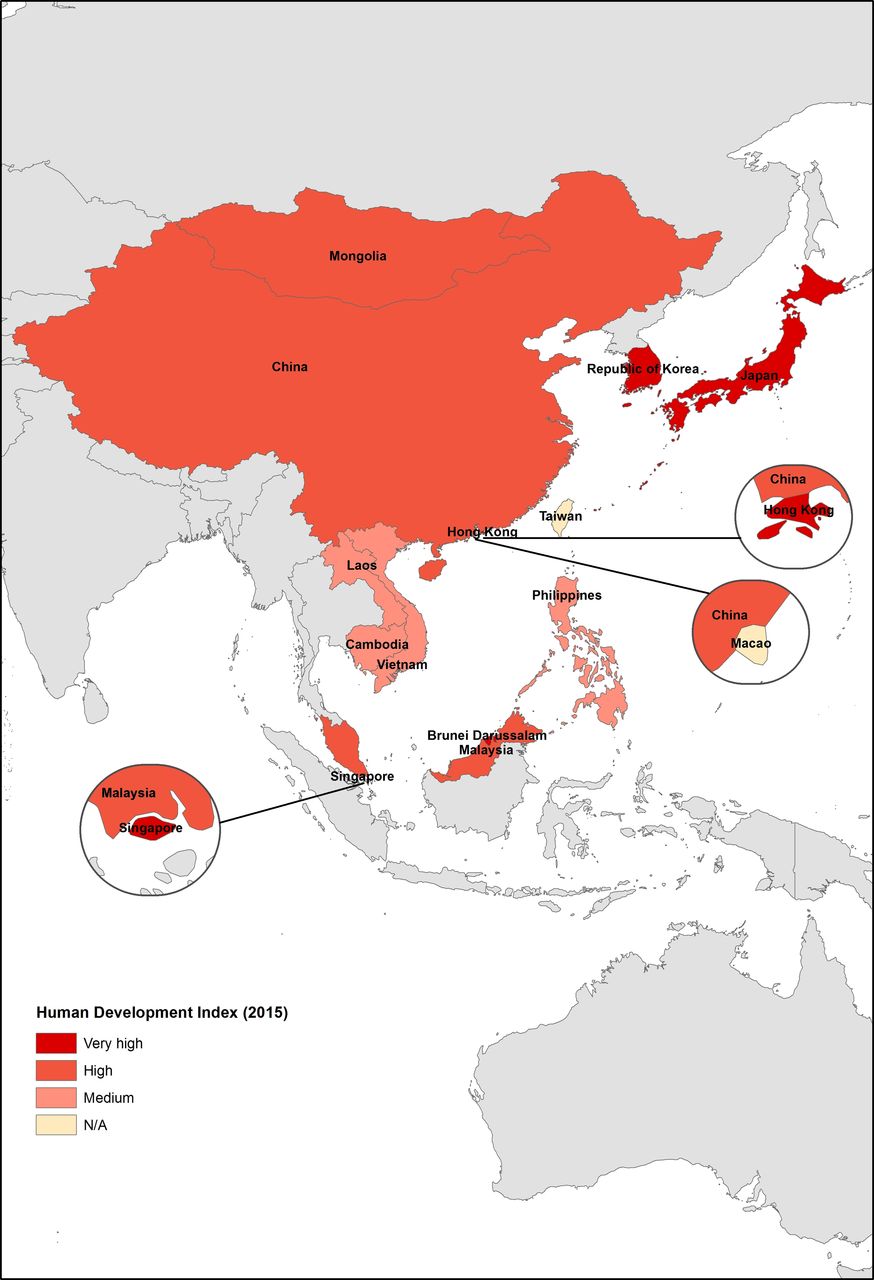
We identified publicly available official health statistics and peer-reviewed literature documenting RHD prevalence or mortality in the WHO WPR Member State countries/areas outside Oceania, as well as Taiwan (figure 1). Oceania was considered out of scope as a similar project has already been conducted for that subregion.6

Countries and areas of the Western Pacific region included within the scope of this study. Taiwan does not have WHO Member State status but is within this geographical region and so was included in this study.
We searched the PubMed and Global Health databases during April–June 2017 with a search strategy incorporating a combination of ‘rheumatic heart’ OR ‘rheumatic fever’ terms and individual country names. The rheumatic fever string was included to ensure all relevant papers were captured. Additionally, we searched the Institute for Health Metrics and Evaluation’s Global Health Data Exchange for RHD scientific literature, and relevant studies known to the authors were reviewed for eligibility.
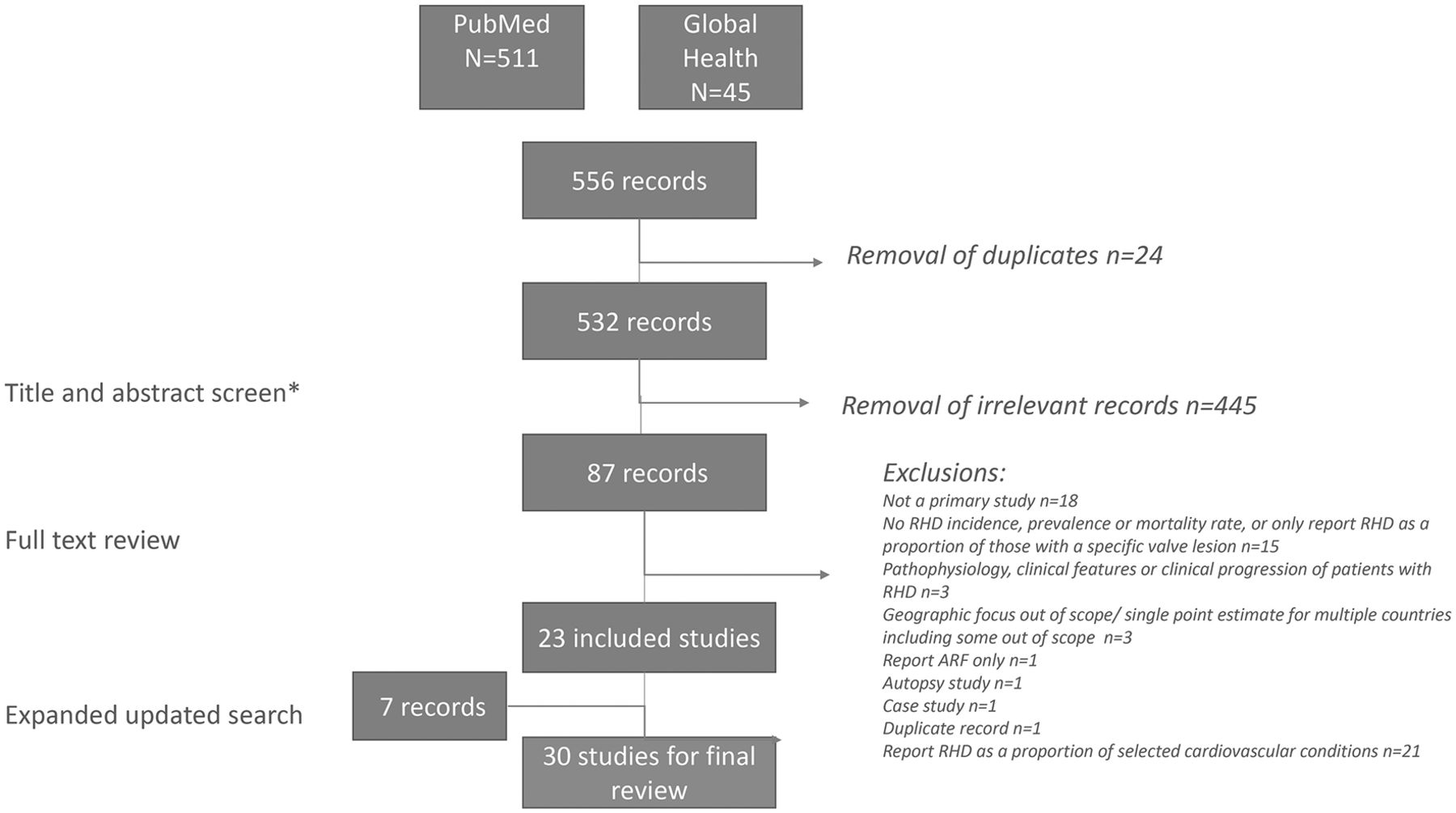
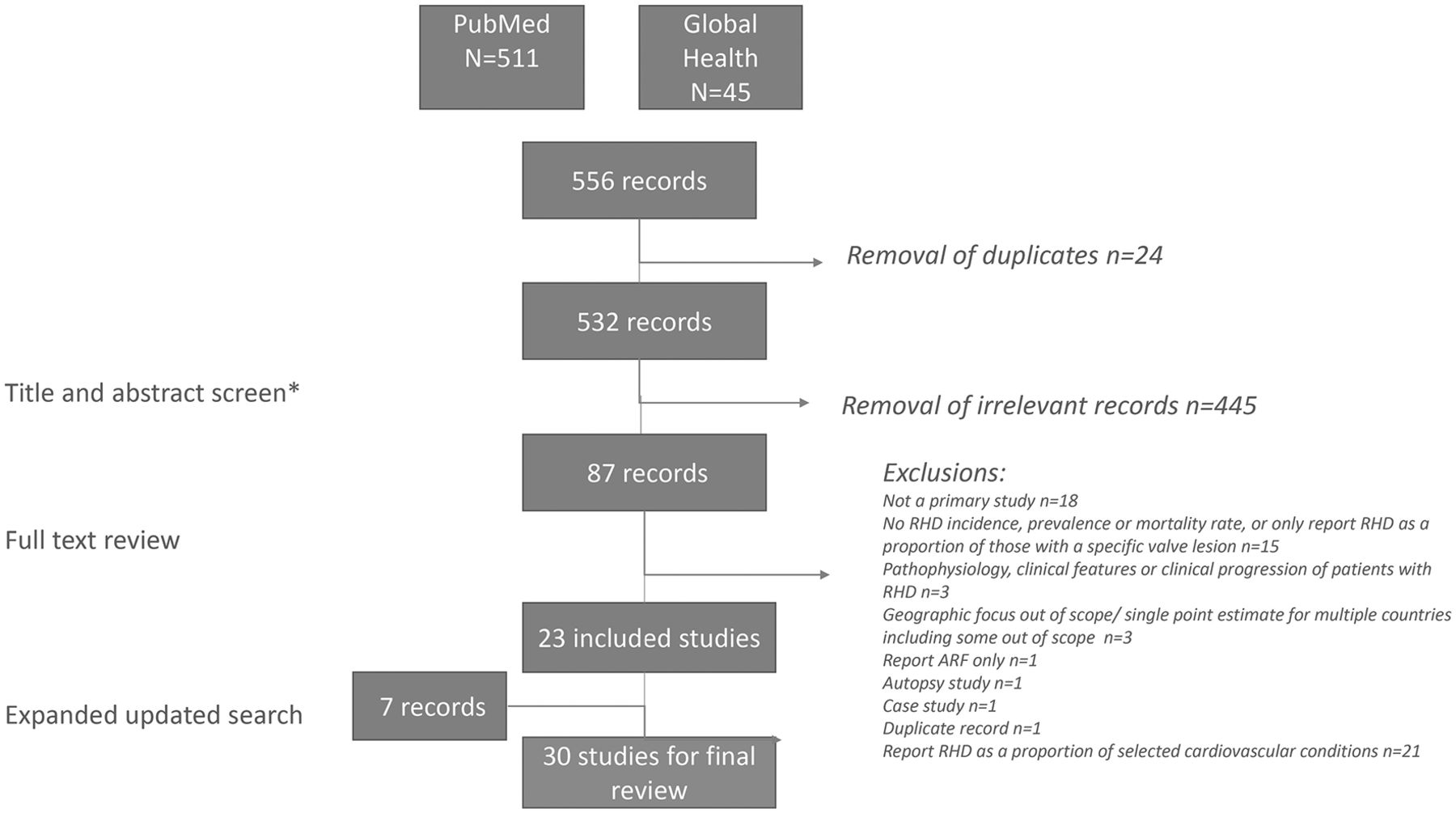
Studies were eligible for inclusion if they were primary studies conducted in the non-Oceania Member States and areas of the WHO’s WPR or in Taiwan; reported RHD prevalence or mortality rates or proportions for the general population or in specific population or clinical subgroups (obstetric, cardiovascular/echocardiograph populations, hospital admissions); were published between 1980 and April 2017 (regardless of study period); and full texts were available in English. We included studies that ascertained disease burden using any type of data source, including auscultation-based or echocardiography-based screening, administrative data or clinical records. Studies on RHD in pregnancy were included only if the total number of pregnant women was reported, allowing calculation of the proportion with RHD. Studies focusing solely on ARF were excluded. Other specific exclusions are outlined in figure 2.
{kind=link}
{kind=link}
Summary of literature search results. *Exclusion criteria: not a primary study (including guidelines, conference proceedings, reviews); case studies; published in a language other than English; focus is pharyngitis burden/rates of group A streptococcal colonisation; focus is pathophysiology/clinical features or clinical progression of patients with ARF/RHD; focus is outcomes or treatment effectiveness in patients with ARF/RHD; report proportion of patients with a specific valve lesion due to RHD but no population denominator; does not report RHD prevalence or mortality rates (including studies that only present absolute numbers); geographical focus out of scope or report single point estimate for multiple countries, including some out of scope. ARF, acute rheumatic fever; RHD, rheumatic heart disease.
We also conducted a Google search for national statistical agency health indicator and vital statistics documents reporting RHD prevalence or mortality and published in English. Where available, summary statistics were extracted from the most recent reports.
Title and abstract screening and full text reviews were undertaken by two reviewers independently, with disagreements resolved by consensus; records retrieved via the expanded search strategy and grey literature were assessed by one reviewer. Relevant data regarding study methods and disease estimates were extracted and summarised by one reviewer, with discussion as required. In papers reporting multiple components, only those measures fulfilling inclusion criteria were included (eg, absolute numbers only with no rates were not extracted). Where multiple estimates over a given period were presented, the earliest and the latest estimates were extracted and temporal trends noted.
Results are presented stratified by country level of development, with classification based on the United Nations Development Programme’s Human Development Index (HDI) for 2015.5 The HDI is a composite measure that reflects life expectancy, average and expected educational attainment and gross national income per capita, with a higher score reflecting better performance on these measures. This scheme classifies countries as having very high (HDI scores ≥0.800), high (0.700–0.799), medium (0.550–0.699) and low (<0.550) human development. Studies from China were also mapped against province-level HDI.7
Ethics approval was not required for the conduct of this study.
Results
Of 37 countries and areas in the WHO’s WPR, 11 countries and two Special Administrative Regions of China lie outside Oceania, as does Taiwan.
Figure 2 outlines the search strategy and handling of records. Full text review of 87 publications was undertaken, with 23 identified as relevant and a further 7 included following an updated search and review of papers known to the authors.8–37 Relevant RHD prevalence or mortality data were also retrieved from publicly available government documents for Brunei,38 Hong Kong,39 40 Japan,41 Mongolia42 and the Philippines43; no official statistics were identified for other countries/areas.
Table 1 summarises the peer-reviewed paper characteristics, representing 9 of the 14 countries/areas. Of these, 12 papers reported population-based prevalence, 13 reported RHD as a proportion of total admissions/surgeries/echos performed or proportion of deliveries, and 9 reported mortality rates. Several papers used multiple data sources and report multiple metrics. Study periods from Hong Kong, Singapore, Malaysia, the Philippines and Taiwan were all prior to 2000.
Study details for peer-reviewed publications presenting estimates of RHD burden by country/area 2015 HDI status, 1980–2017
Tables 2–5 present burden estimates from countries with very high, high, medium and unspecified 2015 HDIs, respectively, and table 6 presents official statistics.
RHD burden estimates in countries with very high 2015 human development indices, 1980–2017
RHD burden estimates in countries with high 2015 human development indices, 1980–2017
RHD burden estimates in countries with medium 2015 human development indices, 1980–2017
RHD burden estimates in countries and areas with 2015 human development indices unspecified, 1980–2017
National health agency RHD burden estimates, by country and year
RHD prevalence
Very high HDI: Singapore, Hong Kong, Japan, South Korea, Brunei
Two Korean papers covering 2006–2011 used administrative data to estimate prevalence, reporting high disease burden particularly among older age groups table 2.9 10 Two other prevalence papers were early studies of younger populations that reported low RHD prevalence among university students in Hong Kong in the 1970s12 and school children in Japan from the 1950s to 1980s.14
Early reports of disease burden among hospital populations in these settings also indicate a low prevalence. In South Korea in the mid-1980s, RHD comprised approximately 5% of adult cardiovascular admissions.8 In the 1960s–1980s, RHD decreased as a proportion of cardiac admissions in Japan14 and RHD as a proportion of hospital and cardiac admissions was also low and declining in Hong Kong among both adult and paediatric patient populations.12 13 Recent Hong Kong government reports indicate 1736 of 79 896 heart disease inpatient discharges or deaths in hospital in 2014 were due to RHD39 (2.2%).
Population-based or hospital-based prevalence estimates were not found for Brunei and Singapore, and the most recent data for Japan were from 1981 (prevalence in school children 0.14 per 1000).14
High HDI: China, Malaysia, Mongolia
Prevalence data were only available for China (table 3). Online supplementary figure S1 presents RHD data availability in China by province and by province HDI score. Provinces for which data were available were generally those with higher development levels; several impoverished provinces had no data. Burden estimates varied subnationally, by population subgroup, data source and over time. For example, in Dongguan City, 5 of 81 213 children aged 5–13 years screened in 2011–2012 had echo-confirmed RHD,21 equating to 0.06 per 1000. Among adults aged 18–74 years from nine communities in urban and suburban China, prevalence of echo-detected RHD was 1.86 per 1000 in 2001–2002.20 In a study involving 13 provinces, 91 of 29 079 subjects aged 30 and over, were reported to have RHD29 (3.13 per 1000). Earlier clinical screening data from Panyu County, Guangdong Province, demonstrated a prevalence of 2.5% in the general population aged over 15 years.19
Supplementary Material
Supplementary Figure 1:RHD data availability by province 2015 HDI score, China (footnote: some studies reported data from multiple provinces in a single point estimate)![[SP1.jpg]](https://heartasia.bmj.com/content/heartasia/9/2/e010948/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
The relative contribution of RHD to cardiovascular and general medical/paediatric admissions has generally decreased over time in China but still comprises a considerable caseload. For example, in Shanghai RHD accounted for 24.23% of all medical admissions with heart disease during 1980–1989,22 down to 2% of all cardiac admissions during 2000–2005.23 For one facility in Zhejiang over the period 2010–2015, RHD prevalence was 1.6% in adult patients.26 Similarly in 2008 RHD still comprised 20% of all cardiac surgery cases in Beijing.27 At a Shanghai facility, 0.5% of 20 983 women delivering during 1993–2007 had RHD.28 RHD also comprised 3% of all adult outpatient echocardiograms performed at a Shanghai facility in 201225 and 33% of all valvular disease among inpatients at a Guangdong centre in 2013.24
Mongolian official government documents report 24 116 new cases of ARF/RHD in 2012, and a total population of approximately 2.87 million,42 equating to 8.4 cases per 1000. No Malaysian data were identified.
Medium HDI: Vietnam, Philippines, Laos, Cambodia
No population or hospital prevalence data were available for Vietnam or Laos (table 4).
Estimates of echocardiography-confirmed RHD prevalence among school children based on screening studies ranged from 1 per 1000 in Legazpi City, Philippines in 199834 (screen by auscultation) to 21.5 per 1000 among children 6–17 years old in Cambodia in 2001–200231 (screen by echocardiography). RHD was the indication for 43% of all Cambodian cardiac surgery procedures between 2001 and 2006 and 29% between 2007 and 2011.32
HDI unspecified: Taiwan, Macao
No information was available specifically for Macao. Surveys (with examination in questionnaire-positives) in Taiwan show a significant decline in RHD prevalence in 1970–1985 from 1.4 to 0.62 per 1000 (table 5).36 ARF/RHD as a proportion of paediatric admissions fluctuated over the 1940s–1980s, to approximately 15 per 1000 admissions in 1981.37
RHD mortality
Mortality data in peer-reviewed literature were only available for six countries/areas.
The limited trend data available indicate that RHD as a proportion of total cardiovascular deaths generally decreased over time in countries across development levels, including in Malaysia30 and Japan.16 In Taiwan, age-adjusted RHD mortality rates decreased between the 1970s and 1980s35, and ARF/RHD mortality rates per million population also decreased between the 1950s and 1980s37. In the Philippines the crude annual death rate remained relatively unchanged in 1964–1976, although the absolute number of RHD deaths increased by more than 50%33; in Singapore RHD mortality increased from 3.6 to 4.4 per 100 000 between 1966 and 1977.17 RHD was the cause of an estimated 2.4% of heart disease deaths and 0.4% of total deaths in Japan during 1950–2008 collectively.15
Where available, contemporary RHD mortality estimates in very high development countries indicate a relatively low burden: 1.2 per 100 000 population in Hong Kong in 2014,40 1.8 per 100 000 population in Japan in 2014,41 1.4% of total cardiovascular deaths in Brunei in 201638 and combined ARF/RHD mortality of less than 1 per 100 000 population in Korea in 2012.11
Among high development settings, RHD mortality rates were not found for China. In Mongolia in 2012 there were 51 ARF/RHD deaths among 16 923 total deaths registered,42 equating to 3.0 ARF/RHD deaths per 1000. The most recent data from Malaysia were for 1989, when RHD comprised 1.7% of cardiovascular deaths and 0.5% of total deaths.30
From medium development settings, data were only available for the Philippines, where RHD mortality was 1.7 per 100 000 population among all ages in 2013.43
Discussion
The WPR outside Oceania is developmentally and demographically diverse, and it follows that there is marked variation in RHD epidemiology and data availability within and between countries. Findings of this review suggest that RHD prevalence and mortality have fallen in association with economic development, particularly in very high HDI countries. In several countries that have undergone recent economic development, RHD persists particularly among older populations, a legacy of high burden in the young before socioeconomic progress. In poorer WPR countries there is a persistent RHD burden, including in young populations. This review has also highlighted considerable data gaps, particularly pronounced in less developed countries such as Laos and Vietnam. Subnational data gaps also exist in some higher HDI settings that still have substantial populations living in poverty, whose RHD burden may therefore be masked. These findings have important implications for health policy and planning nationally, regionally and globally, and reinforce that urgent and concerted efforts are required to fill the data gaps and address this avoidable disease that still exists across the region.
Consistent with known patterns of RHD distribution in different age groups by levels of economic development, in some countries with very high current HDI, RHD burden is high among older populations. For example, in South Korea crude RHD prevalence for 2008 was estimated at 220 per 100 000, with highest prevalence rates being among people aged over 60 years (791 per 100 000), and total costs being US$67.25 million9. Besides economic repercussions, high disease burden in older populations also has marked implications for health service planning and delivery, particularly in the context of ageing populations. A high RHD burden may generate demand on health services, both for treatment of the valvular disease itself and for RHD sequelae (including endocarditis, ischaemic stroke and heart failure) and comorbidities.
The high disease burden in the young in low-resource settings is also cause for concern. Peak incidence of ARF occurs at ages 5–14 years and RHD prevalence increases with age, peaking at 25–34 years.44 The only relatively recent data from the four medium HDI countries was from Cambodia—prevalence among school children aged 6–17 years in 2001–2002 was 21.5 per 1000, with 90% being detected only on echocardiographic screen.31 Cambodia has a young population age structure, with approximately one-third of the total population aged 0–14 years.4 It is plausible that a similarly high burden of undetected disease exists in the other countries with similar levels of development and age structure.
In China, studies since 2000 indicate persistent burden among school children aged 5–13 years21 and the general population aged 30 and over29 and 18–74 years.20 Available Chinese data were predominantly from large cities; many less developed provinces had data gaps. Despite China’s considerable socioeconomic progress, pronounced socioeconomic inequality exists7 and RHD burden may well be higher in less developed, data-poor regions. Additionally, China’s large population size means that high rates translate into considerable absolute numbers of people living with RHD—prevalence of 2 per 1000 equates to an estimated 2 million middle-aged and elderly adults.20 RHD has generally decreased as a proportion of total medical and cardiac admissions over recent decades, likely reflecting China’s epidemiological transition with an associated increase in the burden of lifestyle-related conditions such as type 2 diabetes and ischaemic heart disease.
For several WPR countries, contemporary estimates of disease burden were not available in the peer-reviewed literature. In settings that now have very high HDI, this probably indicates RHD is no longer a public health priority. The prevalence study from Japan reported a progressively declining burden among school children over time, to 0.14 cases per 1000 in 1981.14 Similarly for Hong Kong, population prevalence among university students was low and the proportion of RHD hospital admissions progressively declined over the 1960s to 1980s.12 ,13 Although it is appropriate that resources are directed to areas of contemporary priority, there is no room for complacency, as highlighted by recent Japanese reports that between 2010 and 2015 there were 44 new cases of ARF occurring predominantly in large Japanese cities.45 In WPR and beyond, it is important that even highly developed nations remain vigilant to ARF and RHD.46
Data gaps elsewhere warrant attention because they occur particularly in settings where socioeconomic conditions would suggest that RHD burden is likely to be high. Several countries had high burden documented but no recent follow-up studies to gauge progress. In the Philippines, an early study documented a 13% increase in the ARF/RHD proportional mortality rate between 1964 and 1976,33 and a preliminary report on Filipino school screening (data to June 1998) indicated an RHD prevalence of 1 per 1000.34 More contemporary estimates were not found in the published literature. However, health department reports of mortality rates of 1.7 per 100 000 in 201343 indicate that RHD persists. A single Malaysian study reported cardiovascular mortality between 1950 and 1989,30 but no contemporary mortality statistics and no population-based estimates of RHD prevalence were located, as noted by others.47 Some developing countries had no data whatsoever. Globally, the volume of ARF/RHD research in the published literature has declined markedly over time, in parallel with and reflecting the decreased disease burden in developed nations, but this waning interest comes at the expense of information deficits in developing settings where disease burden is likely greatest.48
In some low-resource settings poorly developed health information infrastructure means that there are little real data about the health status of populations, including RHD burden. For example, mortality data are often unavailable because of inadequately functioning civil registration and vital statistics systems and poor rates of medical certification of cause of death.49 Data gaps mean that there is a reliance on statistically modelled estimates such as the Global Burden of Disease study50 to gauge disease burden.
Modelling studies help bridge information gaps. However, there are limitations, assumptions and uncertainties inherent in any model, and a model is only as good as its data inputs. For some WPR countries, modelled estimates differ considerably from other data sources. These estimates may not be directly comparable if the primary data signals are of poor quality or insufficiently described—paucity of information about diagnostic methods, case definitions, reporting requirements and other metadata may mean that modelled metrics and indicators derived from other data are not measuring the same thing, precluding direct comparison. For mortality estimates, differences may arise due to incomplete or poor quality death data requiring statistical correction for completion. In other cases, where local data are unavailable, modelled estimates are derived using data from other settings. Models are best enhanced by improving the primary data inputs. It is imperative that there is improved collection of real world data to more accurately understand the true situation on the ground.
There are several potential limitations to this work. Relevant papers may have been excluded or missed. Additionally, as this review only captured English-language peer-reviewed publications and government reports, burden estimates reported in other languages or sources were not considered. There are inherent difficulties in measuring RHD burden, including screening methodology and variation in the quality and completeness of civil registration systems and cause of death statistics across the region. Differences in study methodology, data sources, study periods, geographical coverage and study populations preclude direct comparison. In particular, the change from auscultation to echocardiographic screening (including World Heart Federation criteria for echo screening) is associated with significant changes in sensitivity.31 51 The metrics complied in this review encompass a range of indicators, methodologies and study population groups, and the measures reported differ both within some countries and between countries. This makes it difficult to accurately gauge progress over time, but this issue reflects the difficulties arising from not having standardised, consistent and serial measurement. Finally, settings with poor information infrastructure are also the ones most likely to have a considerable disease burden; hence, official statistics may not completely capture all cases/deaths.
Nonetheless, this paper tells the story of successes achieved in controlling RHD in some parts, where falling prevalence is followed by declining representation in biomedical literature. It also highlights information gaps and evidence of disease hot spots throughout the WPR beyond Oceania, indicating a need for active and ongoing disease control initiatives, and a focused regional effort to address this issue.
Elsewhere, high disease burden has precipitated strong calls to address this avoidable disease of disadvantage, including from across Africa52 and from the World Heart Federation, who have called for a 25% reduction in RHD mortality in those aged under 25 years by 2025.53 In the sustainable development goals era, the impetus to address poverty and the underlying social and systemic determinants of disease has never been greater. Achieving RHD control is now on the agenda at the highest levels of global health diplomacy.54 Concerted efforts across WPR are required to fill information gaps and ensure that targeted, contextually relevant actions are adopted where needed. Serial monitoring of disease burden is crucial to gauge progress and ensure that the whole region is on track to banishing RHD to the history books.
Acknowledgments
We wish to acknowledge Scott Sims of the Telethon Kids Institute, University of Western Australia, for his graphical work in producing the maps.
References
Footnotes
Contributors MA conceived and designed the study; undertook literature search, reviews and data extraction; synthesised and interpreted results; drafted manuscript. JK undertook literature search, reviews and data extraction; synthesised and interpreted results; edited manuscript. RW conceived and designed the study, interpreted results, edited manuscript. DW conceived and designed the study, interpreted results, edited manuscript. TDJ assisted with data collection, proofread manuscript. JC conceived and designed the study, interpreted results, edited manuscript and is the study guarantor.
Funding MA, RW, DW and TDJ are supported by the Medtronic Foundation grant to RhEACH. JK is supported by a National Heart Foundation Future Leader Fellowship.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This article has been corrected since it was published Online First. The sentence ’comprised 1.6% of all adult admissions.26' has been changed to read ’prevalence was 1.6% in adult patients.26'