Article Text

Abstract
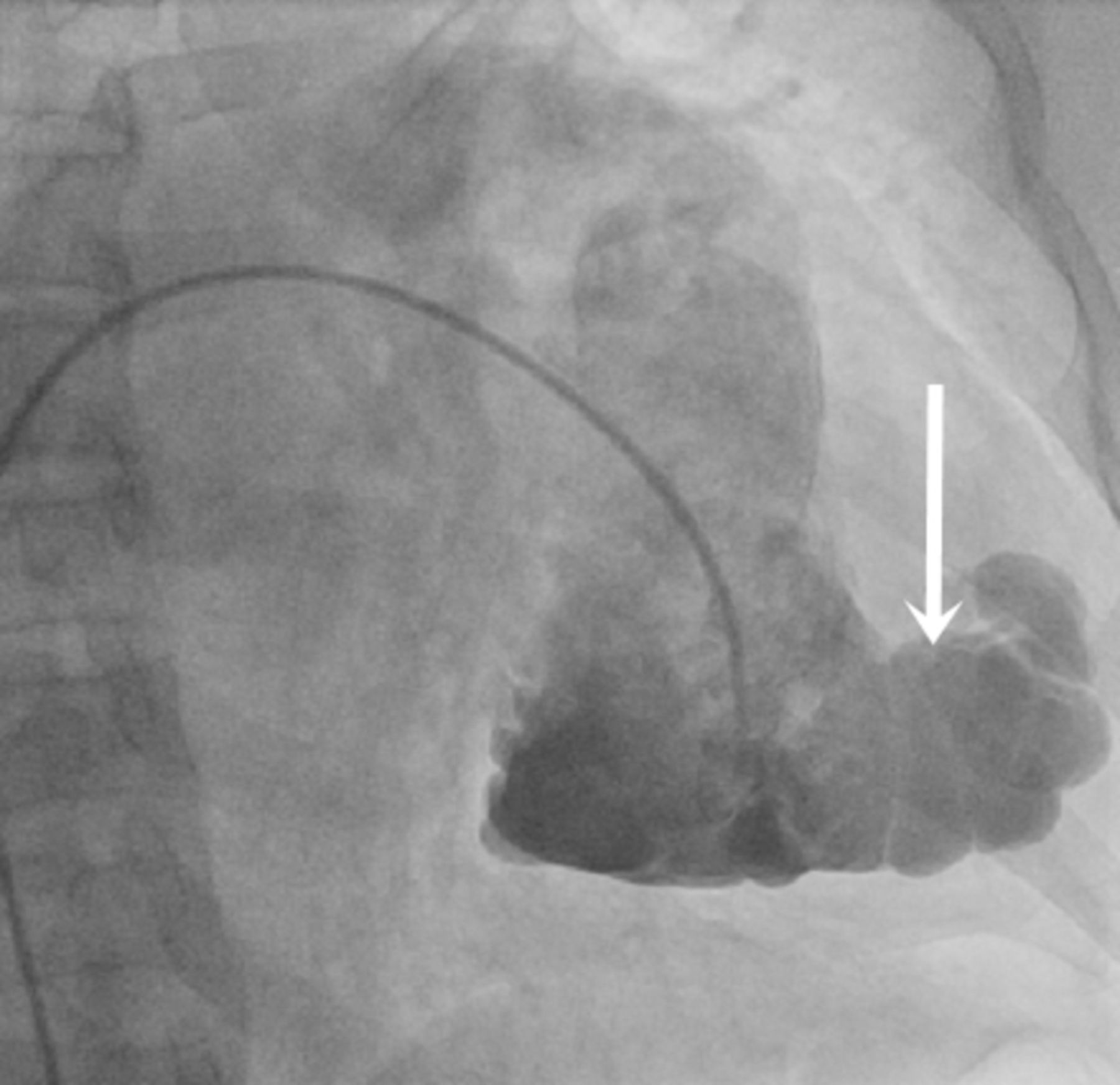
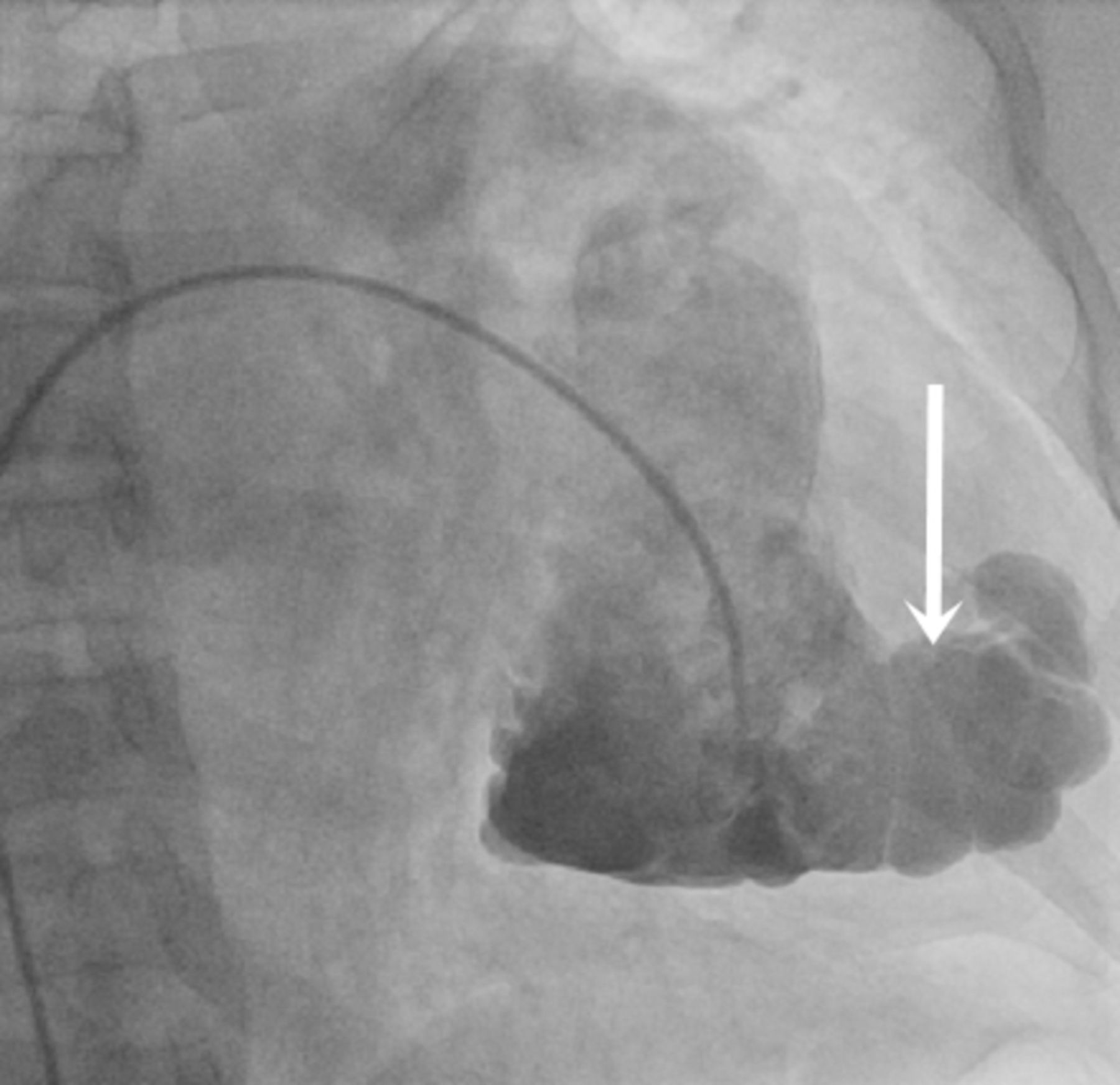
A 66-year-old man presented with abdominal distension and pedal oedema for the past 10 years. He had history of right heart failure on several occasions in the past, and one of these admissions prompted referral to a cardiac specialist. On examination, he had markedly elevated jugular venous pressure with prominent ‘y-descent’, a tricuspid regurgitation murmur, gross ascites and pedal oedema. A full blood count, routine biochemical screen and serum bicarbonate levels were normal. Right ventricular angiogram revealed a ‘caterpillar’-like aneurysm of the right ventricle (RV) apex (figure 1 arrow) with a dilated right ventricular outflow tract and significant tricuspid regurgitation with a dilated right atrium (see online supplementary video 1).
Supplementary file 3
{kind=link}
Acine angiographic frame of the right ventricle in posteroanterior view, showing a ‘caterpillar’-like right ventricle aneurysm (arrow).
Question On the basis of the clinical and right ventriculography features, what is the most likely diagnosis for this patient?
Arrhythmogenic right ventricular cardiomyopathy (ARVC)
Right ventricular endomyocardial fibrosis (RV-EMF) with an RV aneurysm
Cardiac sarcoidosis
Congenital diverticulum of the right ventricle
Question
- arrhythmogenic right ventricular dyplasia
- cardiomyopathy restrictive
- cardiomyopathy apical
Statistics from Altmetric.com
Answer: B
Chest radiography revealed significant right atrial (RA) enlargement (see online supplementary figure 1A, arrow). The echocardiogram showed a grossly dilated RA and a small RV with an apical aneurysm (see online supplementary figure 1B, arrow, and online supplementary video 2). Significant tricuspid regurgitation (see online supplementary video 3) and a restrictive filling pattern were noted. Cardiac catheterisation with pressure tracings showed a ‘dip-and-plateau’ appearance of the RV pressure tracing (see online supplementary figure 1C). Cardiac MR (CMR) imaging with a delayed enhanced phase of the myocardium (late gadolinium enhancement) showed high signal intensity in the right ventricular subendocardium (see online supplementary figure 1D).
Supplementary file 4
![[SP4.jpg]](https://heartasia.bmj.com/content/heartasia/9/2/e010957/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
Supplementary file 2
Significant RA dilatation, reduced RV volume, severe tricuspid regurgitation and restrictive pattern of RV pressure tracings (‘dip-and-plateau’ appearance or ‘square root sign, see online supplementary figure 1) indicate a diagnosis of RV-EMF. Subendocardial late gadolinium enhancement on CMR is diagnostic. Scarring or necrosis of the endomyocardium increases gadolinium concentration, which explains the delayed hyperenhancement.1
Supplementary file 1
An RV aneurysm with dilated right ventricular outflow tract mimics ARVC. But a dilated RV with transmural fatty replacement or diffuse thinning of the myocardium are the typical CMR features of ARVC. Hence option (A) is wrong. Advanced cases of cardiac sarcoidosis can have valvular abnormalities and ventricular aneurysms.2 However, zones of thinning with increased intramyocardial signal intensity are CMR features. Hence option (C) is also wrong. Narrow mouth and synchronous contractility are the characteristics of congenital diverticulum. They are usually associated with other congenital cardiac anomalies.3 But ventriculography of this case shows that the aneurysm balloons outward from a discrete region of the ventricular wall and is asynchronous to the adjacent myocardial segments, which is not a feature of congenital diverticulum. Hence option (D) is also not correct.
Fibrotic obliteration of the ventricular apex is the typical feature of EMF.4 But the formation of ventricular aneurysm is uncommon.5 Even though there is a significant decline in the number of newly diagnosed cases of EMF all over the world, it should be kept as a differential diagnosis of RV aneurysm, especially in tropical countries. The chronically raised pressure in the inflamed ventricle might have contributed to the development of the aneurysm. The patient was managed with diuretics and anticoagulation.
Footnotes
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.