Article Text

Abstract
Objective: To evaluate the incidence of coronary vasospasm as a possible pathophysiological mechanism causing chest pain symptoms in patients with clinically suspected myocarditis.
Design and setting: Prospective study in a teaching hospital.
Patients: 85 patients who presented at hospital with atypical chest pain and demonstrated clinical signs suggestive of myocarditis.
Main outcome measures: Incidence of coronary vasospasm demonstrated by intracoronary acetylcholine (ACh) testing.
Methods: The combined procedure of intracoronary ACh testing and endomyocardial biopsy (EMB) was performed after ruling out significant coronary artery disease (CAD). EMBs were analysed for myocardial inflammation by immunohistological methods and for virus genome persistence.
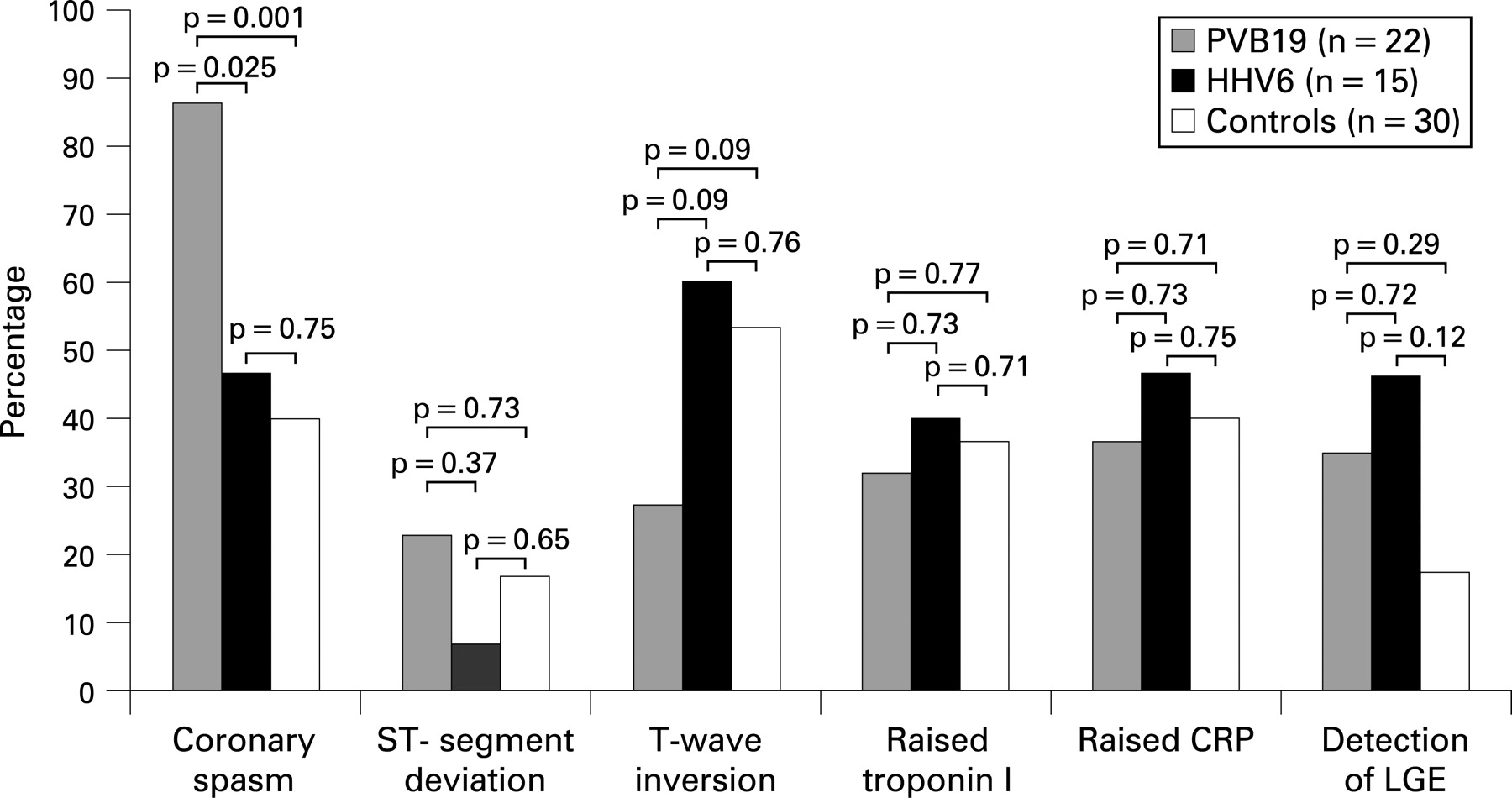
Results: Pathological biopsy results, including myocardial inflammation or detection of viral genomes, or both, were found in 55 (64.7%) patients while 30 (35.3%) patients showed neither cardiac inflammation nor viral genomes and were defined as the control group. Coronary vasospasm was demonstrated in 39/55 (70.9%) patients with pathological results compared with only 12/30 (40.0%) with normal biopsy results (p = 0.01). Patients with isolated PVB19 infection (n = 22) demonstrated a significantly higher incidence of coronary vasospasm than both those with isolated HHV6 infection (86.4% vs 46.7%; p = 0.025) and those with normal biopsy results (86.4% vs 40.0%; p<0.001). Univariate and multivariate logistic regression analysis showed that only PVB19 infection was independently correlated with coronary vasospasm (OR = 4.9, 95% CI 1.56 to 15.28, p = 0.006).
Conclusions: Coronary vasospasm is one of the main reasons for atypical chest pain in patients with clinical signs of myocarditis and biopsy-proven PVB19 myocarditis in the absence of significant CAD.
Statistics from Altmetric.com
In Western societies coronary artery disease (CAD) is the most likely diagnosis in patients presenting with typical or atypical chest pain syndromes.1 However, when significant CAD has been ruled out, other cardiac disorders such as myocarditis must be considered.2–4
Recent studies have shown that parvovirus B19 (PVB19) and human herpesvirus 6 (HHV6) are the most common pathogens of viral myocarditis5 and that the clinical presentation of patients with myocarditis is related to the type of virus present in the myocardium:3 Patients with myocardial PVB19 infection mainly presented with chest pain, whereas patients with myocardial HHV6 infection or combined PVB19/HHV6 infection showed symptoms of heart failure, suggesting a virus-specific pathophysiology that is currently unknown and may reflect a regional phenomenon.
It is known, however, that endothelial cells represent PVB19-specific targets in PVB19-associated myocarditis,6 7 probably through blood group P antigen.8 Thus, one may suspect a causal relationship between myocardial inflammation and/or PVB19 infection of vascular endothelial cells and microvascular dysfunction.9 10 In addition, myocardial inflammation in response to viral infection was found to be associated with increased endothelial expression of HLA and adhesion molecules, and to be correlated with systemic endothelial dysfunction.10 11 Furthermore, the presence of inflammation in both coronary arteries and myocardium with a proinflammatory shift in the myocardium has been associated with acute coronary thrombosis in patients dying after coronary thrombosis.12
Taken together, all these results suggest that symptoms of chest pain in patients with viral myocarditis, but no significant CAD, may be caused by coronary vasospasm, as a result of myocarditis-induced coronary endothelial dysfunction. This hypothesis would not only explain many previous findings but also offer new treatment strategies for chest pain symptoms in patients with myocarditis in the absence of CAD.
Consequently, we sought to evaluate whether chest pain in patients without CAD is caused by coronary vasospasm associated with myocarditis. Furthermore, we focused on possible differences between cardiac PVB19 and HHV6 infections, with respect to the incidence of coronary vasospasm.
PATIENTS AND METHODS
Patient population
Between June 2002 and September 2006 altogether 801 patients presented with atypical chest pain defined as a painful sensation starting immediately behind the sternum and occurring predominantly at rest (especially at night) without any physical exertion (in addition to other complaints). Patients demonstrating clinical signs suggestive of myocarditis were selected from the patients presenting with atypical chest pain (fig 1). Patients having a previous history of CAD or a cardiovascular risk profile clearly indicating CAD, severe heart failure (left ventricular ejection fraction <30%), other underlying cardiomyopathy, signs of renal failure or malignant diseases were not eligible for this study. Finally, 99 patients demonstrating clinical signs suggestive of myocarditis were recruited successfully.

Myocarditis was clinically suspected when at least one of the following criteria was present in combination with atypical chest pain: (a) history of malaise for more than 1 week and/or a history of respiratory and/or gastrointestinal symptoms, both within 8 weeks before admission; (b) ECG signs such as ST-wave abnormalities, T-wave inversions, new onset of conduction blocks, supraventricular tachycardia as well as sustained or non-sustained ventricular tachycardia. Fourteen of our 99 patients had to be excluded owing to current significant CAD (defined as coronary artery stenosis >50% in diameter) or significant CAD in the past, resulting in 85 patients available for analysis. Cardiovascular magnetic resonance imaging (CMR) was performed in 71 of the 85 patients. All patients gave written informed consent before inclusion in the study.
Acetylcholine testing and endomyocardial biopsy
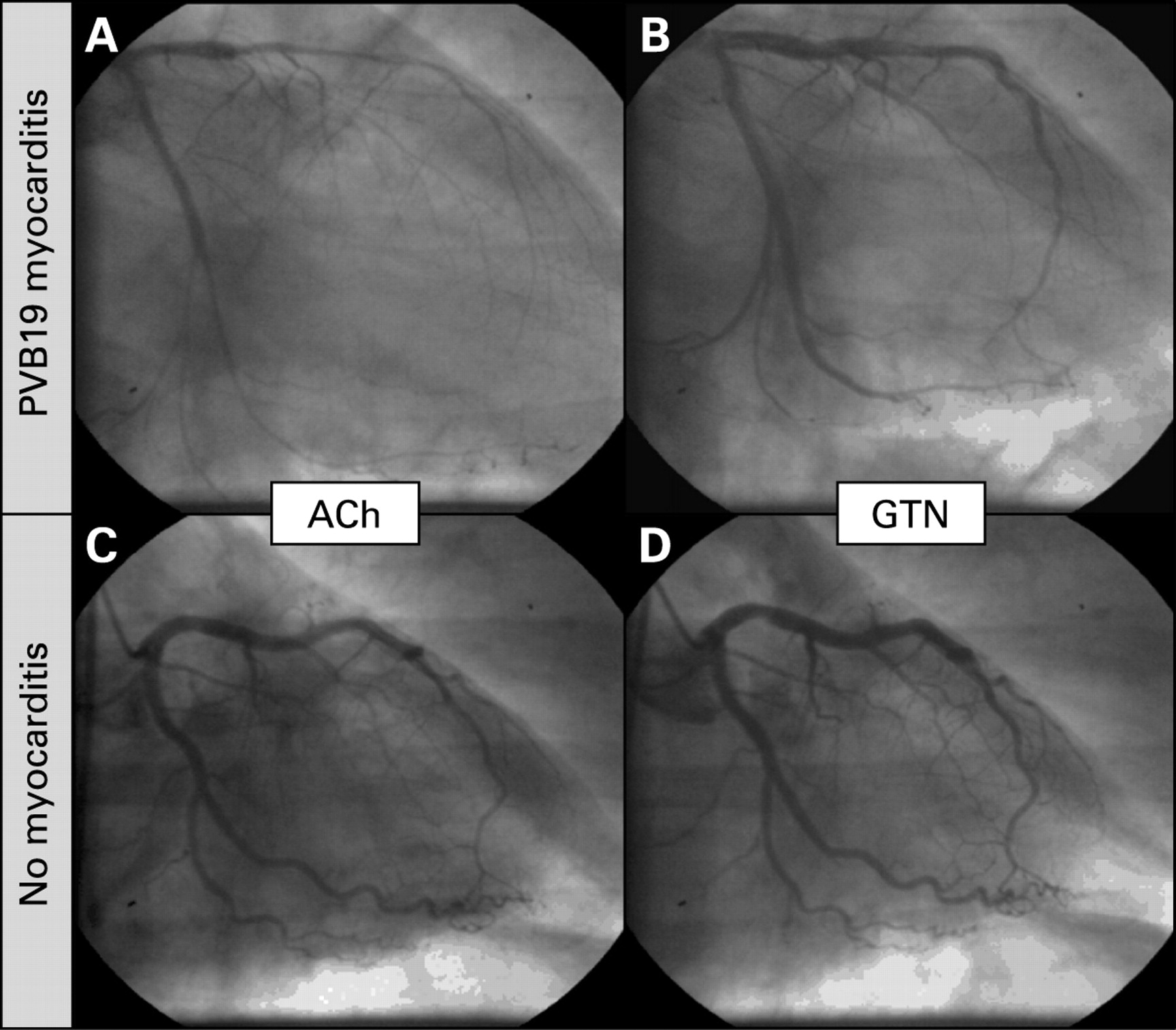
After stopping all vasoactive drugs for at least 24 h, diagnostic left ventriculography and multiplane coronary angiography were performed, followed by intracoronary acetylcholine (ACh) testing. Initially, all coronary arteries were selectively tested with graded doses of ACh, according to the protocol of the ENCORE investigators.13 However, in view of the Japanese experience14 we decided to adapt a more simple, yet equally effective, protocol in 2005: After baseline angiography, the left coronary artery was tested in a projection best showing large portions of the vessel. Graded doses of ACh (2 μg, 20 μg and 108 μg) were given over 3 min each, using the catheter employed for diagnostic coronary angiography. The test was stopped if symptoms occurred and coronary vasospasm was seen in at least one of the tested major coronary arteries (left anterior descending or left circumflex artery). Glyceryl trinitrate was applied immediately, dependent on the patient’s symptoms. If no vasospasm was detected in the left anterior descending or left circumflex artery, the catheter was repositioned in the right coronary artery and just a single dose of ACh (80 μg) was applied. Finally, glyceryl trinitrate (0.2 mg) was injected into both the left and right coronary arteries and additional coronary angiograms were obtained. The proportion of positive test results was identical for both ACh testing protocols used.
To evaluate myocardial inflammation and infection, endomyocardial biopsy specimens (EMBs) were taken from the right (septum) or left ventricle (free wall), or both, under fluoroscopic control after the coronary spasm provocation test.15 16
Histopathological analysis
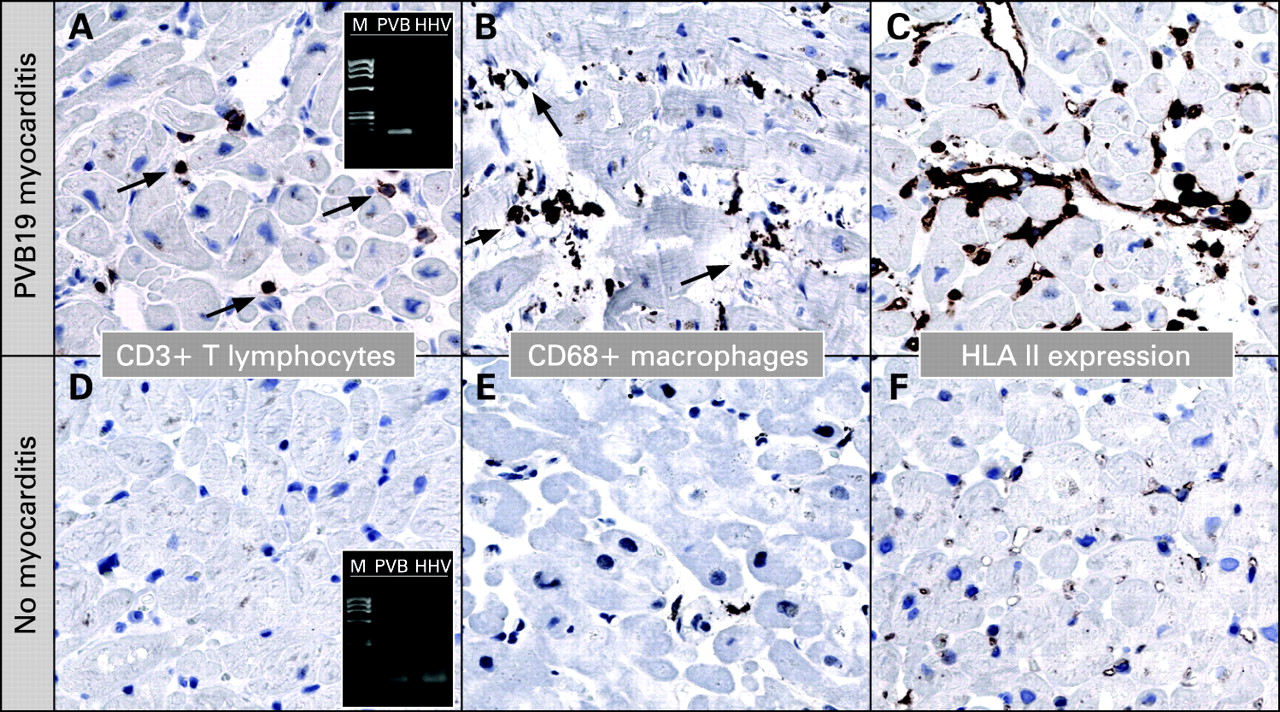
EMBs were stained with Masson’s trichrome as well as Giemsa stain and examined by light microscopy. For immunohistology, tissue sections were treated with an avidin–biotin immunoperoxidase method (Vectastain-Elite ABC Kit; Vector, Burlingame, California, USA), with application of the following monoclonal antibodies: CD3 (T cells; Novocastra Laboratories, Newcastle, UK), CD68 (macrophages, natural killer cells; DAKO, Hamburg, Germany) and HLA-DRα (DAKO).
Myocardial inflammation indicative of myocarditis was defined as the detection of ⩾14 infiltrating leucocytes/mm2 (CD3+ T lymphocytes or CD68+ macrophages, or both).17 Active myocarditis was diagnosed when myocardial inflammation was combined with the presence of myocyte damage.18–20 In addition, expression of HLA class II molecules in professional antigen-presenting immune cells and endothelium was visually assessed after immunoperoxidase staining.7
Detection of viral genomes
DNA and RNA were extracted simultaneously with the use of proteinase-K digestion followed by extraction with phenol/chloroform. Nested polymerase chain reaction (PCR)/reverse transcriptase-PCR was performed for the detection of enteroviruses (including coxsackieviruses of group B, various coxsackieviruses of group A and echoviruses), PVB19, adenoviruses, human cytomegalovirus, Epstein–Barr virus and HHV6. As a control for successful extraction of DNA and RNA, oligonucleotide sequences were chosen from the glyceraldehyde-3-phosphate dehydrogenase gene. Specificity of all viral amplification products was confirmed by automatic DNA sequencing.3
Angiographic analysis
Coronary angiograms were analysed by a blinded observer using quantitative coronary angiography (QCA) software (QCA-CMS 6.0; Medis, Netherlands), applying an automatic edge detection algorithm, according to the segment classification model of the American Heart Association. Only main segments of the main coronary arteries were included in the analysis. Average lumen diameters were determined in identical, at least 10 mm long segments in the angiograms, first after ACH infusion and then after glyceryl trinitrate application. The percentage vasoconstriction was determined by dividing the mean segment diameter after ACh by the diameter after glyceryl trinitrate application and subtracting the result from 1.21
Patients with significant CAD, defined as coronary artery stenosis >50% in diameter in at least one coronary artery segment, were excluded. Coronary vasospasm was defined as a lumen narrowing of a coronary artery segment >75% in diameter after ACh infusion as compared with the relaxed state after intracoronary application of glyceryl trinitrate, associated with ischaemic ST-segment changes or reproduction of the identical clinical symptoms that led to hospital admission.22 A negative result was noted if there was no severe lumen narrowing in all tested coronary arteries, as described above, and no or only minor, non-significant ST-segment changes occurred. The feeling of a hitherto unknown chest pain symptom in the absence of severe vasoconstriction and without significant ST-segment changes was seen in a few patients and consequently interpreted as an unspecific sensation in response to ACh.
Cardiac magnetic resonance protocol and analysis
ECG-gated CMR imaging was performed in breath-hold with the use of a 1.5 T Magnetom Sonata (Siemens Medical Solutions, Erlangen, Germany). Both cine and late gadolinium enhancement (LGE), short-axis CMR images were prescribed every 10 mm (slice thickness 6 mm) from base to apex. In-plane resolution was typically 1.2×1.8 mm. Cine CMR was performed with the use of a steady-state free precession sequence. LGE images were acquired on average 5–10 min after contrast administration with the use of a segmented inversion recovery gradient echo technique23 and constant adjustment of inversion time. The contrast dose (Omniscan (gadodiamide); Amersham Health Deutschland, Braunschweig, Germany) was 0.1 mmol/kg. Contrast images were evaluated for LGE after dividing each short axis into 12 circumferential segments. The presence or absence of LGE was assessed visually by reaching a consensus between two experienced observers.
Statistical analysis
Data for continuous variables are expressed as mean value (SD), whereas data for categorical variables are expressed as the number and percentage of patients. Comparisons between groups were done using a two-sided unpaired Student t test for normally distributed variables and a Mann–Whitney U test for non-normally distributed continuous variables. For categorical variables we used the χ2 test and Fisher exact test, where appropriate. For multiple group comparisons post hoc testing was performed using Bonferroni correction. Univariate and multivariate logistic regression analyses were performed in order to identify possible determinants of coronary vasospasm. Only univariate variables with a p<0.30 were entered into the multivariate logistic regression analysis. The difference between two groups was defined as significant if the two-sided p value was <0.05.
RESULTS
Clinical presentation
Table 1 shows the patients’ clinical characteristics. Pathological EMB results including myocardial inflammation or detection of viral genomes, or both, were present in most patients, while only a minority had neither myocarditis nor detection of viral genomes. This biopsy-negative subgroup constituted the control group in this study. Apart from coronary vasospasm in some of these controls, no definitive reason for their complaints could be found. No significant differences in cardiovascular risk profiles were detected between the groups.
Histopathological analysis and detection of viral genomes
In our 55 patients with pathological EMB results (figs 2A–C), myocardial inflammation was detected in 47 and viral genome persistence in 42 subjects. Histopathological and immunohistological investigation showed active myocarditis in seven patients and viral genome persistence without inflammation in eight. PVB19 genomes were detected by nested PCR in 22 patients, with 18 of them having myocardial inflammation, including two patients with active myocarditis. HHV6 genomes were found in 15 patients, with 12 of them having myocardial inflammation, including two patients with active myocarditis. A combined infection with PVB19 and HHV6 was demonstrated in five patients (four of them with myocardial inflammation and one patient with virus persistence only). No other viral genomes were detected in our patient group. In 13 patients myocardial inflammation was found without detection of viral genomes (including three patients with active myocarditis). The remaining 30 patients did not show myocardial inflammation and showed no viral genomes in the heart (figs 2D–F).

Intracoronary ACh testing
Coronary vasospasm was demonstrated in 39/55 (70.9%) patients with pathological EMB results, whereas it was only seen in 12/30 (40.0%) patients with normal EMB results (p = 0.01). In this group of 39 patients with pathological results in EMBs and coronary vasospasm, the mean (SD) value of maximal vasoconstriction (response to ACh compared with the relaxed status after glyceryl trinitrate application) was 90.3 (9.3)%, compared with 22.7 (9.0)% in the 16 patients with pathological EMB results but without coronary vasospasm (fig 3). In our control group with normal EMB results and coronary vasospasm, the averaged maximal vasoconstriction was 91.9 (7.1)%, compared with 22.7 (12.1)% in patients with normal EMB results and no coronary vasospasm.
To elucidate possible clinical differences between patients with isolated PVB19 infection, isolated HHV6 infection and those without histopathological abnormal results, pairwise comparisons were performed (fig 4). Patients with isolated PVB19 infection demonstrated a significantly higher incidence of coronary vasospasm, compared with those with isolated HHV6 infection and to those with normal biopsy results. The remaining variables, including ST-segment changes, T-wave inversions, raised troponin I and raised C-reactive protein serum level at admission did not differ significantly between the groups.

CMR results
CMR analysis for investigation of clinically suspected myocarditis was performed in 71 patients, while the remaining 14 patients did not undergo CMR owing to contraindications (n = 4), severe claustrophobia (n = 5) or logistic difficulties (n = 5). LGE was detected more commonly in patients with PVB19 myocarditis or HHV6 myocarditis (35.0%, n = 7 and 46.2%, n = 6), respectively), or in patients with myocardial inflammation in the absence of virus persistence (30.8%, n = 4), than in those with normal biopsy results (17.4%, n = 4; p = 0.05). The small numbers of patients in the various subgroups precluded a meaningful further statistical analysis between these subgroups.
Interestingly, in the 13 patients who had either PVB19 myocarditis or HHV6 myocarditis as well as myocardial LGE, coronary vasospasm was present in nearly all of them (84.6%, n = 11). In contrast, only 50.0% (n = 24) of patients with pathological biopsy results and no LGE demonstrated coronary vasospasm (p = 0.03). Compared with those with either PVB19 myocarditis or HHV6 myocarditis as well as myocardial LGE, only 21.7% (n = 5) of the patients with normal biopsy results and no LGE had coronary vasospasm (p<0.001). Thus, the highest incidence of coronary vasospasm was found in patients with biopsy-proven myocarditis in combination with LGE.
The distribution patterns of LGE in this small cohort of patients with PVB19 and HHV6 myocarditis was as follows: LGE in the lateral free wall was detected in four patients with PVB19 compared with in two patients with HHV6. LGE in the septal wall was detected in three patients with PVB19 and four with HHV6. Importantly, in four of those 13 patients, LGE was not distributed subepicardially or intramurally as would be typical for myocarditis, but subendocardially or transmurally, similar to myocardial infarction (fig 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Logistic regression analysis
Univariate and multivariate logistic regression analyses were performed to identify possible determinants of coronary vasospasm. Univariate linear regression analysis showed that only isolated PVB19 infection detected by PCR analysis was a significant determinant of coronary vasospasm documented by intracoronary ACh testing, whereas isolated HHV6 infection was not associated with coronary vasospasm (table 2).
Higher age and female gender tended to be associated with a higher incidence of coronary vasospasm, but these measures did not reach statistical significance. When variables with p<0.30 in univariate regression analysis were entered into the multivariate logistic model (table 3) only PVB19 infection was correlated with coronary vasospasm independently of other variables.
DISCUSSION
We could demonstrate for the first time that coronary vasospasm is more common in patients with pathological EMB results than in those with normal EMB results. Furthermore, patients with isolated PVB19 infection were found to have a significantly higher incidence of coronary vasospasm than those with isolated HHV6 infection and those with normal biopsy results. Interestingly, only PVB19 infection was found to be independently correlated with coronary vasospasm. Hence, these results expand our knowledge of clinical and pathophysiological differences based on different viral pathogens.
Prevalence of biopsy-proven myocarditis and coronary vasospasm in patients with clinically suspected myocarditis
We enrolled 85 patients into this study in whom myocarditis was suspected by a history of malaise/viral illness or abnormal ECG findings together with atypical chest pain as the main symptom forcing the patients to seek medical attention. In agreement with the WHO/ISFC Task Force Report the final patient classification in this study was based on biopsy results and not on clinical symptoms.24 These clinical criteria were considerably less strict than those used in our previous studies.3 25 Consequently, the average severity of disease in this study group was less pronounced and myocardial inflammation and/or virus persistence was diagnosed with the use of histopathological, immunohistological and PCR techniques in 55 patients only.
In accordance with appropriate guidelines,1 intracoronary ACh testing as the “gold standard” for the diagnosis of coronary vasospasm was performed after CAD was ruled out. Previously, only Kuhl et al had performed intracoronary ergonovine testing in a subset of nine patients with biopsy-proven myocarditis.9 The incidence of coronary vasospasm was significantly higher in our patients who had pathological biopsy findings than in the controls (70.9% vs 40.0%, p = 0.01). Thus, this study demonstrates for the first time a clear relationship between myocardial inflammation and/or virus presence and coronary vasospasm as the reason for atypical chest pain in a larger group.
Nevertheless, the incidence of coronary vasospasm in our control group (40.0%) was comparatively high. The reason for this observation may be an erroneous assignment of some patients to the groups owing to a possible sampling error in EMBs. Interestingly, a closer look at some of these controls shows the limitation of classification of patients based on biopsy results. The clinical characteristics of the four patients in the control group (history of malaise/viral infection together with ECG changes on admission and raised markers of inflammation or myocardial damage) who had LGE by CMR were indicative of myocarditis. Accordingly, all four patients demonstrated coronary vasospasm by ACh testing. However, EMB results in those patients did not show signs of myocarditis and these patients were hence assigned to the control group. Therefore, we speculate that the true incidence of coronary vasospasm might be even higher in patients with biopsy-proven myocarditis and even lower in patients without myocarditis. Interestingly, in a comparable study the prevalence of coronary spasm was found to be 41% in patients with suspected myocardial ischaemia and without significant CAD.4 This is in accordance with the incidence in our control group and obviously lower than in our myocarditis group.
Incidence of coronary vasospasm and differences between viral pathogens
In our previous studies we have shown that the clinical presentation of human myocarditis is related to the underlying viral pathogen.3 Other studies support the clinical observation that PVB19 infection may mimic acute myocardial infarction.9 26 Therefore, we hypothesised that PVB19 would be the most important viral pathogen causing coronary vasospasm in patients with biopsy-proven myocarditis.
To verify this hypothesis, first we performed pairwise comparisons of viral pathogen-based groups that demonstrated a significantly increased proportion of results positive for coronary spasm in PVB19-positive patients compared with HHV6-positive patients or patients with normal EMB results. Subsequently, we applied logistic regression analysis to assess possible determinants of coronary vasospasm and could demonstrate that PVB19 infection was the only significant variable associated with coronary vasospasm in our study group, verifying our hypothesis.
Possible mechanism for myocarditis-associated coronary vasospasm
The current results in combination with those of previous studies may improve our understanding of the complex pathophysiology in human myocarditis. It has been shown that peripheral and coronary endothelial function is impaired in patients with myocardial virus persistence and this impairment is even more pronounced in the case of both myocardial virus persistence and inflammation.10 11 27 However, although systemic endothelial dysfunction may be associated with exercise intolerance and a worse prognosis,28 it does not explain the clinical symptom of resting chest pain in subjects with myocarditis. With this study, we were able to demonstrate that coronary vasospasm is responsible for chest pain symptoms in patients with myocarditis apart from other possible reasons. Hence, myocardial inflammation or virus persistence, or both, may cause a coronary vasomotility disorder enabling the occurrence of coronary vasospasm.
This coronary vasomotility disorder may be caused by severe endothelial dysfunction due to a decreased bioavailability of the vasodilator nitric oxide (NO), as this pathophysiology has previously been suggested as a possible mechanism for coronary vasospasm.29 Interestingly, other researchers have shown that systemic inflammation (induced by vaccination) may cause endothelial dysfunction through reduction of vascular NO bioavailability and increases in oxidative stress.30 31 However, this hypothesis of endothelial dysfunction is competing with the view of a coronary smooth muscle cell hyper-reactivity as the underlying cause for coronary vasospasm.32 In previous studies, an increased intracellular rho-kinase activity was identified as a possible key mechanism for smooth muscle cell hyper-reactivity.33 This kinase was found to be highly activated only in spastic coronary arteries, while non-spastic coronaries (even within the same person) did not demonstrate increased rho-kinase activity.33 Furthermore, there is evidence that the activation of this kinase may facilitate leucocyte adhesion to arteries, thereby enabling their accumulation in the vessel wall and the spread of inflammation.34 Therefore, one might also speculate that viral infection of coronary arteries may be associated with coronary smooth muscle cell hyper-reactivity, thereby facilitating the expansion of inflammation and the occurrence of coronary vasospasm. However, it is currently unknown whether rho-kinase activity is increased in inflamed myocardium.
Bültmann et al described an increased expression of the adhesion molecule E-selectin in PVB19-targeted endothelial cells,6 which in turn should facilitate the adhesion and migration of leucocytes from the intravascular bed into the myocardial interstitium. Depending on the severity of virus infection and the individual immune response, a further spread of the inflammation to other myocardial regions and layers with the accumulation of interstitial lymphocytes and macrophages can be expected, causing various patterns of myocardial damage. In this context, increased HLA class II expression reflecting professional antigen-presenting immune cells was seen in the cardiac interstitium surrounding small-sized vessels in some of our patients. Hence, the infection of coronary endothelial cells with PVB19 may cause a kind of “coronary vasculitis” which may constitute a major determinant of the future clinical course and the myocardial spread of the inflammation.
The incidence of coronary vasospasm was significantly lower in patients with HHV6 infection than in those with PVB19 infection, and regression analysis showed no association between HHV6 infection and coronary vasospasm. However, almost every second patient with isolated HHV6 infection demonstrated coronary vasospasm. The reason for this observation is not quite clear. Unspecific myocardial inflammation12 31 caused by HHV6 infection may have resulted in a coronary vasomotility disorder enabling the occurrence of coronary vasospasm. However, there is some evidence that HHV6 can also lead to vascular injury.35 HHV6 seems to be able to directly infect various human endothelial cells, including the endothelium of human microvessels,36 and even replicate in certain endothelial cells.37 Therefore, we cannot rule out the possibility of an HHV6-specific effect on human coronary arteries also resulting in some kind of increased coronary reactivity.
Various LGE patterns in patients with myocarditis and coronary vasospasm
We have demonstrated previously that the pattern of myocardial damage induced by viral infection as detected with LGE differs depending on the underlying pathogen: in the case of PVB19 infection myocardial damage was predominantly seen in the subepicardium of the lateral free wall.3 This subepicardial pattern was also shown in this study in some patients with PVB19 myocarditis (figs 5A and B). However, a severe coronary vasospasm induced by PVB19 infection, mimicking acute myocardial infarction as suggested above, should rather cause myocardial damage in the subendocardium than epicardium. How can this discrepancy be explained? As mentioned before, the average disease severity in this study group was less pronounced than in our previous studies owing to different inclusion criteria. Consequently, in patients with pathological EMB results (n = 55) the immunohistological diagnosis of active myocarditis was made only in seven patients (12.7%) and LGE was detected only in 17/48 (35.4%).
Interestingly, as expected, subendocardial LGE was detected in this study in four patients with coronary vasospasm and myocarditis but no significant CAD (figs 5C–F). This is in contrast to our previous findings but may be explained by the fact that subjects with coronary vasospasm were excluded in our previous studies. Thus, our findings suggest that subendocardial lesions may occur as a consequence of coronary vasospasm associated with myocarditis. In future studies, the exact meaning of this observation in relation to clinical and histopathological characteristics should be evaluated.
Study limitations
Our patient classification, based on biopsy results, with the methodological limitation of sampling error, is susceptible to an erroneous assignment of some patients to the groups. However, as discussed before we are sure that this overlap was neither significant nor weakened the derived conclusions. Of course, myocarditis is not the only possible reason for the occurrence of coronary vasospasm and chest pain is not always caused by coronary vasospasm. Other causes for atypical chest pain in patients with biopsy-proven myocarditis such as pericarditis cannot be ruled out and have to be kept in mind. Furthermore, other reasons for coronary vasospasm in patients with chest pain (in the absence of biopsy-proven myocarditis), such as atherosclerosis without stenosis, electrolyte disturbances and ethnic predisposition,1 or possible other reasons for atypical chest pain other than coronary vasospasm, such as oesophageal spasm or pulmonary diseases, will have to be considered in future studies.
CONCLUSION
Our results clearly suggest that coronary vasospasm is one of the main reasons for atypical chest pain in subjects with clinical signs of myocarditis and biopsy-proven PVB19 myocarditis. These results are of potential clinical importance since they may offer new treatment options for chest pain symptoms in patients with myocarditis in the absence of CAD.
REFERENCES
Footnotes
Competing interests: None.