Article Text

Abstract
Objective To analyse whether levels of high-sensitivity cardiac troponin (hs-cTn) below their respective 99th percentile can be used as a single parameter to rule out acute myocardial infarction (AMI) at presentation.
Design Prospective, multicentre study.
Main outcome measures We measured hs-cTn using four different methods (hs-cTnT Roche, hs-cTnI Siemens, hs-cTnI Beckman Coulter and hs-cTnI Abbott) in consecutive patients presenting to the emergency department with acute chest pain. Two independent cardiologists adjudicated the final diagnosis. Patients were followed for death or AMI during a mean period of 24 months.
Results Among 2072 consecutive patients with hs-cTnT measurements available, 21.4% had an adjudicated diagnosis of AMI (sensitivity 89.6%, 95% CI 86.4% to 92.3%, negative predictive value (NPV): 96.5%, 95% CI 95.4% to 97.4%). Among 1180 consecutive patients with hs-cTnI Siemens measurements available, 20.0% had AMI (sensitivity 94.1%, 95% CI 90.3% to 96.7%, NPV: 98.0%, 95% CI: 96.6% to 98.9%). Among 1151 consecutive patients with hs-cTnI Beckman Coulter measurements available, 19.7% had AMI (sensitivity 92.1%, 95% CI 87.8% to 95.2%, NPV: 97.5%, 95% CI 96.0% to 98.5%). Among 1567 consecutive patients with hs-cTnI Abbott measurements available, 20.0% had AMI (sensitivity 77.2%, 95% CI 72.1% to 81.7%, NPV: 94.3%, 95% CI 92.8% to 95.5%).
Conclusions Normal hs-cTn levels at presentation should not be used as a single parameter to rule out AMI as 6%–23% of adjudicated AMI cases had normal levels of hs-cTn levels at presentation. Our data highlight the lack of standardisation among hs-cTnI assays resulting in substantial differences in sensitivity and NPV at the 99th percentile.
- CORONARY ARTERY DISEASE
Statistics from Altmetric.com
Introduction
Coronary artery disease (CAD) is the most common manifestation of cardiovascular disease and it is associated with high morbidity and mortality.1 There are different clinical manifestations of CAD including silent ischemia, stable angina pectoris, unstable angina pectoris, acute myocardial infarction (AMI), sudden death and heart failure.1 In Europe and in the USA, almost 15 million patients per year present to the emergency department (ED) with chest pain or other symptoms suggestive of AMI.2 As in most patients acute chest pain is caused by benign disorders and not by AMI, rapid rule out of AMI is fundamental.3 Delayed rule out of AMI increases resource use and time spent in the ED, patient anxiety and the problem of overcrowding in the ED, which itself is associated with increased mortality and morbidity.3
Since the late 1980s, when cardiac troponins (cTns) were first described as biochemical markers for cardiomyocyte damage, there have been important advances in cTn assay technology, which have led to an improvement in the clinical ability to detect and quantify cardiomyocyte damage.4 According to current guidelines, a test with a high ability to diagnose and rule out AMI has to meet two basic criteria: First, it has to detect increased cTn levels in blood that surpass the 99th percentile of cTn levels in a normal reference population, with an imprecision corresponding to ≤10% coefficient of variation (CV) at the upper reference limit.1 ,5–7 Second, a high-sensitivity assay should be able to measure in at least 50% of healthy individuals concentration levels over the assay's limit of detection (LOD) but below the 99th percentile.6 ,7 None of the earlier generation cTn assays, still in clinical use in many institutions, does fulfil these requirements.8 High-sensitivity cardiac troponin (hs-cTn) assays have a 10-fold to 100-fold lower LOD and meet the demand of analytical precision.1 This enables physicians to detect AMI earlier and more frequently in patients presenting with chest pain.2 ,7 The aim of our study was to determine whether hs-cTn values below the 99th percentile can be used as a single parameter to rule out the diagnosis of AMI at presentation.
Methods
Study design and population
Advantageous Predictors of Acute Coronary Syndrome Evaluation (APACE) is an ongoing prospective, international, multicentre study coordinated and designed by the University Hospital Basel (ClinicalTrials.gov number, NCT00470587).2 Consecutive adult patients were enrolled from April 2006 to August 2011 if presenting to the ED with symptoms suggestive of AMI such as acute chest pain, angina pectoris at rest or other thoracic sensations presumably caused by myocardial ischemia with an onset or peak within the last 12 h. Patients were excluded if presenting with terminal kidney failure requiring dialysis. Patients were excluded from analysis if (1) hs-cTnT, hs-cTnI (Siemens), hs-cTnI (Beckman Coulter) or hs-cTnI (Abbott) values were not available in the respective data-files or if (2) the final diagnosis remained unclear after adjudication. All patients provided written informed consent. The study was performed according to the principles of the Declaration of Helsinki and approved by the local ethics committees.
Routine clinical assessment
The initial clinical assessment included clinical history, physical examination, 12-lead electrocardiography (ECG), continuous ECG monitoring, pulse oximetry, standard blood tests and chest radiography.2 Measurements of cTn levels were performed at presentation and 6–9 h later or as long as clinically indicated.9 Timing and treatment of patients were left to the discretion of the attending physician.
Adjudication of final diagnosis
Adjudication of final diagnosis was performed twice for all patients in the core lab (University Hospital Basel) by two independent cardiologists. In the initial analyses, the adjudication of final diagnoses was performed according to the conventional cTn levels used locally to assess the performance of hs-cTn assays.2 ,10–13 In order to also identify patients with small AMIs that were missed by the conventional assays, patients were readjudicated using hs-cTnT values in addition to the conventional cTn values.
Measurements of hs-cTn
hs-cTnT (Roche) was measured on the Elecsys 2010 analyser (Roche Diagnostics) with a LOD determined to be 5 ng/l, an imprecision corresponding to 10% CV reported at 13 ng/l and the 99th percentile of a healthy reference population at 14 ng/l.5 For this assay, normal hs-cTnT levels were defined as those below 14 ng/l and elevated levels as ≥14 ng/l. The measurements of the last 876 recruited patients (patient 1196–2072) were performed with lots that needed a revision of the calibration curve. Thus, they were corrected using non-linear regression correction.14–16
Measurement of Beckman Coulter hs-cTnI was performed on the Access 2 analyser using an investigational prototype assay with—according to the manufacturer—a LOD of 2 ng/l, a 99th percentile at 9 ng/l, with a CV of less than 10%. For this assay, normal hs-cTnI levels were defined as below 9 ng/l and elevated levels as ≥9 ng/l.
For hs-cTnI (Siemens) Dimension Vista 1500 immunoassay system was used, which has—according to the manufacturer—an LOD of 0.5 ng/l, a 99th percentile at 9 ng/l, and a CV of less than 10% at 3 ng/l.6 Normal hs-cTnI levels were defined as below 9 ng/l and elevated levels as ≥9 ng/l.
Measurement of hs-cTnI (Abbott) was performed with a final precommercial release version of the ARCHITECT High Sensitive STAT Troponin I (hsTnI) assay (Abbott Laboratories, Abbott Park, IL) with a 99th percentile concentration of 26.2 ng/l, a corresponding CV of <5% and a LOD of 1.9 ng/l.6 ,17 For this assay, normal hs-cTnI levels were defined as below 26.2 ng/l and elevated levels as ≥26.2 ng/l. Long-term stability of TnI has been demonstrated previously.18 Good correlation between plasma and serum has been demonstrated.19 Furtherinformation to the adjudication of the final diagnosis and to measurements of hs-cTn are described in the online supplementary material.
Follow-up
The primary endpoint was all cause-mortality and AMI rate during follow-up. Further information is described in the online supplementary material.
Statistical analysis
Categorical variables are presented as percentages and continuous variables are presented as median and interquartile range (IQR). Continuous, skewed distributed variables were compared with the Mann–Whitney U test and categorical variables were compared using the Pearson χ2-square test. Kaplan–Meier analysis was performed for the endpoint of death during follow-up and for the AMI rate during follow-up. Statistical significance was determined with the log-rank test. All hypothesis testing was two-tailed and p value<0.05 was described as statistically significant. All statistical tests were performed using SPSS for Windows 21.0 (SPSS Inc., Chicago, Illinois) and MedCalc 11.2.1.0 (MedCalc Software).
Results
Patient characteristics
Figure 1 displays the detailed flow of patients. A total of 2245 patients consented to inclusion in this multicentre study, of whom 2072 were available for inclusion in the analysis of hs-cTnT levels, 1180 were included for analysis of hs-cTnI (Siemens), 1151 for analysis of hs-cTnI (Beckman Coulter) and 1567 for the analysis of hs-cTnI (Abbott). Table 1 provides baseline characteristics of all included patients with hs-cTnT measurements. Baseline characteristics of the patients with hs-cTnI measurements were similar to the ones with hs-cTnT (data not shown).
Baseline characteristics of included patients
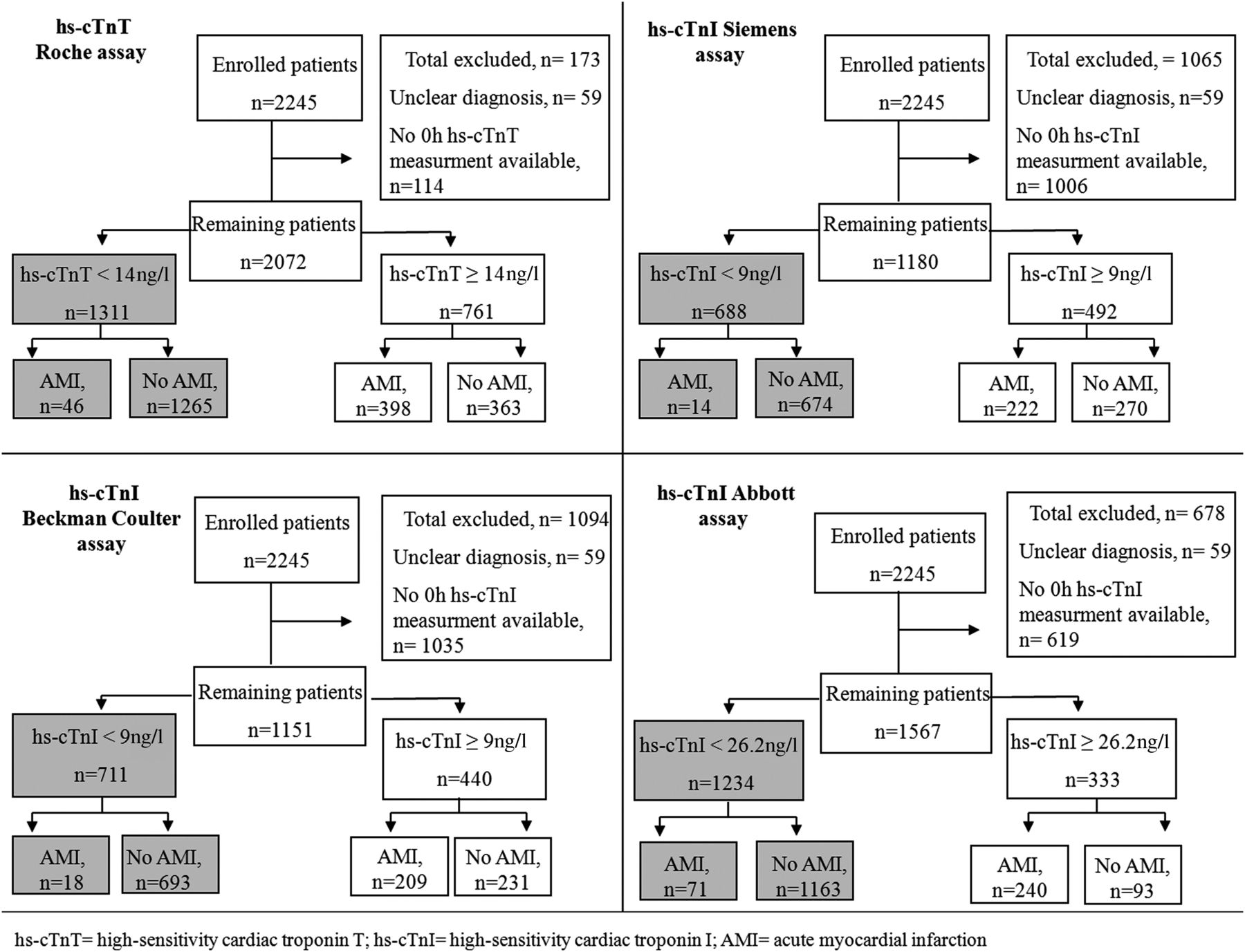
Study flow diagram.
The diagnosis of AMI was adjudicated in 444 (21.4%) patients with hs-cTnT measurements, in 236 (20.0%) with hs-cTnI (Siemens), in 227 (19.7%) with hs-cTnI (Beckman Coulter) and in 311 (19.8%) with hs-cTnI measurments (Abbott).
At presentation, all four hs-cTn assays showed significantly higher levels in patients with AMI compared with patients without AMI. These results, the results of the second adjudication of the final diagnosis based on hs-cTn values and the results of the subgroup analysis of patients with non-ST-elevation myocardial infarction (NSTEMI) are shown in the online supplementary material.
Normal levels of hs-cTnT at presentation were measured in 63.3% of patients, 58.3% of patients presented with normal levels of hs-cTnI (Siemens), 61.8% presented with normal levels of hs-cTnI (Beckman Coulter) and 78.7% presented with normal levels of hs-cTnI (Abbott).
Normal levels of hs-cTn at presentation for rule out of AMI
In patients with hs-cTnT measurements and diagnosed AMI, 398 (89.6%) presented with elevated levels of hs-cTnT and 46 (10.4%) had normal levels at presentation. As shown in table 2, the sensitivity of hs-cTnT at the time of presentation using the conventional 99th percentile at 14 ng/l was 89.6% (95% CI 86.4% to 92.3%) and the negative predictive value (NPV) was 96.5% (95% CI 95.4% to 97.4%). In patients with hs-cTnI (Siemens) measurements at presentation and the diagnosis of AMI, 222 (94.1%) had initially elevated hs-cTnI levels (≥9 ng/l) and 14 (5.9%) showed normal levels, resulting in a sensitivity of 94.1% (95% CI 90.3% to 96.7%) and a NPV of 98.0% (95% CI 96.6% to 98.9%). In patients with hs-cTnI measurements (Beckman Coulter) at presentation and diagnosed AMI, 209 (92.1%) showed initially elevated hs-cTnI levels (≥9 ng/l) and 18 patients (7.9%) had normal levels. Thus, the sensitivity for AMI with this assay was 92.1% (95% CI 87.8% to 95.2%) and the NPV was 97.5% (95% CI 96.0% to 98.5%). In patients with hs-cTnI (Abbott) measurements at presentation and the diagnosis of AMI, 240 (77.2%) had initially elevated hs-cTnI levels (≥26.2 ng/l) and 71 (22.8%) showed normal levels, resulting in a sensitivity of 77.2% (95% CI 72.1% to 81.7%) and a NPV of 94.3% (95% CI 92.8% to 95.5%).
Sensitivity and specificity of different hs-cTn assays for AMI at respective upper limit stratified by time from symptom onset
All four hs-cTn assays showed their highest sensitivity and their highest NPV in patients presenting after 6 h from symptom onset (Roche, n=999; Siemens, n=572; Beckman Coulter, n=561; Abbott, n=775). Further details of patients presenting after 6 h and the results of subgroup analysis of patients with measurements available for all four hs-cTn assays are described in the online supplementary material.
Early presenters
The majority (60.9%, 28 of 46) of patients with AMI who had normal levels of hs-cTnT at presentation were early presenters (<3 h from symptom onset). As shown in table 2, early presenters showed lower values in sensitivity for the cut-off value 14 ng/l (73.8%, 95% CI 64.5% to 81.9%) and in NPV (92.3%, 95% CI 89.0% to 94.8%) compared to late presenters (≥3 h). There sensitivity is 94.7% (95% CI 91.7% to 96.8%) and NPV is 98.1% (95% CI 97.0% to 98.9%).
Death and AMI rate during the follow-up period
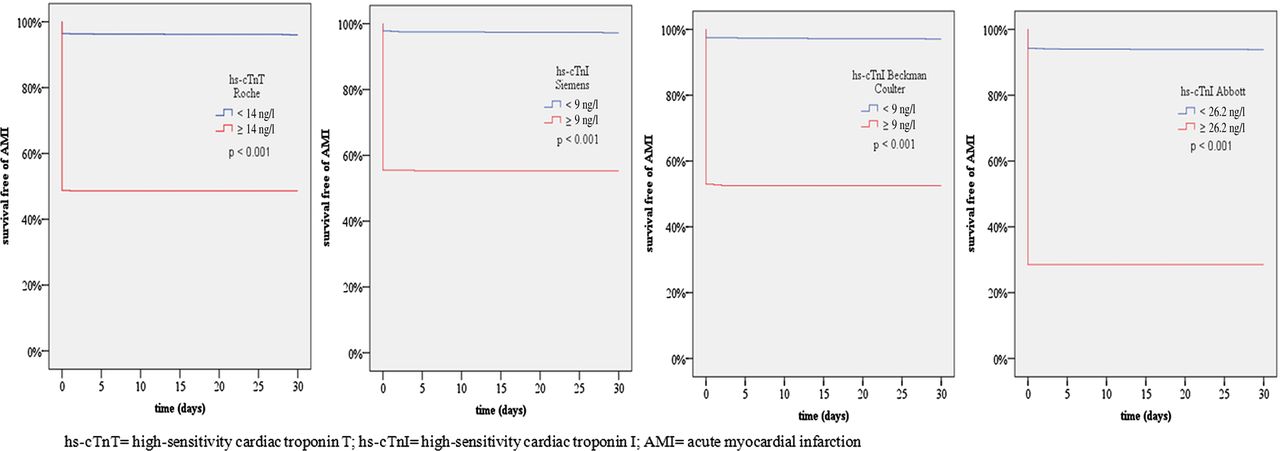
As outlined in figure 2 and figure 3, during the first 30 days of follow-up, mortality rate and AMI rate were significantly higher in patients with elevated hs-cTn at presentation than in patients with normal hs-cTn at presentation. Further details are described in the online supplementary material.

Cumulative mortality rate within 30 days according to the respective 99th percentile of hs-cTn. Access the article online to view this figure in colour.

{kind=link}
{kind=link}
{kind=link}
Cumulative rate of AMI within 30 days according to the respective 99th percentile of hs-cTn. Access the article online to view this figure in colour.
Discussion
We performed a prospective, international, multicentre study enrolling unselected patients presenting to the ED with acute chest pain. The aim of this analysis was to evaluate four different hs-cTn assays and to assess whether hs-cTn values below their respective 99th percentile can be used as a single parameter to rule out the diagnosis of AMI at presentation. We report five major findings:
First, the percentage of AMI patients having normal levels of hs-cTn at presentation varied substantially among the four different hs-cTn assays used and ranged from 6% to 23%. These differences among hs-cTn assays may be related to analytical details of the specific assays, differences among the reference population chosen to define the respective 99th percentiles of each assay as well as potential pathophysiological differences including release kinetics between cTnT and cTnI. The incidence of normal hs-cTn levels in this cohort of unselected acute chest pain patients was similar as the incidence reported in the previous studies recruiting unselected patients.2 ,7 ,20 Second, the vast majority of patients with acute chest pain and normal levels of hs-cTn did not have an AMI. The NPV of the hs-cTn assays examined for normal levels of hs-cTn ranged from 94% to 98%. Third, for all four assays, sensitivity and NPV were higher in patients presenting after 6 h from symptom onset. These results indicate that the rule out of AMI could possibly be performed with a single hs-cTn measurement in conjunction with the 12-lead ECG and a full clinical assessment in patients presenting within 6 h from symptom onset. However, all four assays showed a lower sensitivity in patients presenting within 3 h from symptom onset. This observation confirmed the time-dependent release of cTn from the injured myocardium. It also highlights the need for particular caution regarding the rule out of AMI with hs-cTn in early presenters, especially regarding the high difference in sensitivity of hs-cTnI assays in early presenters. Fourth, differences in NPV and PPV at the 99th percentile among the different hs-cTnI assays were substantial and did not seem to be adequately explained by differences in assay sensitivities. We consider the lack of standardisation, including the use of different reference populations to define the respective 99th percentiles, the most likely explanation for these substantial differences among hs-cTnI assays.21 For example, more than three times as many patients with AMI had hs-cTnI levels in the normal range with the Abbott assay as compared with the Siemens or Beckman Coulter assay.
One of the basic criteria that must be met to diagnose AMI is the detection of a rise and/or fall of cTn that surpass the 99th percentile of cTn levels in a normal reference population.1 ,22 As there is no universally accepted standard of the composition of the reference population that results in important differences in age as well as work-up performed in order to ensure that the healthy reference population is really healthy, most of 99th percentile values reported by manufacturers and in the literature are deduced from different study populations.21 For the hs-cTn assays used in our analysis the 99th percentiles range from 9 to 26.2 ng/l. In case of hs-cTnI (Abbott), choosing a higher 99th percentile resulted in a higher specificity and PPV at the 99th percentile, with the cost of having the highest percentage of patients with AMI and ‘normal’ levels of hs-cTnI at presentation, and therefore, lowest values for sensitivity and NPV.
Fifth, during 30 days follow-up, mortality rate was 17 times higher in patients with elevated hs-cTnT at presentation than in patients with normal hs-cTnT at presentation. Mortality in patients with elevated measurements of hs-cTnI was about 10 times higher than in patients with normal levels. Similarly, the rate of AMI during 30 days follow-up was significantly higher in patients with elevated hs-cTn levels compared to patients with normal hs-cTn levels at presentation, irrespective of the hs-cTn assay used. Our results support previous findings, which showed that the implementation of hs-cTn assays identifies patients at high risk of death or recurrent AMI.23 ,24
A test with a high ability to rule out ACS, that is, a test with a high NPV is of paramount importance for clinicians because it improves the diagnostic triage and facilitates discharge from the ED.1 ,25 Results from two multicentre studies, in which the conventional 4th generation cTnT assay was compared with sensitive and hs-cTn assays, showed that the diagnostic accuracy of the new hs-cTn assays is significantly higher compared with the standard assays, especially in early presenters.2 ,20 One of them, Keller et al, reported a NPV of 84.1% for a single sensitive troponin I assay, when measured in patients presenting within 3 h of chest pain onset.20 Recently, the same study group presented data about hs-cTnI measurements at admission and reported a NPV of 94.7% and a sensitivity of 82.3%.7 Our results support these findings, as all four hs-cTn assays showed comparable NPVs.
One of the particular strengths of this analysis is the adjudication of the final diagnosis using hs-cTnT levels in conjunction with all other information becoming available during work-up. This also allows the accurate detection of small AMIs, which might have been missed in previous studies that relied on conventional cTn levels for the adjudication. Thereby, this analysis extends and corroborates recent findings regarding the utility of normal hs-cTnT levels and the diagnosis of an acute coronary syndrome (AMI and unstable angina) in general.13
Our findings may help to highlight that hs-cTn values should only be used in conjunction with the 12-lead ECG and full clinical assessment. Although normal hs-cTn levels at presentation argue in favour of a diagnosis other than AMI and are associated with a very low risk of death and AMI during follow-up, other clinical information including the second hs-cTn level obtained after 3–6 h—especially in early presenters—have a critical role to definitely rule out AMI as the index event.1
Limitations
Several potential limitations of this study should be mentioned. First, we assessed the performance of normal levels of four different hs-cTn assays. Although we obtained consistent results in all four assays and consequently suppose that it can be generalised to all hs-cTn assays, further studies need to confirm this assumption. Second, we cannot comment on patients with terminal kidney failure requiring dialysis as these patients were excluded from analysis. Third, as it is a prospective, observational study, we cannot determine the exact clinical benefit associated with risk stratification and improved diagnosis. Fourth, we underlined that one of the strengths of our study was the adjudication of diagnosis using the values of hs-cTnT. Although it could theoretically bias a direct comparison of the diagnostic accuracy of hs-cTnT versus hs-cTnI, we do not expect an alteration of the key message of our study.
Conclusions
Among consecutive patients with acute chest pain, depending on the hs-cTn assay used, 6% to 23% of adjudicated AMI cases had normal levels of hs-cTn levels at presentation. Therefore, although the majority of acute chest pain patients with normal levels of hs-cTn will be found to have causes other than AMI, normal hs-cTn levels at presentation should not be used as a single parameter to rule out AMI. This caveat applies particularly to early presenters. In addition, our data highlight the lack of standardisation among hs-cTnI assays resulting in substantial differences in NPV and PPV at the 99th percentile.
Acknowledgments
We are indebted to the patients who took part in the trial, to the ED staff, the laboratory technicians, and in particular to Irina Klimmeck, Melanie Wieland, Esther Garrido, Kirsten Hochholzer, Janine Voegele, Ina-Maria Ferel and Fausta Chiaverio for their most valuable support. We also thank Pascal Benkert for his advices in statistics.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
RH and MRG have contributed equally and should be considered first author.
-
Contributors Guarantors: RH, CM. Study concept, design and supervision: CM. Conduct of the study: all authors. Analysis and interpretation of data: RH, MR, CM. Drafting of the manuscript: RH, MR, CM. Critical revision of the manuscript for important intellectual content and approvement of the final version of the manuscript: all authors.
-
Funding This work was supported by the Swiss National Science Foundation, the Swiss Heart Foundation, 8sense, Abbott, Brahms, Nanosphere, Roche, Siemens, and the Department of Internal Medicine of the University Hospital Basel.
-
Competing interests Prof. Mueller has received research grants from the Swiss National Science Foundation [PP00B-102853] and the Swiss Heart Foundation, the Stiftung für kardiovaskuläre Forschung Basel, 8sense, Abbott, ALERE, Brahms, Critical Diagnostics, Nanosphere, Roche, Siemens, and the Department of Internal Medicine, of the University Hospital Basel, as well as speaker honoraria from Abbott, ALERE, Brahms, Novartis, Roche, and Siemens. All other authors declare that they have no conflict of interest with this study. The hs-cTn assays were donated by their respective manufacturers. The funding sources were not involved in the design of the trial, the gathering, analysis and interpretation of data, the writing of the manuscript or the decision to publish the paper.
-
Patient consent Obtained.
-
Ethics approval Swissethics.
-
Provenance and peer review Not commissioned; externally peer reviewed.