Article Text

Abstract
Objectives To determine the accuracy of CHADS2 and CHA2DS2-VASc tools for predicting ischaemic stroke or transient ischaemic attack (TIA) and death in patients without a history of atrial fibrillation or flutter (AF).
Methods The study included 20 970 patients without known AF enrolled in the Alberta Provincial Project for Outcomes Assessment in Coronary Heart disease (APPROACH) prospective registry who were discharged after an acute coronary syndrome (ACS) between 2005 and 2011. The outcome measures were incident ischaemic stroke, TIA or death from any cause.
Results Over a median follow-up of 4.1 years, 453 patients (2.2%) had a stroke (n=297) or TIA (n=156) and 1903 (9.0%) died. The incidence of stroke or TIA increased with increases in each risk score (p<0.001), with an absolute annual incidence ≥1% with CHADS2 ≥3 or CHA2DS2-VASc ≥4. Both CHADS2 and CHA2DS2-VASc scores had acceptable discrimination performance (C-statistic=0.68 and 0.71, respectively). The mortality rate was also greater in patients with higher CHADS2 and CHA2DS2-VASc scores (p<0.0001).
Conclusions In patients with ACS but no AF, the CHADS2 and CHA2DS2-VASc scores predict ischaemic stroke/TIA events with similar accuracy to that observed in historical populations with non-valvular AF, but with lower absolute event rates. Further study of the utility of the CHADS2 and CHA2DS2-VASc scores for the assessment of thromboembolic risk and selection of antithrombotic therapy in patients without AF is warranted.
Statistics from Altmetric.com
Introduction
Each year, nearly 800 000 people in the USA have a stroke—one every 40 s.1 Stroke leads to direct and indirect costs in the USA of over $38 billion and is the fourth leading cause of death.1 Approximately 15% of all strokes are attributed to non-valvular atrial fibrillation or atrial flutter (AF).2 In such patients, CHADS2 and CHA2DS2-VASc have emerged as the dominant prediction tools to estimate a patient's risk of stroke or systemic thromboembolism.3 ,4
CHADS2 (congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, previous stroke/TIA (transient ischaemic attack) (double score)) and CHA2DS2-VASc (congestive heart failure, hypertension, age ≥75 years (double score), diabetes mellitus, previous stroke/TIA (double score), vascular disease, age 65–74 years, sex class (female))4 have been validated in an independent patient population of 90 490 patients with AF not treated with oral anticoagulants.5 Although the predictive values of CHADS2 and CHA2DS2-VASc scores for ischaemic stroke were modest (c-statistics 0.66 and 0.67, respectively), there was a clear increase in annual risk with increasing scores using either predictive tool. Recently, CHADS2 and CHA2DS2-VASc clinical tools have been reported to have predictive capacity for outcomes in patients without known AF, including the risk of death after stroke,6 the risk of new onset AF,7 the risks of stroke or death after coronary artery bypass grafting,8 ,9 the risk of stroke in unselected patients,10 the risk of stroke in patients with stable coronary artery disease11 and the risk of stroke after an acute coronary syndrome (ACS).12
The purposes of the present study were to further evaluate the utility of the CHADS2 and CHA2DS2-VASc clinical tools for the prediction of stroke, TIA, death and their composites in a very large, well-characterised population of patients discharged after an ACS. This analysis also permits an indirect assessment of the risk of stroke independently conferred by AF in this patient population.
Methods
Study population and data sources
In the province of Alberta, Canada, all cardiac care is coordinated by a single organisation (Alberta Health Services), divided into five regional zones. Using its administrative Discharge Abstract Database, we identified all patients discharged alive from acute care hospitals in the Southern and Calgary zones (2011 population: 1.7 million) with a primary diagnosis of ACS between 1 April 2005 and 31 March 2011. ACS was defined using International Classification of Diseases (ICD) 10 codes for acute myocardial infarction and unstable angina. To enhance clinical detail and minimise missing data, this database was linked with the Alberta Provincial Project for Outcomes Assessment in Coronary Heart Disease (APPROACH) database.13 APPROACH is a prospective registry capturing clinical data on all patients undergoing cardiac catheterisation or revascularisation in Alberta. The University of Calgary Health Research Ethics Board approved APPROACH data collection, including the waiver of individual consent for enrolment and linkages with secondary sources.
Case definitions
Baseline characteristics and elements of the CHADS2 and CHA2DS2-VASc scores during the index hospitalisation were obtained from the APPROACH database and were merged with administrative data.13 All 25 primary and secondary hospital discharge diagnostic codes were scanned to evaluate risk factor status. Congestive heart failure was considered present for patients with a history of heart failure or a measured left ventricular ejection fraction <0.35.
Timing and diagnoses of subsequent hospitalisations up to 31 March 2012 were determined using ICD10 codes. The follow-up outcomes were death or a subsequent discharge diagnosis of ischaemic stroke or TIA. Data on mortality were provided by linkage with Alberta Vital Statistics. Stroke was defined by ICD-10 codes I63.x and I64.x excluding I63.6 and TIA was defined by ICD-10 codes of G45.x excluding G45.4. We previously validated the sensitivity and specificity of ICD-10 codes for stroke diagnosis and for stroke risk factors against chart review.14 AF was identified using ICD-10 codes I48.x and I97.
Statistical analysis
The distributions of CHADS2 and CHA2DS2-VASc scores and their individual components were compared between those with and without AF at index discharge using the χ2 test. In those without AF, the annual incidence of ischaemic stroke, TIA and death, as well as their composites, were calculated for each risk score. Logistic regression modelling was used to determine stratum-specific ORs and the predictive accuracy of the CHADS2 and CHA2DS2-VASc scores using receiver operating characteristic (ROC) analysis. For survival analysis, risk scores were dichotomised using a threshold that identified a cohort with an absolute annual risk of stroke or TIA ≥1%, which would trigger consideration of anticoagulant therapy in patients with AF. Associated HRs were calculated using Cox models, after verifying the proportional hazards assumption with Schoenfeld residuals. Two-sided p values <0.05 identified statistical significance. All analyses were performed with SAS V.9.2 (Cary, North Carolina, USA).
Results
Between 1 April 2005 and 31 March 2011, 40936 patients were discharged alive after admission with a primary diagnosis of ACS. The study cohort consisted of 23 042 of these patients (56.3%) for whom linkage with the APPROACH registry was possible. Table 1 compares the baseline characteristics and CHADS2 and CHA2DS2-VASc scores of those with (n=2072, 9.0%) and those without (n=20970, 91.0%) a diagnosis of AF at baseline. Patients without AF were younger, were more likely to be male and had a lower prevalence of each of the components of the CHADS2 and CHA2DS2-VASc scores with the exception of vascular disease, which, by virtue of the selection criteria, was present in all patients. Consequently, the CHADS2 and CHA2DS2-VASc scores were significantly lower in those without known AF (χ2 p<0.0001).
Baseline characteristics and stroke risk scores
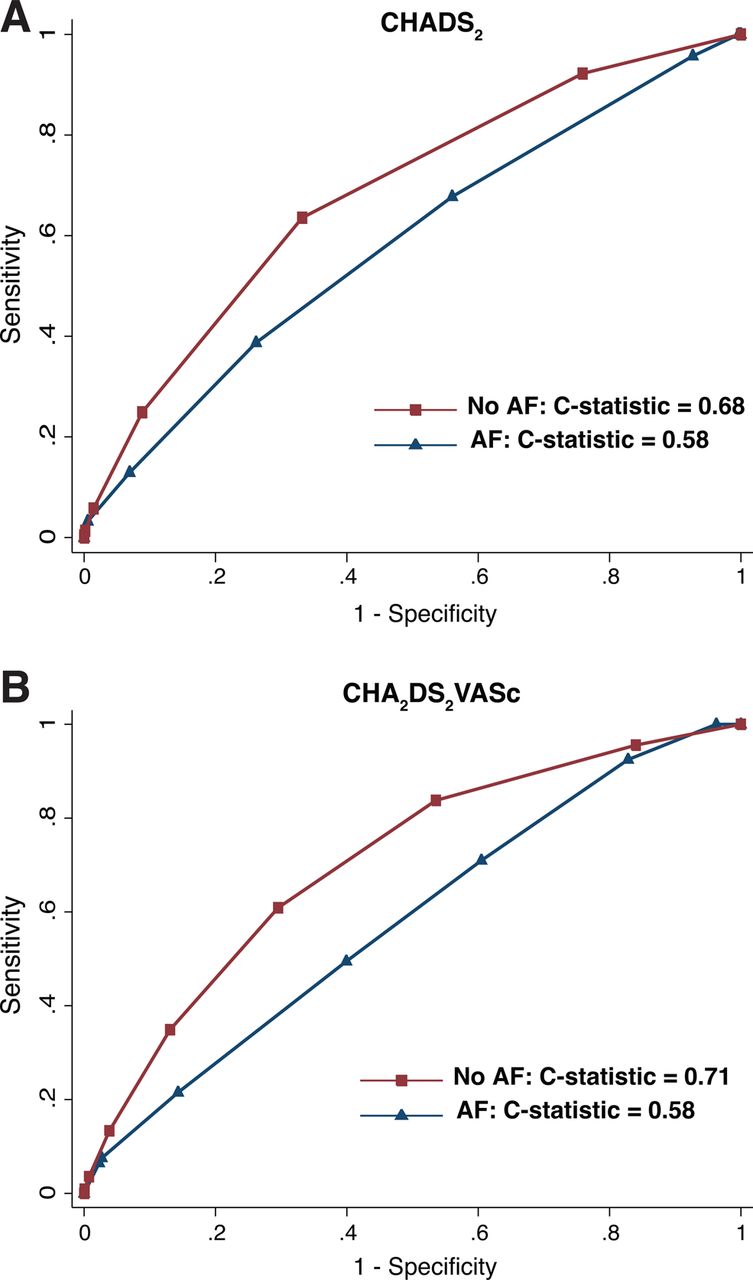
Over a median follow-up of 4.1 years, 297 (1.4%) and 453 (2.2%) patients without baseline AF had a subsequent hospital discharge diagnosis of stroke and stroke or TIA, respectively, and 1903 (9.1%) patients died. A total of 947 (4.5%) patients had a subsequent hospital discharge diagnosis of AF. Table 2 summarises the associations between CHADS2 and CHA2DS2-VASc scores and incident ischaemic stroke, TIA and death from any cause for patients without AF at baseline. Each component of the prediction rules, except for age 65–74 years, was significantly associated with outcomes on univariable analysis. The strongest predictors of incident stroke were a prior history of stroke or TIA: OR 4.82, 95% CI 2.59 to 8.97 and age ≥75: OR 3.45, 95% CI 2.72 to 4.37. Stepwise increases in the annual incidence of ischaemic stroke, stroke or TIA, and stroke, TIA or death were observed with each increment in both CHADS2 and CHA2DS2-VASc scores (figure 1). The sensitivity and specificity of the scores, at each risk level, for prediction of stroke or TIA are presented in online supplementary table 1. When integrated, these data demonstrate that CHADS2 and CHA2DS2-VASc scores provide similar, moderate discriminatory performance using ROC analysis (figure 2). The C-statistic for prediction of incident ischaemic stroke or TIA was 0.68 (95% CI 0.66 to 0.71) for CHADS2 and 0.71 (95% CI 0.68 to 0.73) for CHA2DS2-VASc in those without baseline AF. The C-statistics were 0.58 for each score in patients with baseline AF. A CHADS2 score of ≥3 or a CHA2DS2-VASc score of ≥4 identified patients with an absolute annual incidence of ischaemic stroke or TIA of ≥1%. For each prediction tool, higher scores were associated with increased risk of ischaemic stroke or TIA (figure 3) and with increased risk of the composite endpoint of ischaemic stroke, TIA or death from any cause (see online supplementary figure 1).
Stroke, TIA and death in those without atrial fibrillation at discharge

Graded increase in risk of stroke, transient ischaemic attack (TIA) and death by CHADS2 and CHA2DS2-VASc scores. Incidence of ischaemic stroke, TIA or stroke and stroke, TIA or death stratified by, in patients without a baseline history of atrial fibrillation. Non-parametric trend p<0.001 for each grouping.
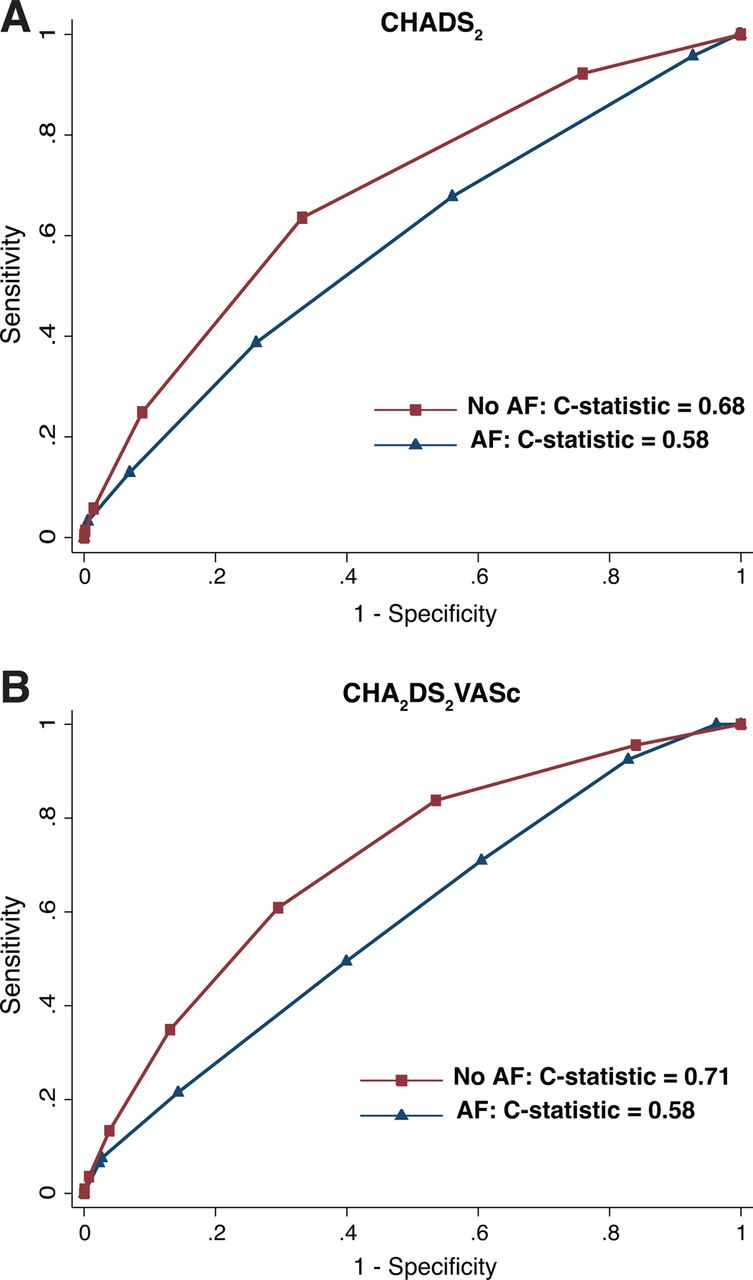
Discrimination performance of CHADS2 and CHA2DS2-VASc scores for prediction of stroke or transient ischaemic attack (TIA). Receiver operator characteristic curves for the performance of CHADS2 (A) and CHA2DS2-VASc (B) scores in predicting incident stroke or TIA.

{kind=link}
{kind=link}
{kind=link}
Association between increased CHADS2 and CHA2DS2-VASc scores and the risk of ischaemic stroke or transient ischaemic attack (TIA). Kaplan–Meier failure plots for the risk of ischaemic stroke or TIA stratified by CHADS2 score (A) and by CHA2DS2-VASc score (B).
CHADS2 and CHA2DS2-VASc scores also predicted subsequent hospital discharge with a diagnosis of AF in those without pre-existing AF (see online supplementary table 2). The annual incidence of AF increased in a stepwise fashion and reached 3.85% in patients with CHADS2 ≥3 and 2.52% in those with CHA2DS2-VASc ≥4. Each score had reasonable discrimination performance for prediction of incident AF (C-statistic=0.71 for each score). To determine whether the associations between CHADS2 and CHA2DS2-VASc scores and stroke or TIA were mediated by incident AF, all analyses were repeated after exclusion of patients who developed AF during follow-up (data not shown) and in models in which incident AF was added as a covariate with the risk scores (see online supplementary table 3). No significant differences in effect estimates or their interpretations were noted in either analysis.
The group with no risk factors for stroke according to CHADS2 (N=4981) had an annual risk of ischaemic stroke of 0.15%, and the patient group with no risk factors for stroke other than vascular disease according to CHA2DS2-VASc (N=3300) had an annual risk of ischaemic stroke of 0.11%. In the independent validation of the CHADS2 and CHA2DS2-VASc tools in patients with non-valvular AF not treated with vitamin K antagonists, the annual risks of ischaemic stroke were 0.6% for AF patients with CHADS2 scores of 0 and 0.6% for AF patients with CHA2DS2-VASc scores of 1.6 These results suggest that the contemporary risk of ischaemic stroke independently imparted by a history of AF is between fourfold (0.6%/0.15%) and sixfold (0.6%/0.11%).
Discussion
This analysis demonstrates that the CHADS2 and CHA2DS2-VASc prediction tools used to assess the risk of thromboembolic events in patients with non-valvular AF have similar utility in survivors of ACS without known AF. Increasing scores using either tool identified increasing risks of ischaemic stroke, of TIA, of death and of their composites. Nevertheless, the absolute ischaemic stroke rate in this non-AF patient cohort was lower than that reported in patients with AF, supporting the contention that AF is an independent risk factor for ischaemic stroke (increasing the annual risk fourfold to sixfold). An annual rate of stroke or TIA of >1%, often used to identify patients with AF in whom the benefits of long-term oral anticoagulation may outweigh the risks of bleeding, was observed in non-AF patients only when the CHADS2 score was ≥3 or the CHA2DS2-VASc score was ≥4. Each clinical prediction tool had moderate discriminatory capacity (C-statistics of 0.68 for CHADS2 and 0.71 for CHA2DS2-VASc) similar to those reported in validations of these tools in patients with non-valvular AF.6 ,15 Both CHADS2 and CHA2DS2-VASc scores also predicted incident AF. Patients with higher risk scores also had higher annual incidences of death, mostly unrelated to ischaemic stroke.
These findings are congruent with those of recent reports of small patient populations without AF. Welles et al11 reported the utility of the CHADS2 score in 916 patients with stable coronary artery disease but no history of AF. The risk of ischaemic stroke or TIA increased with higher CHADS2 scores, with a C-statistic of 0.65, and clinically relevant event rates emerged with CHADS2 scores ≥4. Poçi et al12 reported the utility of the CHADS2 score in 2327 ACS survivors with or without AF. Increasing CHADS2 scores predicted mortality in all patients but, as in our experience, predicted stroke only in patients without AF. Similar observations have been reported in other patient groups without AF, including after coronary artery bypass surgery,8 ,9 after a first stroke/TIA,6 ,16 with left ventricular non-compaction,17 and in a population-based study from China.10 The present report adds to this evolving literature by validating previous findings and by refining their point estimates in the largest cohort to date. The smaller sample sizes of prior reports evaluating stroke and TIA mandated analyses by groups of CHADS2 and CHA2DS2-VASc scores (low, intermediate and high risk). The larger sample of this study allows analysis by individual scores in a stepwise fashion and permits determination of threshold scores for prediction of clinically relevant event rates.
Relationships among CHADS2 and CHA2DS2-VASc, stroke type and atrial fibrillation
That the CHADS2 and CHA2DS2-VASc scores predict stroke events in patients without AF is not surprising. First, components of these scores are associated with ischaemic strokes that do not require AF-associated cardioembolism. The Atherosclerosis Risk In Communities (ARIC) investigators reported that the strength of associations and population attributable risks for hypertension, age, diabetes and gender were similar for lacunar, large artery thrombotic and cardioembolic stroke subtypes.18 Furthermore, higher CHADS2 scores are associated with increased cerebral atherosclerosis,19 and patients with heart failure are at risk of embolism from ventricular thrombi even in sinus rhythm.20 A recent study investigating mechanisms of stroke in patients with AF found that increasing CHADS2 scores were associated with left ventricular sources of embolism rather than left atrial sources.21 Furthermore, CHADS2 and CHA2DS2-VASc scoring systems include the main risk factors for non-valvular AF.22 Therefore, as reported here, higher scores identify patients likely to develop AF, which may be asymptomatic. In a recent prospective study of patients with implanted pacemakers or defibrillators, 10% of 2451 patients without known AF had asymptomatic atrial arrhythmias lasting at least 6 min in the first 3 months of monitoring, a feature that was associated with subsequent ischaemic stroke.23 In our study, a graded increase in event rates with increasing CHADS2 score was seen even after adjusting for incident AF.
In both the present study and that of Poçi et al,12 discriminatory performance of the CHADS2 and CHA2DS2-VASc scores, measured by the C-statistic, was better in patients without, rather than with, AF. These findings should not cast doubt on the utility of these scores in patients with AF as they are likely a function of routine clinical use of risk scores for selection of antithrombotic therapy in patients with AF.
Clinical implications
Survivors of an ACS are at risk for subsequent vascular events, including stroke. We have shown that such patients who do not have AF but have a CHADS2 score ≥3 or a CHA2DS2-VASc score ≥4 have an annual incidence of stroke or TIA of >1%. Could this residual risk be reduced by aggressive antithrombotic therapy? Randomised trials comparing adjusted dose warfarin to placebo in patients treated with aspirin after myocardial infarction demonstrated a halving of stroke rate.24 However, these trials were conducted before routine use of coronary stents and dual antiplatelet therapy. Recent trials have studied the use of dabigatran,25 apixaban26 or rivaroxaban27 after ACS in patients receiving contemporary therapy. CHADS2 and CHA2DS2-VASc scores were not explicitly used to select patients, but each of the three trials used elements from the scores as inclusion criteria. The trials involving dabigatran and apixaban were stopped early because of increased bleeding rates. The trial of rivaroxaban, using lower dosages than in patients with AF, suggested a reduction in recurrent ischaemic events or death with a less worrisome increase in bleeding. Although use of the CHADS2 or CHA2DS2-VASc prediction tools can identify higher risk patients without a history of AF, studies demonstrating whether or not such patients benefit from oral anticoagulation have not yet been done. Meanwhile, the data suggest that screening for AF in those patients with high CHADS2 or CHA2DS2-VASc scores may be warranted.28 ,29
Limitations
This analysis used registry and administrative data that may be subject to misclassification of both risk factors and outcomes. However, previous publications validate both the use of APPROACH data to enrich administrative records and the use of ICD-10 codes for ascertainment of stroke outcomes.13 ,14 Nevertheless, these data do not allow classification of ischaemic stroke subtypes. Ascertainment of incident AF is incomplete since it was identified using hospital discharge data. However, since AF is asymptomatic in many patients, only intensive rhythm monitoring would have correctly classified all patients. Finally, incorporation of longitudinal prescription data, which was unavailable, may have increased the accuracy of the predictive models.
Conclusions
In patients with ACS but no history of AF, CHADS2 and CHA2DS2-VASc scores predict ischaemic stroke; TIA; death; ischaemic stroke or TIA; and ischaemic stroke, TIA or death with similar accuracies to those observed in historical populations with non-valvular AF. However, in patients without AF, the scores predict ischaemic stroke or TIA event rates that are lower than in patients with non-valvular AF. Further investigation of the utility of the CHADS2 and CHA2DS2-VASc scores for assessment of thromboembolic risk and selection of antithrombotic therapy in patient populations without AF is warranted.
Key messages
What is known on this subject?
-
The CHADS2 and CHA2DS2-VASc scores were derived and validated in patients with non-valvular atrial fibrillation or atrial flutter (AF) for quantifying risk of stroke or systemic thromboembolism and have recently been reported to have predictive capacity in patients without AF.
-
However, prior studies followed small patient cohorts and, accordingly, considered the predictive values of these scores in low and high groupings that do not allow precise estimation of absolute risks or identification of threshold values for possible intervention.
What might this study add?
-
CHADS2 and CHA2DS2-VASc scores predicted incident stroke or transient ischaemic attack in a population of over 20 000 patients without AF discharged after an acute coronary syndrome (ACS) with accuracies similar to the historical AF patient cohorts from which they were derived.
How might this impact on clinical practice?
-
ACS patients without AF but with a CHADS2 score ≥3 or a CHA2DS2-VASc score ≥4 have an absolute annual incidence of stroke or transient ischaemic attack that is large enough to merit consideration for anticoagulation, although randomised data in support of this approach are as yet lacking.
Acknowledgments
The authors thank Mei Zhang, MSc, for assistance with data analysis. Ms. Zhang is an employee of the APPROACH programme. We also acknowledge Dr Matthew James, MD PhD, for critical review of the manuscript, for which he received no compensation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Collaborators APPROACH Investigators.
-
Contributors Study concept and design, and study supervision: LBM, WAG, MK and SBW. Acquisition of data: DG and DAS. Analysis and interpretation of data and drafting of the manuscript: LBM, DAS and SBW. Critical revision of the manuscript for important intellectual content: all authors. Statistical analysis: DAS. Obtained funding: SBW. Administrative, technical or material support: DG. All authors had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. SBW is the study guarantor.
-
Funding Funding for this analysis was provided by an unrestricted grant from Alberta Health Services. Alberta Health Services had no role in the design and conduct of the study; the collection, management, analysis, and interpretation of the data; the preparation, review or approval of the manuscript; or the decision to submit the manuscript for publication.
-
Competing interests LBM reports receiving grant funding from Forest Pharmaceuticals, and consulting for Bayer, Boehringer-Ingelheim, Boston Scientific, Medtronic, Merck and Pfizer. SBW reports receiving grant support from St. Jude Medical and Alberta Health Services. All other authors reported no relevant disclosures.
-
Ethics approval Conjoint Health Research Ethics Board, University of Calgary.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Anonymised patient-level data and statistical code will be made available upon reasonable request from the corresponding author. Informed consent for data sharing was not obtained but the presented data are anonymised and risk of identification is very low.