Article Text

Abstract
There have been few systematic efforts to define the burden of paediatric heart disease in India. Estimates based on published studies on congenital heart disease (CHD) at birth suggest a massive CHD burden. Absolute numbers of children with other heart diseases are also likely to be substantial. Given the enormity of the problem the number of paediatric heart programmes and specially trained paediatric cardiologists and paediatric cardiac surgeons are woefully inadequate. They are largely clustered in those parts of India that are experiencing improving economy and human development. For the average family the cost of care of a child with heart disease is prohibitive because care of children with heart disease often requires considerable human and material resources, together with sophisticated technology. While paediatric cardiology is only now being recognised in India as a major specialty, there is a need to intensify efforts to develop the specialty especially in those parts of India where there are very few centres. The present challenges are many and they include obtaining representative data on disease burden, establishing quality institutions with comprehensive paediatric cardiac programme training a cadre of professionals for paediatric heart care, developing cost-effective management strategies and improving awareness on diagnosis and management of paediatric heart diseases.
Statistics from Altmetric.com
The extraordinary geographical and cultural diversity of India was recognised as independent India was being established.1 One of the early challenges faced by the nation at the time of independence related to human development. The infant and maternal mortality rates were extremely high in the early 1950s for most of India.2 Since independence, selected states in India showed impressive improvement in various health indices, largely as a result of improving literacy, specifically female literacy.2 3 However, the track record for most of the Indian states in improving human development and health indices has been abysmal.4
In recent years selected areas of India are witnessing unprecedented economic growth, largely ushered in by the forces of globalisation. This has rapidly changed lifestyles, particularly in urban India.5 Globalisation has also had a “flattening effect” on India’s cultural diversity. India’s diversity today stems from sharp regional differences in economic growth and human development, in addition to previously existing differences in geography, language and religion. Large parts of rural India still have among the worst human development in the world, with extremely high infant and maternal mortality and alarming levels of malnutrition.4 As a result, it is perhaps impossible to make generalisations on health indices and disease prevalence in India.
These regional differences are likely to reflect on cardiovascular disease profiles in various parts of India. While most of India has witnessed an increase in lifestyle-related cardiovascular disease and diabetes, the problem appears particularly worrying in some areas.6 Rheumatic heart disease often mirrors human development and striking regional contrasts in disease trends can therefore be expected.7
Unlike acquired conditions, the prevalence and profile of congenital heart disease (CHD) at birth is unlikely to be significantly influenced by the above mentioned factors. However, the condition of healthcare delivery systems can significantly influence the early survival of newborns and infants with serious forms of CHD.8 This is turn can have an important effect on the profile of CHD encountered beyond infancy.
The rapid economic growth in the recent years has had a powerful impact on healthcare delivery in India. Tertiary health care has largely been taken over by the private sector. This sector has grown impressively in terms of revenue generated and number of hospitals and healthcare facilities.9 Comprehensive paediatric heart care that includes prenatal diagnosis, newborn and infant heart surgery and catheter interventions can only be provided in sophisticated tertiary hospitals. In the absence of health insurance the costs of paediatric heart operations and catheter interventions are prohibitive for most Indian families and only a small proportion of India’s population (mostly urban) can afford it. In this review we will focus on the current situation of paediatric cardiac diseases in India. The growth and development of services relating to paediatric heart care in India will also be discussed.
DEVELOPMENT OF PAEDIATRIC CARDIOLOGY AND PAEDIATRIC CARDIAC SURGERY
The first cardiac centres in India were established in the early 1960s. For the next 30 years, facilities for advanced heart care including cardiac surgery for both adults and children were essentially limited to very few large teaching institutions. These programmes trained a number of cardiologists and cardiac surgeons over a 30 year period. Training was simultaneously for both adult and paediatric heart care. All trainees, with very few exceptions, had their basic background in adult medicine. Paediatric cardiology therefore did not evolve as a subspecialty of paediatrics. Only a small handful of individuals seriously pursued paediatric cardiology and the number of dedicated paediatric cardiac surgeons in the country was limited to less than half a dozen.10 Pioneering and dedicated efforts from these individuals was responsible for the introduction of echocardiography, catheter interventions11 and infant heart surgery in India. However, because of the paucity of institutions willing to take care of children with heart disease, very little could be offered to Indian children with heart disease until recently.
In the 1990s a few dedicated paediatric heart programmes were established in the private sector in spite of serious questions about their economic viability. With the establishment these programmes and the formation of the Paediatric Cardiac Society of India in the late 1990s, paediatric cardiology and cardiac surgery are being recognised as separate specialties. Dedicated training programmes in paediatric cardiology have been created in these new programmes. Trainees from these programmes are in turn seeking to establish newer centres. The total number of infant and newborn congenital heart operations performed in all the existing Indian centres put together was less than 2500 in the year 2004. For a population of one billion, it can be expected that there would perhaps be approximately 100 000 newborns with congenital heart disease requiring some form of intervention during infancy. Thus, heart surgery appears realistic today for only 2–3% of infants requiring congenital heart surgery in India.12 13 This situation is likely to change with rapid changes in the economy and human development that we are now witnessing in many parts of India. It may be useful, therefore, to chart a roadmap for development of paediatric heart care for the country.
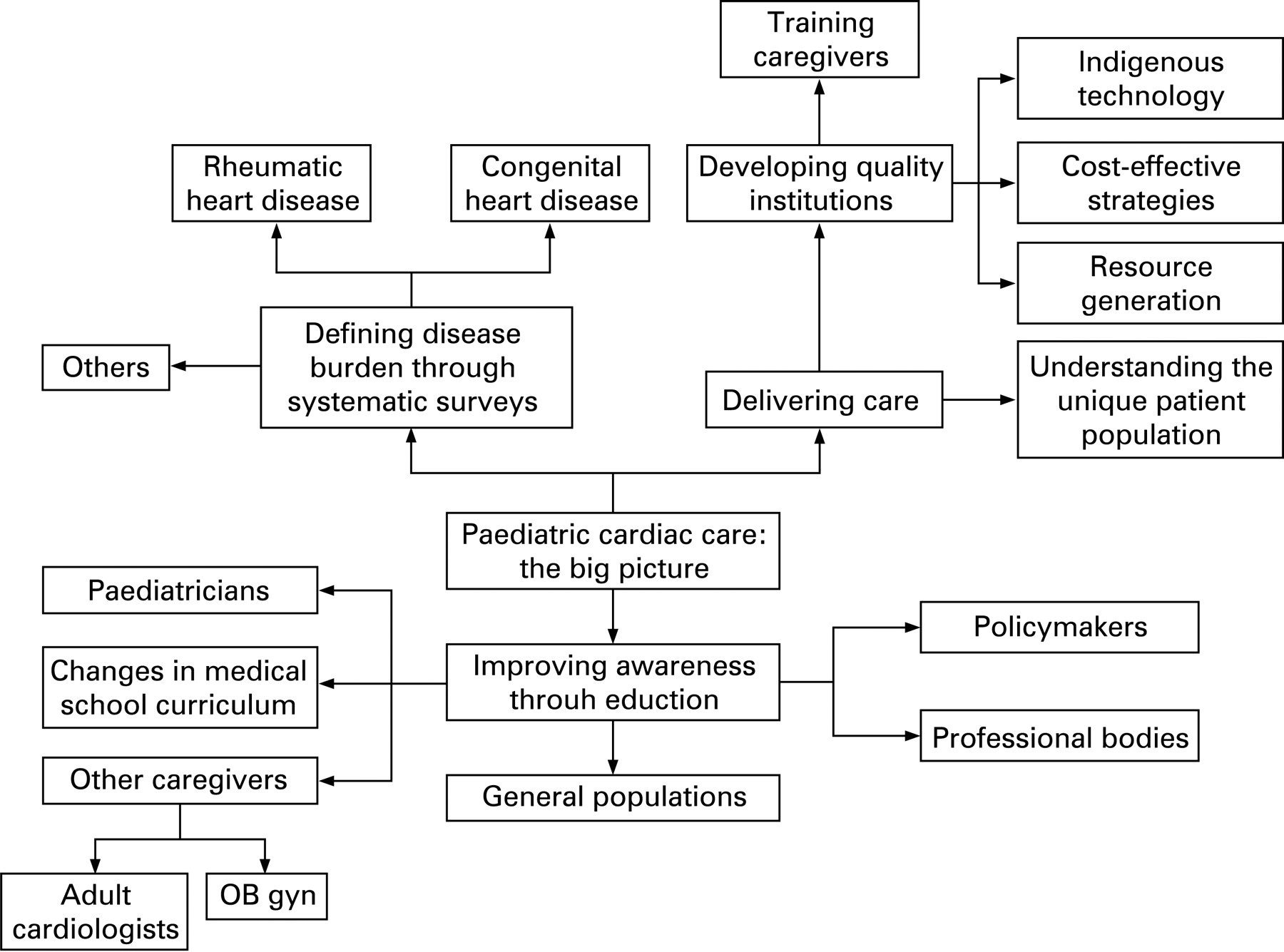
Figure 1 shows the various components of comprehensive paediatric heart care from a national perspective. This model can perhaps be applied to any specialty. This figure will form the basis of this section of the review and each of the headings will be discussed individually.
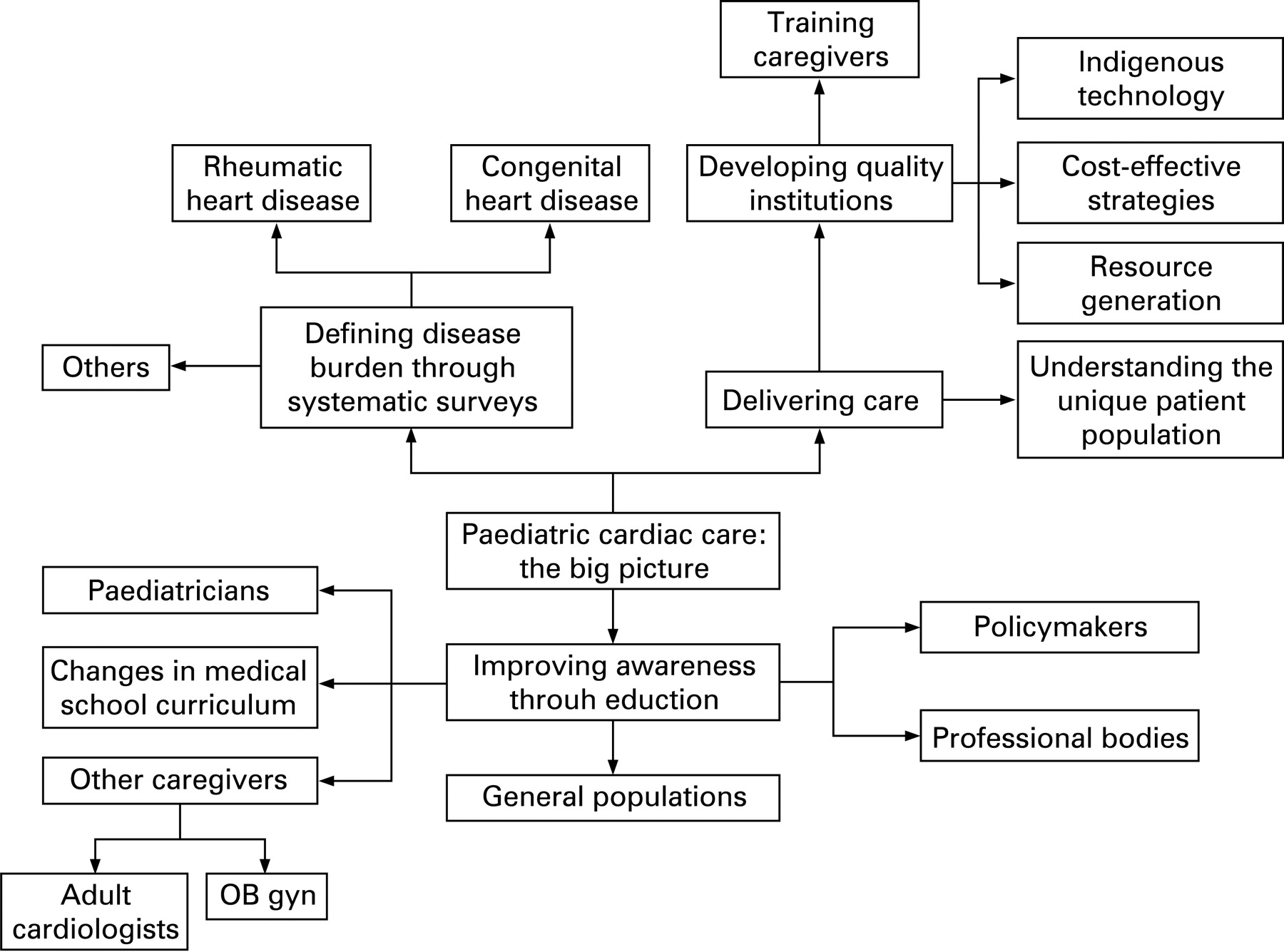
Defining disease burden
The major categories of paediatric heart disease from the standpoint of relative numbers can be classified under the following major categories:
-
Rheumatic heart disease
-
Congenital heart disease (CHD)
-
Lifestyle-related conditions—childhood obesity and hypertension
-
Other conditions—Kawasaki disease, cardiomyopathy and myocarditis.
No population-based systematic surveys on disease prevalence have been performed for CHD at birth. Although school surveys are available for CHD,14–16 they cannot be used to generate population-based prevalence data because of attrition in early years, low school enrolment rates in many parts of India and the possibility of children with CHD being absent from school because of illness. Similarly, published studies based on hospital statistics17 are also unlikely to be representative of the population. An ideal study that can generate reliable data for the population requires an organised infrastructure necessary for optimal care of newborns and infants with CHD (table 1).18 19 Such a situation does not exist even in the large metropolitan areas of India. Given the reasonable uniformity in CHD prevalence among various racial and ethnic groups in previous large population-based studies from various parts of the world,8 it may be fair to assume that the overall prevalence of CHD at birth may not be substantially different in India. There may, however, be differences in the relative prevalence of certain specific conditions and this may be worth investigating. It may, therefore, be appropriate to screen representative cohorts of live births in selected parts of India to obtain an idea of the typical profile of CHD in various parts of the country.
The epidemiology of rheumatic heart disease in India will be discussed separately. The information on other common acquired heart diseases is limited to small case reports and descriptive studies. Kawasaki disease (KD) is increasingly being recognised and a number of reports have appeared in recent years after initial descriptions in 1970s.20 21 Most reports are from urban populations and there is a strong possibility that a number of cases are missed.22 Awareness of manifestations of KD has not been formally evaluated and may be quite limited in many parts of India. There is a need to develop a comprehensive national disease registry for KD.23 Other forms of inflammatory vasculitis, such as aortoarteritis, are well recognised in Indian children. Several unique features characterise the disease in Indian children.24 25 They include a strong association with tuberculosis, occurrence of heart failure and myocardial dysfunction and involvement of the thoracic and abdominal aorta.
Few epidemiological data are currently available about myocarditis and cardiomyopathy in Indian children. Clinical features and diagnostic approaches for a child with suspected myocarditis are largely based on descriptions from studies published in Western literature and the disease has not been well characterised in Indian children.26 27
Changing lifestyles have started to have an impact in Indian children. This is particularly true for urban children. Surveys from selected cities have started to highlight the growing prevalence of obesity in Indian children.28–31 Evidence from prospective studies suggests that childhood obesity is directly related to the incidence of hypertension, type 2 diabetes and hypercholesterolaemia. According to the World Health Organization, chronic diseases are the major cause of death in almost all countries, including those in Asia. It is estimated that 70% of these deaths will happen in developing Asian nations like China, India, Pakistan, Cambodia and Vietnam.32 Cardiovascular diseases (CVD) are responsible for the major share of these chronic disease deaths. South Asians appear to have worse CVD risk profiles when compared to white populations with similar body mass index (BMI) levels. Small increases in BMI among them may translate into a substantial increase in the CVD burden.32 For this reason the trends reported in India are alarming even though the overall proportion of obesity and overweight children is lower than reported in other countries. The magnitude of the problem is already substantial and this is likely to rapidly increase in the near future. More studies are needed with representation from various regions. There is also an urgent need to develop normative data for BMI and other anthropometric indices, blood pressures and lipid profiles in Indian children.
Delivering paediatric heart care; developing quality institutions
Perhaps the most critical component of delivering paediatric heart care relates to development of quality institutions that should ideally become centres of excellence. Like many other technology and resource intensive subspecialties, the success of a paediatric cardiac programme is largely dependent on the creation of a cohesive team of individuals. This team is constituted by paediatric cardiologists, paediatric cardiac surgeons, anaesthesiologists, intensive care experts, nurses, technologists (catheterisation, perfusion, ultrasound) and other support personnel (fig 2). Additional closely related specialties include obstetrics and neonatology. A hugely challenging facet of delivering paediatric cardiac care in the developing world relates to establishment of new paediatric heart programmes. Because of the paucity of pre-existing training programmes, there is a tremendous shortage of trained staff in India. Additional challenges include costs of infrastructure and equipment and development of support services. Perhaps because of these reasons all existing paediatric heart programmes in India are in hospitals with busy adult cardiology and cardiac surgery programmes. The infrastructure, equipment and many of the personnel are completely shared with adult services. Paediatric heart programmes in India have not evolved in children’s hospitals, unlike many programmes in the West.

{kind=link}
{kind=link}
Paediatric heart care in India is currently being delivered in two settings. The first is a handful of large programmes with impressive case volumes. As of 2007 there are only half a dozen programmes in India with annual case volumes of more than 500 for paediatric heart surgery. The second setting is small centres, mostly private establishments, with small case volumes and limited personnel. The scope of comprehensive paediatric cardiac care, particularly newborn and infant heart surgery, is very limited in smaller centres. Most centres are clustered in large cities in selected regions in India. For large parts of the country there are no paediatric cardiac centres. The most poorly served regions include most eastern and all north-eastern states, vast regions in western and central India.10 12 13 The majority of children with CHD in these regions escape detection. For the small percentage of cases where the condition is diagnosed early enough for treatment, families are often intimidated by financial implications and the prospect of seeking care at a far-off centre. However, a small but growing number of families do travel large distances to obtain treatment in selected Indian centres that deliver comprehensive paediatric heart care. The larger and relatively less expensive programmes in India are often overwhelmed with numbers and have significant waiting lists. The low rate of detection of CHD, and economic and logistic considerations have perhaps ensured that only a tiny proportion of cases from the most poorly served regions reach these centres and keep the numbers to “manageable” levels.
A significant challenge relates to the prevailing mindset regarding the financial viability of paediatric heart programmes. Most private hospitals have been reluctant to establish these programmes because the costs of care are substantial and often cannot be recovered from patients. Open-heart operations for CHD typically cost $4000–$6000 (£2500–£3000) in most private Indian hospitals. Third-party payments are limited to situations where either parent is employed by selected organisations (mostly government) that provide comprehensive family health coverage. Most insurance companies exclude congenital heart defects from the list of conditions covered. Efforts to provide financial support for individual patients through donations from government funds are limited to selected patients in a few Indian states (such as Gujarat and Andhra Pradesh). This is not feasible on a larger scale. From a public health perspective, subsidies for expensive heart surgery or interventions would perhaps amount to significantly misplaced priorities and are not likely to be sustainable. Overseas agencies such as the Gift of Life programme of Rotary International (www.giftoflifeinternational.org) also fund paediatric heart operations in selected centres in a limited way. However, donations and logistic support for capacity building of selected centres in India may have a more lasting effect when compared to funding assistance for selected heart operations. The Children’s Heart Link (www.childrensheartlink.org) is an example of an organisation that is seeking to improve quality of paediatric heart care by facilitating collaborations between established centres in North America and new programmes in the developing world.
Another challenge relates to quality of care. The outcomes after paediatric cardiac surgery in infants and newborns are critically dependent on the skills and cohesiveness of the individual team members and there is a fairly steep learning curve for the institution.33 Newly established programmes therefore often need to have careful case selection policies in the beginning. Careful prioritisation of care is often necessary in the face of large numbers and limited resources. Most Indian centres do not therefore routinely perform the Norwood operation for hypoplastic left heart syndrome. Lesions that can be corrected through a single operation often receive greater priority over multistaged palliative procedures. Nosocomial infections are a significant cause of mortality in this particularly vulnerable group of patients and it is essential to establish a robust infection control programme as new programmes are being established.32
When compared to established programmes in developed nations, there are noticeable differences in how paediatric heart programmes are structured in India. Most paediatric cardiologists are forced to multitask and do not focus on specific areas with in the specialty. For example, a paediatric cardiologist could perform echocardiography, catheter interventions procedures and look after intensive care. Dedicated services for specific areas such as adult congenital heart disease, fetal cardiology and paediatric electrophysiology have not been developed in Indian centres.
Role of institutions
Training
Apart from delivering care, institutions serve a number of other vital purposes. Training of staff in all the facets of paediatric heart care is largely possible only in busy institutions. Small programmes with low case volumes cannot develop robust training programmes. Until recently, training was largely limited to a small number of institutions in India. There were no formal structured programmes exclusively for paediatric cardiology. Paediatric cardiology had to be learned as a part of training in adult cardiology. After completion of training very few saw opportunities to practise paediatric cardiology; besides, most trainees did not have a basic background in general paediatrics. As a result in the mid-1990s the total number of dedicated paediatric cardiologists in all of India was less than a dozen. A beginning was made recently with the establishment of a structured training programme in paediatric cardiology by the national board in four of the existing large paediatric heart programmes in the country. The numbers of trainees emerging from these programmes are grossly inadequate for the country’s needs. The situation is far worse for paediatric cardiac surgery; there are no dedicated training programmes yet. As a result there is a great shortage of paediatric cardiac surgeons. The shortfall is likely to continue for many years and existing centres may find it particularly difficult to deal with growing case numbers.
Developing specific strategies for Indian patients
Because of great differences in the CHD patient populations that are typically encountered in India, specific management approaches often need to be developed for Indian patients (table 2). The differences relate to older age at presentation for many of the congenital heart defects, high prevalence of malnutrition and associated infections. Economic considerations (below) also impact treatment practices significantly. A number of important publications, mostly from selected Indian institutions with paediatric heart programmes, highlight the unique problems encountered in India and suggest solutions to deal with them.33–45
Cost-effective practices
Because of severe cost constraints typically encountered in most Indian institutions, a number of cost-effective practices have evolved in India.46–53 These relate to management strategies for individual conditions, institutional policies for catheter interventions and for cardiac surgery, as well as development of specific operations and catheter-based procedures46 (tables 3 and 4). Some of the less expensive management strategies practised for patients with CHD may not be perceived as ideal and their long-term outcomes are likely to be less acceptable than those that conform to the standards of care in developed nations. A good example relates to patients requiring the use of conduits for congenital heart surgery. Conduits are very expensive in all but one or two programmes in India that have a homograft bank. More importantly, conduits need regular replacement and the prospect of repeated open-heart operations is completely unrealistic for a number of patients and their families. As a result, many Indian programmes attempt to postpone the implantation of conduits through palliative procedures such as aorto-pulmonary shunt and the Glen shunt.
Indigenous technology
Cardiology and cardiac surgery have been largely dependent on and driven by imported technology. Because of the paucity of institutions that focus on medical technology development, there have been very few Indian innovations in cardiology and cardiac surgery. The success of the TTK Chitra heart valve underscores the feasibility and scope of innovative technological solutions developed in India.54 55 This valve is a tilting disc artificial heart valve prosthesis designed and developed by Sree Chitra Tirunal Institute for Medical Sciences and Technology, (SCTIMST), an autonomous institute under the Department of Science and Technology, Government of India. TTK Chitra heart valves are being used in over 175 major cardiac programmes in the country. More than 15 000 valves have been implanted since its first implant on 6 December 1990 (www.sctimst.ac.in/bmt/technologies3). Additional innovations in cardiovascular technology that have found applications include the bubble oxygenator and cardiotomy reservoir (SCTIMST) and the permanent pacemaker (Shree Pacetronics; www.pacetronix.com/clinic) and indigenously processed porcine xenograft conduits (www.frontierlifeline.com, www.biotech.iitm.ac.in).
IMPROVING AWARENESS REGARDING PAEDIATRIC HEART DISEASES
A number of problems relating to inadequate healthcare delivery for children with congenital heart disease are the result of poor awareness among care givers (table 5). This is particularly true for many paediatricians in India. Most postgraduate training programmes in India are in regions with no paediatric heart programmes. As a result the average postgraduate trainee in general paediatrics receives little exposure in paediatric cardiology.10 This translates into a situation where most children with heart disease escape early detection. There is, therefore, an urgent need to educate practising paediatricians through current medical education programmes. Professional bodies such as the Indian Academy of Paediatrics can help facilitate this process. The newly formulated Paediatric Cardiac Society of India (PCSI) has defined education of paediatricians as one of its most important goals. The PCSI is working earnestly in educating paediatricians, postgraduate students in paediatrics through regular continuing medical education programmes, newsletters and annual conferences. There is also a need to include structured training in paediatric cardiology in the curriculum of postgraduate training in Indian institutions. Wherever possible, rotations should be organised in institutions with paediatric heart programmes. It is also perhaps necessary to educate caregivers in closely related specialties. Adult cardiologists often have to care for children with heart disease in many Indian hospitals. Although some of them are familiar with common congenital heart defects, they typically do not have any exposure to a structured paediatric cardiac programme and are unable to handle small infants and newborns. Obstetricians-gynaecologists and radiologists have to be familiarised with basic ultrasound screening for fetal heart defects.
CONCLUSIONS
Notwithstanding the accomplishments in recent years it is perhaps fair to state that paediatric heart care in India is still rudimentary. Given the significant burden of readily treatable conditions, such as diarrhoea and respiratory conditions, congenital heart disease is not yet a paediatric health priority from a national perspective. There is a need for evolving a mechanism to determine disease burden for major categories of paediatric heart diseases in India. There is an urgent need to develop quality institutions for delivering care, training professionals, driving research and developing specific strategies that would be realistic in the Indian context. There is also a need to intensify efforts to educate general paediatricians and other health professionals who encounter children with heart disease. With improving human development and economic progress the demand for quality paediatric heart care is likely to grow exponentially in India. However, the challenge of delivering quality care at a cost that is affordable to the majority of affected families is likely to remain for a very long time.
REFERENCES
Footnotes
-
Competing interests: None.