Article Text

Abstract
The authors illustrate the successful ablation of a left-sided posterior accessory pathway via a retrograde aortic approach in a patient with coronary ostial atresia associated with persistent left-sided superior vena cava. This is an extremely rare anomaly which should be considered by cardiac electrophysiologists when there is difficulty cannulating the coronary sinus via the right atrial route. Awareness of this route obviates the need for additional venous access.
- ARRHYTHMIAS
- CONGENITAL HEART DISEASE
Statistics from Altmetric.com
Case report
A 22-year-old man with no past medical history presented with frequent palpitations. A 12-lead resting ECG showed supraventricular tachycardia that correlated with his symptoms. Transthoracic echocardiogram revealed normal ejection fraction with no structural abnormality.
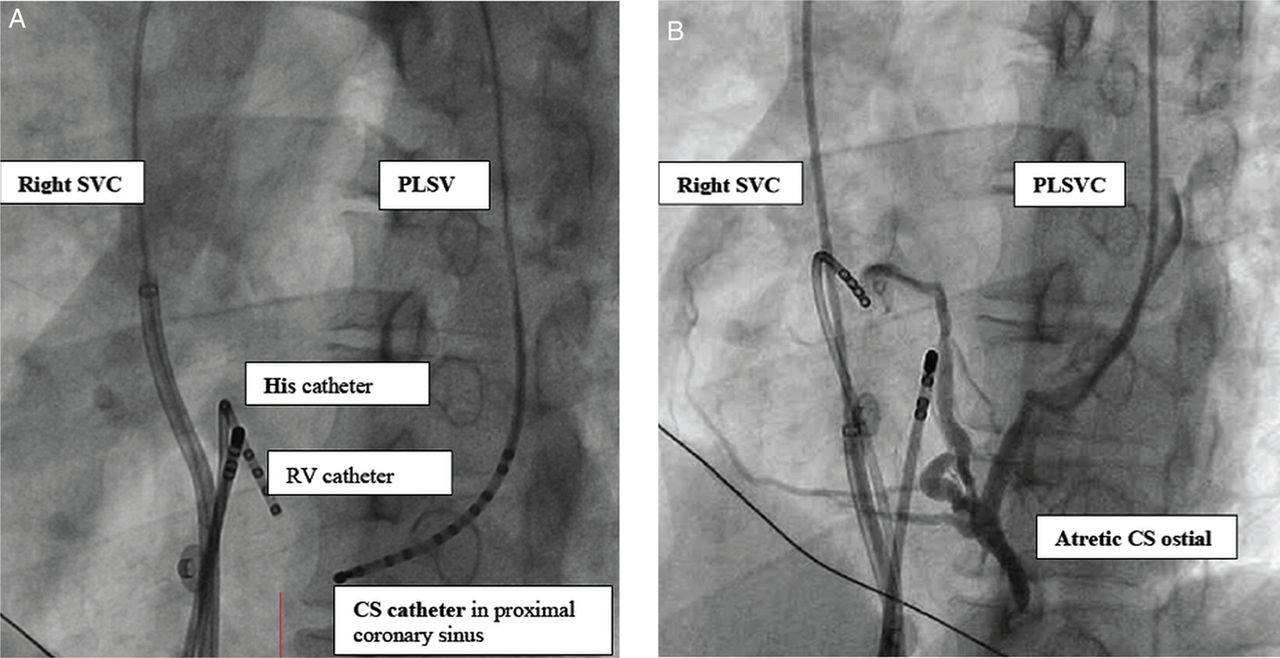
He underwent an invasive cardiac electrophysiology (EP) study. Via the right femoral vein, the authors were unable to cannulate the coronary sinus (CS) with a deflectable decapolar catheter. Multiple attempts at locating the CS os with contrast injection through a Swartz Guiding sheath (SL2, St Jude Medical) were also unsuccessful. The possibility of CS ostial atresia which is usually accompanied by a persistent left superior vena cava (PLSVC) was considered. In this patient, the authors managed to advance the deflectable decapolar catheter from the right atrium to the right-sided SVC, across the innominate vein, inferiorly to the left-sided SVC and successfully position it within the CS with its distal electrode at the proximal CS (figure 1A).
{kind=link}
(A) (left): Left anterior oblique (LAO) 45° view: Successful placement of a deflectable decapolar catheter within the coronary sinus (CS) by advancing from the right atrium to the right superior vena cava (SVC) across the innominate vein into the persistent left SVC (PLSVC) in the patient. (B) (right): LAO 45° view: Venogram demonstrating venous drainage via the PLSVC, and the atresia of CS ostium. RV, right ventricle.
EP study was performed with induction of orthodromic reciprocating tachycardia involving a concealed left-sided lateral accessory pathway. This was successfully ablated via a retrograde aortic approach, aided by the CS catheter electrograms. Post ablation, a selective venogram (figure 1B) confirmed the presence of a PLSVC with CS ostial atresia.
CS ostial atresia associated with PLSVC is an extremely rare anomaly1–3 which should be considered by cardiac electrophysiologists when there is difficulty cannulating the CS via the right atrial route despite multiple attempts and with various long sheaths. The presence of retrograde flow from the CS to the left superior vena cava, and via the innominate vein to the right superior vena cava1 allows us to successfully place a decapolar catheter within the CS. This step is crucial in performing an EP study and guiding ablation of left-sided accessory pathways. Awareness of the possibility of this route obviates the need to obtain additional venous access via the left subclavian or the internal jugular veins.
Footnotes
-
Contributors CTN: involved in the conceptualisation and drafting of the manuscript. CWL: involved in the conceptualisation, drafting and review of the manuscript. JS: involved in the review of the manuscript. C-KC: involved in the conceptualisation and review of the manuscript.
-
Competing interests None.
-
Patient consent Not obtained.
-
Provenance and peer review Not commissioned; internally peer reviewed.