Article Text

Abstract
Objectives Although previous studies have suggested alarming rise in the prevalence of hypertension in Nepal, there is dearth of information on its awareness, treatment and control. In this cross-sectional study, we assessed awareness, treatment and control of hypertension among 298 hypertensive adults from the suburban town of Dhulikhel, Nepal.
Methods This cross-sectional study is based on Dhulikhel Heart Study, which included 1073 adults, aged ≥18 years, recruited from randomly selected households. Comprehensive health interviews and blood pressure measurements were completed during home interviews. Hypertensives (systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg or receiving antihypertensive medication) were further evaluated for awareness, treatment and control of hypertension. Multivariate regression model quantified the association of the sociodemographic characteristics and the cardiovascular disease (CVD) risk factors with hypertension awareness. Differences between sociodemographic characteristics and CVD risk factors with treatment and control of hypertension were tested using χ2 tests.
Results A total of 43.6% of all hypertensives (n=298) were aware of their hypertension status. In multivariate analyses, hypertension awareness was associated with increasing age (p<0.001). More than three-fourth (76.1%) of those who were aware of their hypertension status (n=130) were currently on treatment. There were significant differences in treatment status by sex, occupation, age, income quartiles and body mass index. Only 35.3% of those on treatment (n=99) had blood pressure control.
Conclusions The levels of awareness, treatment and control of hypertension in this sample of Nepalese adults were low.
- HYPERTENSION
Statistics from Altmetric.com
Background
Hypertension was the leading risk factor for global disease burden in 2010, accounting for 7.0% of global disability-adjusted life years (DALYs);1 and ranks among the most important risk factors for cardiovascular disease (CVD), contributing to 45% of global CVD morbidity and mortality. Globally, approximately two-thirds of stroke, one-half of ischemic heart disease (IHD) and approximately three-quarters of hypertensive disease were attributable to non-optimal blood pressure in the year 2000 and approximately two-thirds of the burden of disease occurred in the developing world.2
Unfortunately, hypertension remains a hidden condition for many affected people and is poorly managed among the known patients. In a multi-country study, only 47% of the hypertensive patients were aware of the diagnosis. Of those who were aware, 86% were under treatment but only 33% of those receiving treatment were controlled.3 Awareness, treatment and control of hypertension were higher in high-income countries compared with the low-income countries. Even within a country, the awareness, treatment and control were lower in the rural communities compared with the urban, especially in the low-income countries.3 ,4 A national representative survey from Nepal reported that almost 90% of the diagnosed hypertension were not treated.5
It is also important to understand the factors associated with hypertension awareness, treatment and control to develop evidence-based strategies. Among the aware hypertensives, treatment was more common among less educated, who lived in urban areas, have low socioeconomic status and had a family history.6–8 A study from the USA reported that the awareness of hypertension differed greatly by neighbourhoods and ethnicity.9 Despite the report of high prevalence and poor management of hypertension, there is dearth of information on the correlates of hypertension awareness, treatment and control in Nepal. This gap in knowledge is an impediment to develop targeted strategies for the prevention and management of hypertension.
The present study used the baseline data of the Dhulikhel Heart Study (DHS),10 a population-based longitudinal study focusing on CVD risk factors in a suburban town in central Nepal. The objective of the study is to determine the level of awareness, treatment and control of hypertension and their associated factors in a suburban population of urban Nepal.
Methods and materials
Study design and participants
The DHS was launched in November 2013 to gain an in-depth understanding of the epidemiology of CVD and associated risk factors among all adult residents (18 years and older), in the town of Dhulikhel in central Nepal. The first wave of the DHS baseline survey was conducted between November 2013 and February 2015 and recruited 1073 participants from a third of randomly selected households. The participants included the residents (living in Dhulikhel for at least past 6 months) who were 18 years or older at the time of data collection from the sampled households. We excluded pregnant women, individuals in institutionalised settings (living in hostels, motels) and those who were unable to communicate due to physical or mental problems.
This study analysed the data of 298 hypertensive patients identified during the first wave of DHS baseline survey. This study was approved by the Dhulikhel Hospital Institutional Review Board and was provided exemption by the University of Washington Human Subjects Division.
Hypertension assessment
Blood pressure was measured three times in a sitting posture on the right arm over loose clothes using a standard digital blood pressure machine (Microlife, Switzerland). The mean of the three measurements was used for the analysis. Hypertension was defined as a systolic blood pressure (SBP) of ≥140 mm Hg or a diastolic blood pressure (DBP) of ≥90 mm Hg or those who were receiving antihypertensive medication.11
Hypertension awareness
The participants were considered to be aware of their hypertension status if they reported that a doctor or other health worker had told them that they had hypertension or high blood pressure.
Hypertension treatment
Any participant who self-reported taking medicines for lowering blood pressure was considered as ‘treated’.
Control of blood pressure: Participants who were on antihypertensive treatment and had SBP <140 mm Hg and DBP <90 mm Hg were categorised as having blood pressure controlled.
Assessment of other variables
The study staff administered a structured questionnaire using an electronic tablet. The questionnaire included information on sociodemographic characteristics (age, sex, marital status, occupation, ethnicity, education, income) and lifestyle (smoking, alcohol, physical activity, fruits and vegetable consumption). Body weight and height were measured using standard procedures. Body mass index (BMI) of the participants was calculated as weight in kilogram per square of height in metre and categorised as (1) obesity (≥30.0 kg/m2), (2) overweight (25.0–25.9 kg/m2), (3) normal (18.5–24.9 kg/m2) or (4) underweight (<18.5 kg/m2).12 Smoking and alcohol consumption was ascertained using the questions based on the WHO STEPS survey questionnaire.13 Physical activity was assessed using the Global Physical Activity Questionnaire.14 The activity level of 600 metabolic equivalent minutes per week was categorised as having adequate physical activity as per the WHO recommendation.15 Fruits and vegetable consumption was collected using a validated food frequency questionnaire.16 WHO recommendation of at least five servings of fruits and vegetables per day was considered adequate.17 In addition we also determined the adherence to antihypertensive medications using Morisky's Medication Adherence Scale-8.18–20
Statistical methods
Sample characteristics were described for hypertensive and non-hypertensives using means and SDs for continuous variables and percentages for categorical variables. We quantified the independent associations of hypertension awareness with sociodemographic characteristics (sex, age, marital status, occupation, ethnicity, education, income) and CVD risk factors (BMI, smoking, physical activity, fruits and vegetable consumption, alcohol) using multivariate logistic regression with generalised estimating equation. The association of hypertension awareness with sociodemographic variables were adjusted with the remaining sociodemographic variables.
The bivariate association of hypertension treatment and control with sociodemographic and CVD risk factors were examined using χ2 test and independent t-test. The multivariate model was not conducted due to small sample size.
Results
Characteristics of the DHS participants
Table 1 shows the sociodemographic characteristics of the DHS participants by gender. Majority of the participants were women (58.4%) and belonged to Newar ethnic group. There were significant gender differences in terms of marital status, income and education.
Characteristics of the Dhulikhel Heart Study participants (n=1073)
Table 2 shows the sociodemographic characteristics and CVD risk factors of the hypertensive participants of DHS by gender. The mean age was 50.6 years (SD: 15 years). Hypertension was more prevalent among men. There were also significant differences in occupation, educational status and income between male and female hypertensives, which might in fact reflect the inherent differences on these parameters in the whole community (irrespective of their hypertension status) (table 1). The risk factors like smoking and high alcohol consumption were more common among hypertensive men, whereas overweight, obesity and low consumption of fruits were more common among women.
Sociodemographic characteristics and CVD risk factors of the hypertensive participants of the Dhulikhel Heart Study (n=298)
Factors associated with hypertension awareness
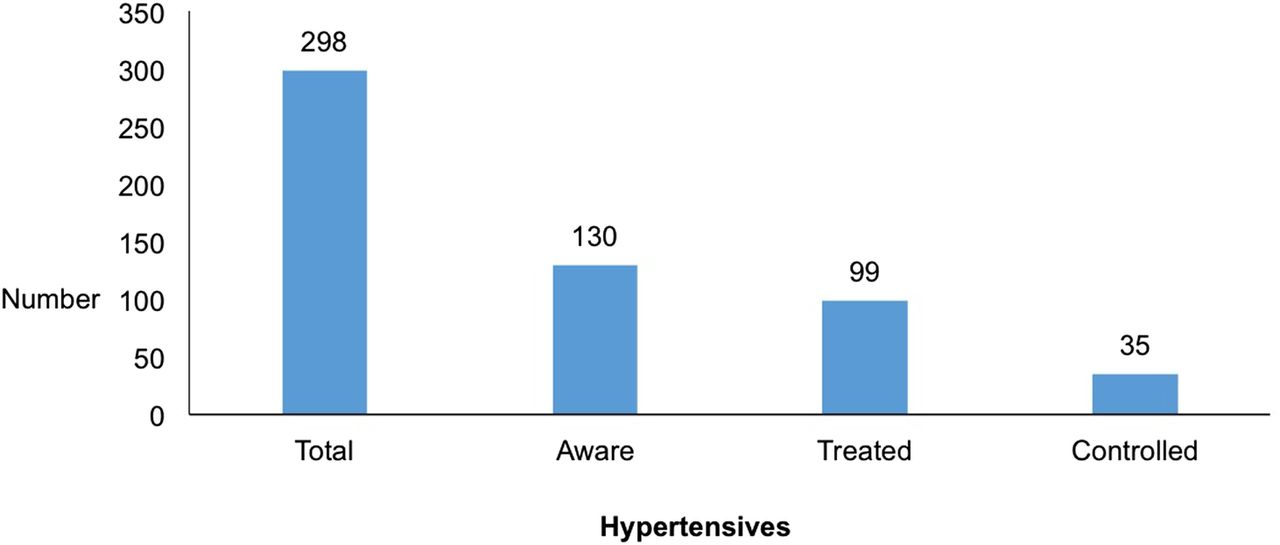
Only 44% of the hypertensive participants were aware of their condition (figure 1 Awareness, treatment and control of hypertensives in a suburban Nepalese population, n=298). In multivariate model, age was positively associated with being aware of hypertension status (p<0.001). One year higher age was associated with 5% higher odds of being aware (OR: 1.05 95% CI 1.02 to 1.07). Men were less likely to be aware compared with women. However, the association was not statistically significant (table 3).

{kind=link}
Bar graph showing the awareness, treatment and control of hypertensives in a suburban Nepalese population (n=298).
Multivariate logistic regression analyses (using generalised estimating equation) of sociodemographic factors with hypertension awareness (n=298)
Hypertension treatment status
A total of 76% of all aware hypertensives were on antihypertensive treatment. Participants on treatment were on an average 7 years older compared with non-treated (p<0.001). Being on treatment was also positively associated with being female, unemployed, poor (in lowest wealth quintile) and being obese (p<0.05) (table 4).
Sociodemographic characteristics of the Dhulikhel Heart Study participants by hypertension treatment status (n=130)
Hypertension control status
Only 35.3% of hypertensives on treatment had blood pressure control (SBP <140 mm Hg and DBP <90 mm Hg). Having normal weight and being non-smoker or former smoker was significantly associated with blood pressure control (p<0.05). Higher medicine adherence was associated with blood pressure control, although the association was not statistically significant (table 5).
Sociodemographic characteristics, CVD risk factors and adherence to antihypertensive medications of the Dhulikhel Heart Study participants by hypertension control status (n=99)
Summary of hypertension awareness, treatment and control
Table 6 summarises the awareness, treatment and control of hypertension in this study (against all hypertensives) by key sociodemographic characteristics. Only a third of all hypertensives were under treatment and a mere 11.7% had their blood pressure properly controlled.
Summary of awareness, treatment and control of hypertension among Dhulikhel Heart Study participants
Discussion
This is one of the first studies to provide an in-depth insight into awareness, treatment and control of hypertension among suburban Nepalese adult population.
Awareness of hypertension
We found that less than half (44%) of the participants were aware of their hypertension status. This is consistent with other studies from Nepal and other low/middle-income countries.3 ,4 ,21
Our study compares well with a multicentre study from neighbouring countries India and Bangladesh in which, among 777 elderly hypertensives from urban and rural sites, 44.7% were found to be aware. The awareness level in our study is also remarkably higher compared with other studies from Nepal and India.22 ,23 It is difficult to infer these differences to specific reasons. However, it is likely that the presence of a major community-based hospital (Dhulikhel Hospital) in the vicinity with a large number of employees from local community might have influenced it. Future studies should investigate these differences in similar population and should aim to learn from some of the best practices that account for increased level of awareness.
Higher level of awareness in older adult Nepalese also concur with other studies.6 ,24 It is likely that the older age groups might have come in contact with health systems more often, leading to greater probability of being aware of their hypertension status. Although not statistically significant, more women than men were aware of their status in our study, which corresponds to most other studies.24 ,25 In a systematic review of hypertension awareness, treatment and control in Africa, most studies reported better awareness among women.25 Women have more contact with the health system due to maternal and child health-related issues, which is likely the reason for their better awareness about their health in general.26 ,27
Our findings also suggest that there might be ethnic differences in the awareness of hypertension in Nepalese community. The Brahmins and Newars, which are historically more well-off and educated ethnic groups, seem to have higher levels of awareness. However, further studies are required to explore the ethnic attributes that affect awareness to health conditions and health behaviours. The lack of a positive association between education and hypertension awareness in our study is in contrast to previous studies. Results from high income countries as well as low and middle income countries have shown that higher-level education has a direct relationship with hypertension awareness.28–30 As most of the elderly were uneducated in our study, it is likely there was residual confounding by age.
Treatment and control of hypertension
The treatment rates in this study (76.1% of all known hypertensives) are comparable with the findings in a multi-country study, which reported that 77.7% of the aware hypertensive participants were on treatment in low-income countries.3 The average proportion of hypertensives on treatment was 75% in another systematic review that included multiple low-income countries.31 Our finding also corresponds to a study from rural Kerala in India in which about 80.5% of known hypertensives were on treatment.32 However, it is lower than a multi-country study (India and Bangladesh) in which 88.7% of known hypertensives were under treatment.9 Our finding is, however, remarkably higher than similar other study in Nepal in which only 46.6% of known hypertensives were on antihypertensive medication.21 These differences might be accounted to a relatively easier and affordable access to treatment for our study population due to the presence of a community-based hospital (Dhulikhel Hospital) in the vicinity. However, it should be noted that despite being so close to an affordable healthcare system, about a quarter of the known hypertensives in our study were not on treatment. The allopathic medications are viewed sceptically, especially when required to be taken for a long time.
The positive association of being on treatment with female gender is consistent with other studies that show women are better than men at healthcare utilisation.33 ,34 The fact that men are at higher risk of hypertension and are less likely to be aware and treated compared with women has important public health implications. Health education and screening programme that have more emphasis to target men need to be warranted in communities. The association of lower socioeconomic status to being treated in our study contradicts with earlier studies.3 Whereas we cannot rule out the possibilities of type 1 error, future studies should definitely explore in-depth relationships between socioeconomic status and hypertension treatment in this population.
Only about a third (35.3%) of those on antihypertensive treatment in our study had their blood pressure controlled. This is consistent with most of the findings from other studies. Only 32% of the treated participants had their blood pressure controlled in a systematic review of studies from both developed and low/middle-income countries.31 Our finding is also remarkably similar to the finding from the five cities study from India in which only about a third of those on hypertension treatment had their blood pressure controlled.23 In another study from suburban population in Nepal, 36% of those on antihypertensive treatment had proper control of blood pressure.21
It is concerning that despite the availability of low-cost drugs for hypertension management, the treatment and overall control rates are not satisfactory. Treatment efforts might be hindered by patients' low perceived risks of hypertension, low health literacy, lack of motivation and medication costs in low resource settings.35 In addition, Nepal does not have a clear national plan and strategy for hypertension prevention and management.36 ,37 Lack of clear guidelines regarding medication use and low medication adherence are also barriers to the proper management of hypertension.35
Significant association of high BMI and smoking status with uncontrolled blood pressure in our study suggests the urgent need for a comprehensive and culturally tailored approach to chronic disease management.38–40
Only about a third of the participants taking medications were highly adherent in our study. It is concerning because poor adherence to therapy is estimated to contribute to uncontrolled blood pressure in more than two-thirds of people living with hypertension.41 Although not statistically significant, our study suggests that higher adherence to antihypertensive is associated with better blood pressure control.
Strengths and limitations
To our knowledge, this is one of the first studies from Nepal to explore the whole spectrum of awareness, treatment and control of hypertension. Vaidya et al had done a similar study in 2004–2005 in a suburban town in Eastern Nepal and had reported higher level of awareness (58%) and control (34% of all hypertensives), thus affirming that the ‘rule of halves’ still applied for hypertension in Nepalese setting. However, the study recruited only male participants and the lowest cut-off for age was 35 years. It also did not describe the proportion on treatment.4 The design of our study relates closely with the study by Sharma et al21 which reported similar awareness (41%) and control rates (35.7% of all on treatment). However, the study did not describe the associated factors. Thus, our study provides newer insights into this topic in Nepalese population and helps address some of the limitations of earlier studies. The random sampling technique, standardised measurements and extensive information on possible confounders are the major strengths of this study in identifying factors associated with hypertension awareness.
Our study has several limitations. As in any cross-sectional study, we were not able to determine causal associations. Although this is one of largest studies on this topic from Nepal, we acknowledge that the sample size was still small and was not sufficiently powered to detect associations of low magnitude. We also did not have adequate sample size to perform multivariate logistic regression for factors associated with hypertension treatment and control. Hence, the present results may have been confounded by sociodemographic variables. We will report results with larger sample size as we continue to expand the remaining baseline data collection of DHS in subsequent waves.
We measured blood pressure at home, and not in a clinical setting, which may have prevented anxiety and thus false high readings. However, the single day blood pressure measurement might have over-diagnosed and thus increased the proportion of unaware, untreated and uncontrolled hypertension. Since most of the population-based studies employ a single day measurement due to logistic challenges, we believe that this should not be a major concern unique to our study only. This study is also not representative of Nepal due to the high ethnic, dietary and geographical variation in the country. In addition, Dhulikhel is a small town with a large tertiary-level health service provider (Dhulikhel Hospital) that employs almost 300 staffs from the locality. This might have led to better awareness, treatment and control compared with the general population of similar sociodemographic levels in other settings.
Conclusion
By providing important insights into the awareness, treatment and control of hypertension in this suburban Nepalese population, this study reaffirms the urgency of hypertension prevention and management and highlights that increasing awareness of hypertension may be a major ‘low-hanging fruit’ in terms of hypertension management in low/middle-income countries.
Key messages
What is already known about this subject?
Several epidemiological studies have reported that the awareness, treatment and control of hypertension are low in low-income settings.
What does this study add?
Our results suggest that awareness, treatment and control of hypertension, including the adherence to antihypertensive medications are low in suburban Nepalese as well. Increasing the awareness level of hypertension may be the low-hanging fruit in terms of population-based approach to hypertension management.
How might this impact on clinical practice?
The findings of the study can be used for developing strategies for addressing the problem of hypertension in low-income settings.
Acknowledgments
BMK and NS were supported by the Laughlin family.
References
Footnotes
Contributors BMK conceived the study. BMK, RPK, ALF, AS and JPL elaborated the study design, developed the protocol and the data collection tool. AS and ALF trained the data collectors. RPK oversaw the data collection in the field. KCGC and AM provided inputs in the data analysis. NS helped improvise the manuscript. All authors contributed to refinement and approved the final manuscript.
Funding NS is supported by the endowed fund from Laughlin family.
Competing interests None declared.
Ethics approval Dhulikhel Hospital Institutional Review Committee, University of Washington Human Subjects Division.
Provenance and peer review Not commissioned; externally peer reviewed.