Article Text

Abstract
Recent developments in magnetic resonance imaging have focused attention on evaluation of patients with cardiac disease. These improvements have been substantiated by a large and expanding body of clinical evidence, making cardiovascular magnetic resonance the imaging modality of choice in a wide variety of cardiovascular disorders. A brief review on the current applications of cardiovascular magnetic resonance is provided, with reference to some of the most relevant studies, statements and reviews published in this field.
Statistics from Altmetric.com
Cardiovascular magnetic resonance (CMR) currently provides a comprehensive evaluation of the heart. Multiplanar imaging and excellent spatial resolution give extensive information on both anatomy and function. Precise quantification of flow is possible, and this is important in valvular and congenital heart disease. Importantly, CMR allows characterisation of the myocardium in vivo, avoiding the sampling error and invasive risks of myocardial biopsy. Thus, fat, iron or water accumulation suggesting inflammation can be identified and quantified. The additional use of gadolinium contrast agents detects areas of infarction, fibrosis, or infiltration by extracellular materials. Gadolinium contrast agents can also be used successfully in myocardial perfusion studies for assessment of ischaemia and in central and peripheral angiograms.
Like echocardiography, CMR is a safe technique with no proven detrimental effects on the long term, as opposed to other x-ray-based techniques such as x ray angiography, computed tomography (CT), and single-photon emission computed tomography (SPECT), where radiation exposure is a key concern. This is an important issue when multimultimodality or serial imaging is considered, especially in the young and female population.
Volumes, function and mass
Estimation of myocardial volumes and mass is accurate and has been validated against postmortem studies. Reproducibility is superior to the other imaging techniques, and so CMR is considered to be the gold standard in volumes and mass assessment.1
Evaluation of ventricular volumes and ejection fraction has major implications for diagnosis, prognosis and management of cardiac conditions. Thus, CMR can provide valuable information on ventricular volumes and ejection fraction when other studies are conflicting or inconclusive. In addition, changes over time are more robustly detected, and clinical decisions can be taken more confidently.
The intrinsic low variability is also a considerable advantage in research, where smaller sample sizes can be used to achieve statistical significance, saving time on recruitment and reducing costs accordingly.
Coronary artery disease
Coronary artery disease (CAD) is the commonest cardiac pathology. CMR has an established role in the evaluation of ischaemia, infarction and viability; can detect myocardial infarction complications such as right ventricular extension and ventricular thrombi; and can differentiate aneurysms from pseudoaneurysms. However, CMR coronary angiography is not recommended in the evaluation of coronary artery stenosis, and its role is limited to diagnosis of congenital coronary anomalies.
Ischaemia-stress CMR
Dobutamine stress CMR is well established for identifying ischaemia-induced wall motion abnormalities in CAD. Diagnostic results are excellent and superior to dobutamine stress echocardiography (accuracy 86.0% vs 72.7%, p<0.005),2 rendering an attractive alternative when echocardiographic image quality is poor.
Prognostic information can also be generated, as a positive study is predictive of adverse events (cumulative event rate of 18.8% at 3 years for a positive test vs 3.3% for a negative test).3 Therefore, this technique is suitable for risk stratification.
Ischaemia-perfusion CMR
First-pass myocardial perfusion is now the most popular CMR method for evaluating myocardial ischaemia, with good results in comparison with SPECT and positron emission tomography (PET). In a recent multicentre randomised trial, there was superiority of perfusion CMR over SPECT for diagnosing CAD (area under the ROC curve for CMR of 0.86 (SD 0.06) vs SPECT 0.67 (0.5), p=0.013).4
Perfusion CMR also provides prognostic information, where a positive test has been shown to predict adverse outcomes (cumulative event rate of 16.3% at 3 years vs 2.3% when the test was negative).3 This is similar to SPECT for risk assessment.
A potential application of perfusion CMR is in the evaluation of patients presenting to the emergency department with chest pain. In this setting, a negative perfusion study can rule out significant CAD or future cardiac events with high sensitivity and specificity.5
Infarction and viability
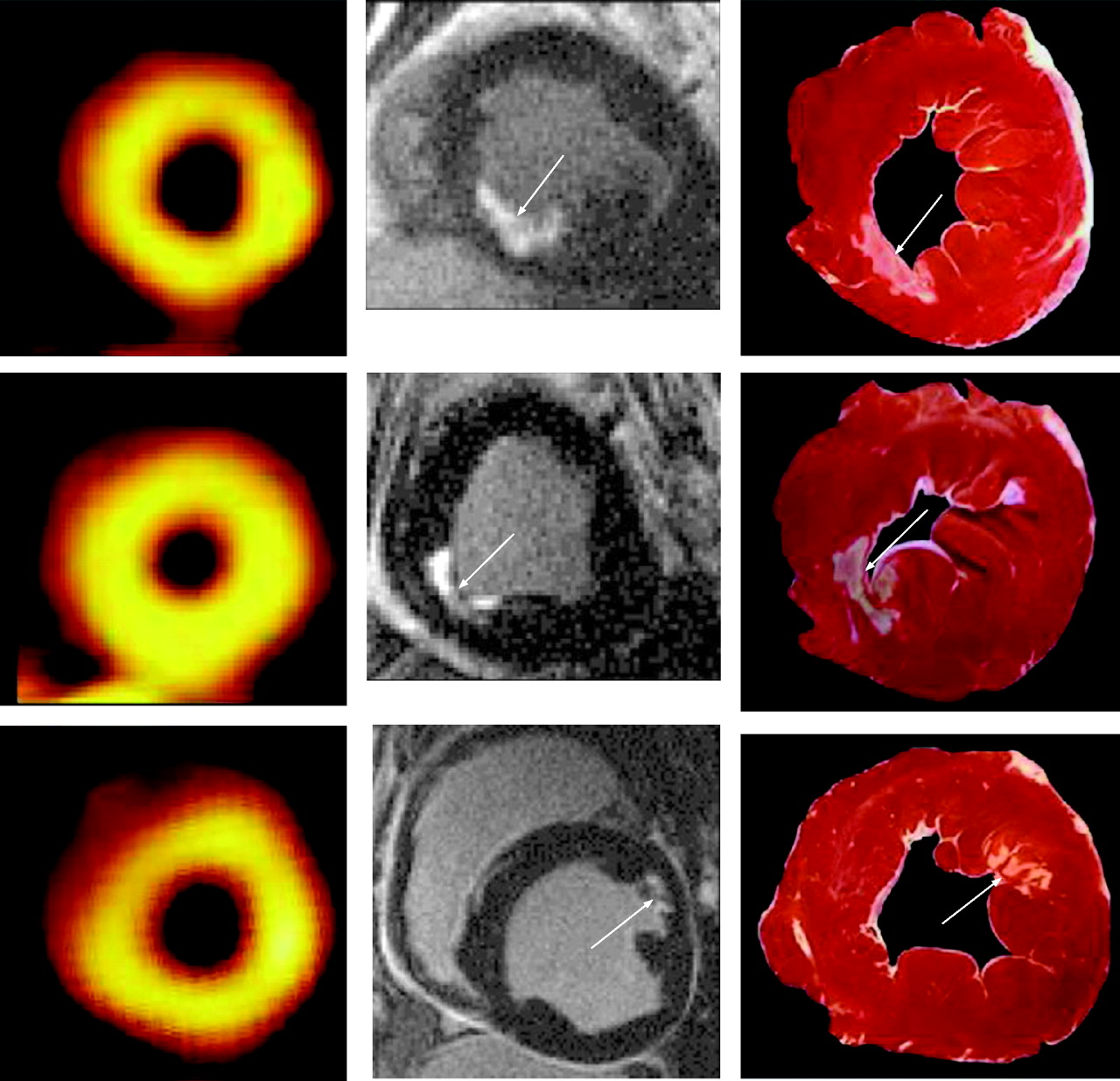
Myocardial infarction can be accurately detected by gadolinium-enhanced CMR, with close correlation with histological findings. With a higher spatial resolution, CMR has been shown to identify small myocardial infarctions even when wall motion and perfusion by SPECT or PET are normal (fig 1).6 7 This has important implications, because the presence of myocardial infarction, whatever its size, is a strong independent prognostic factor, particularly in older people.8

Comparison of 99mTc-sestamibi single-photon emission computed tomography (SPECT) (left), contrast-enhanced cardiovascular magnetic resonance (CMR) (middle) and histological specimens (right) in animal models with subendocardial infarction. With a high spatial resolution and a high contrast-to-noise ratio, CMR can visualise small infarcts confirmed by histology which are undetected by SPECT (adapted from Wagner et al).6
This superior resolution makes CMR the best technique in discriminating viable from non-viable myocardium. Myocardial viability estimated by CMR has become a simple and effective way to predict recovery of function following acute MI and after revascularisation.9 10 When compared with nuclear studies, results are superior to thallium SPECT and comparable with PET.11 12
Coronary arteries
CMR imaging offers a radiation and iodinated-contrast free alternative to CT or x ray angiography for imaging the coronary arteries. Although diagnostic results for detection of CAD are promising,13 this technique is limited by a lower resolution and higher propensity to artefact when compared with the conventional standards. Thus, the current role of CMR coronary angiography is limited to the assessment of congenital coronary anomalies and coronary aneurysms.
Cardiomyopathies
Cardiomyopathies are a heterogeneous group of diseases of the myocardium associated with architectural abnormalities and mechanical dysfunction. Our understanding of these diseases has been facilitated by the use of CMR with late gadolinium enhancement (LGE), which correlates with histological findings and thus permits in vivo characterisation of the myocardium.
Dilated cardiomyopathy
Dilated cardiomyopathy (DCM) is characterised by dilatation and impaired contraction of the left or both ventricles. CMR offers reliable diagnosis of increased ventricular volumes and reduced ejection fraction which can be normalised to body surface area, gender and age. CMR is also useful in establishing the aetiology of heart failure.
Ischaemic cardiomyopathy, which results from persistent ischaemic injury and adverse remodelling, can present in a similar way to a DCM phenotype. LGE has been shown to be extremely reliable in this setting: subendocardial enhancement is virtually diagnostic of ischaemic cardiomyopathy, whereas mid-wall/epicardial enhancement or no enhancement is typical of a non-ischaemic cardiomyopathy.14 The presence of mid-wall LGE in DCM predicts adverse outcomes, and this is independent of more conventional risk markers such as left ventricular ejection fraction.15
Myocarditis
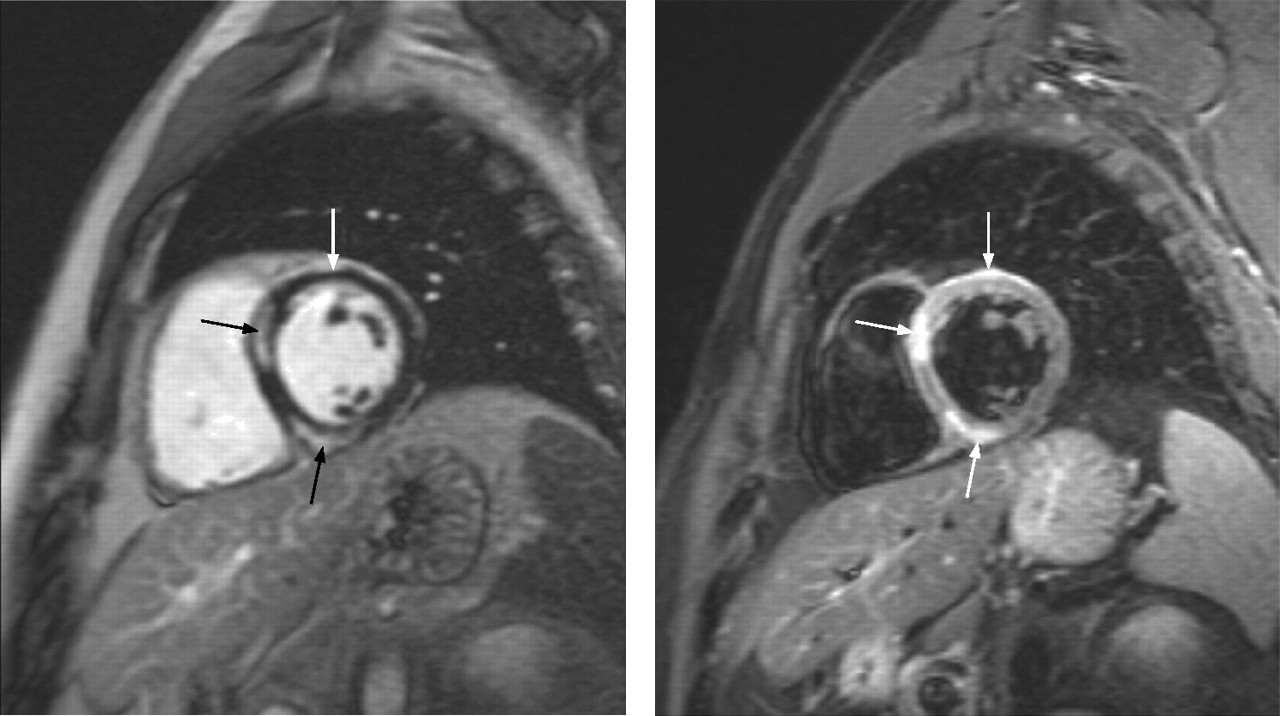
Diagnosis of myocarditis can be challenging as symptoms, ECG changes and troponin rises are variable and often non-specific. LGE demonstrating areas of myocardial injury was seen in 95% of cases confirmed by histopathology.16 Characteristic patterns of LGE affect the septal mid-wall and subepicardial lateral wall (fig 2). LGE also appears to predict adverse remodelling after an acute event.17

Cardiovascular magnetic resonance evaluation of a patient with acute myocarditis. The late gadolinium image (left panel) shows typical enhancement of the mid-wall septal and subepicardial anterior walls (arrows). T2-weighted spin-echo image (right panel) shows increased signal in the same areas of gadolinium enhancement (arrows). The areas of high signal represent increased water content and are consistent with active inflammation. The use of this sequence is therefore helpful in differentiating acute from healed myocarditis.
Hypertrophic cardiomyopathy
Hypertrophic cardiomyopathy (HCM) is thought to be the commonest hereditary cardiac disease and the most frequently found cardiomyopathy. CMR is helpful in establishing or confirming a final diagnosis, detecting hypertrophy missed by echocardiography, especially in the apical and lateral walls.18 19 The presence of patchy mid-wall LGE or widespread perfusion defects is typical of HCM, helping to differentiate it from other forms of left ventricular hypertrophy (fig 3).20
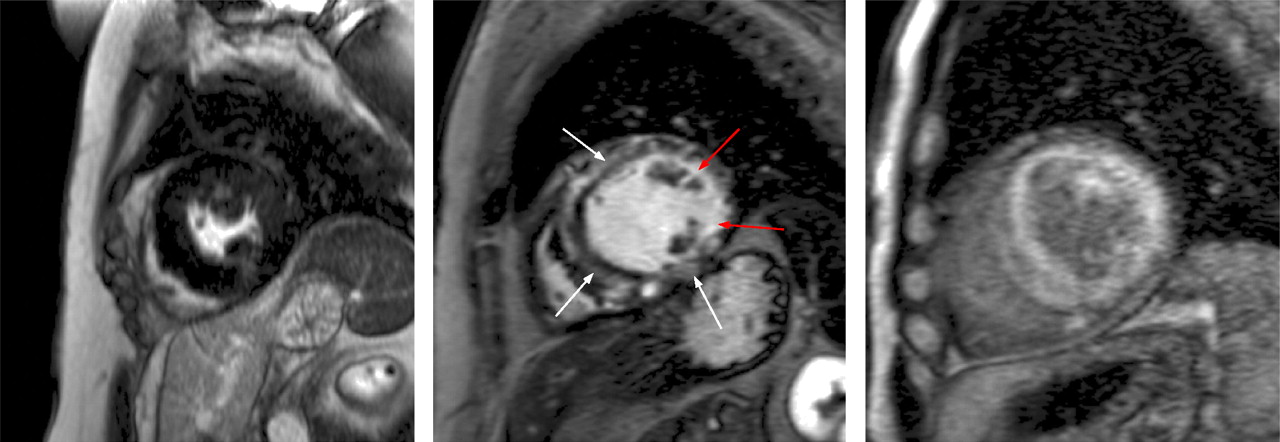
Tissue characterisation by contrast-enhanced cardiovascular magnetic resonance imaging in the evaluation of three different patients with left ventricular hypertrophy. Left panel: there is no evidence of significant myocardial fibrosis in this patient with hypertension, which is consistent with the diagnosis of hypertensive heart disease. Middle panel: diffuse mid-wall patchy fibrosis (white arrows) suggestive of hypertrophic cardiomyopathy; in addition, there is a subendocardial infarction in the lateral wall, which correlates with known coronary artery disease (red arrows). Right panel: diffuse gadolinium enhancement with an associated dark blood pool. This is pathognomonic of cardiac amyloidosis.
LGE is present in about two-thirds of HCM patients, and has been shown to be strongly associated with traditional risk factors for sudden cardiac death and adverse remodelling.21 22 The left ventricular mass index (LVMI) was recently shown to be a more sensitive indicator of risk of death than peak wall thickness,23 and may be used in the future as a potential prognostic marker.
Arrhythmogenic right ventricular cardiomyopathy (ARVC)
ARVC is one of the commonest causes of sudden cardiac death in the young. CMR is useful in the diagnosis of ARVC due to the superior depiction of the right ventricle. The possibility of tissue characterisation allows detection of fibro-fatty replacement, which is the histological hallmark of this condition.
Diagnosis accuracy was evaluated in 232 patients undergoing evaluation for suspected ARVC.24 In the subgroup of patients who met ARVC Task Force criteria, CMR had a high sensitivity (100%) but a low specificity (29%). However, in the subgroup of patients who underwent genotyping, CMR accuracy was extremely high (sensitivity 96% and specificity 78%). Hence, CMR is an important modality in the assessment of ARVC and should be considered in all patients presenting with right ventricular tachyarrhythmias.
Secondary cardiomyopathies
The heart can be affected by a number of systemic conditions. Although cardiac involvement is variable, when it occurs, it is usually associated with a worse outcome.
Examples of these conditions include sarcoidosis, amyloidosis, Anderson–Fabry and other metabolic storage disorders, Chagas disease and muscular dystrophies.
Patients in this group are usually referred when there is suspected cardiac involvement, although sometimes it is an incidental finding in the evaluation of unexplained heart failure or left ventricular hypertrophy.
LGE imaging is extremely helpful in this setting, where infiltration or fibrosis depicted by LGE shows good correlation with endomyocardial biopsy.25 26 Moreover, the presence and extension of LGE are usually associated with more advanced and irreversible forms of cardiomyopathy.27–29
Thus, LGE can detect the presence of cardiac involvement in these conditions, obviating the need for cardiac biopsy, with its inherent invasive risk or potential sampling errors.
A special mention has to be made of iron-overload cardiomyopathy, which is the main cause of mortality of transfusion-dependent haemoglobinopathies. CMR measures T2-star relaxation of the myocardium, which has an inverse correlation with the amount of tissue iron. This is the only non-invasive technique that correlates with left ventricular function and predicts the development of heart failure.30 With the advent of effective cardiac iron-chelating agents and the introduction of the CMR-based T2-star technique to detect and monitor myocardial iron levels, UK mortalities for beta-thalassemia major have decreased by >70% in the last 10 years.31
Valvular heart disease
While echocardiography provides first line imaging of valve disease, CMR can complement when the transthoracic acoustic window is poor and a transesophageal approach is undesirable, or when results of echocardiography and catheterisation are conflicting.
Direct visualisation of all valves and precise flow quantification, either by volumetric or flow mapping methods, are important components of this technique.
Valve stenosis quantification by planimetry or peak flow velocity is technically possible for all valves. Direct planimetry of aortic valve stenosis has been shown to be feasible, reproducible and comparable with both echocardiographic and cardiac catheterisation estimations.32
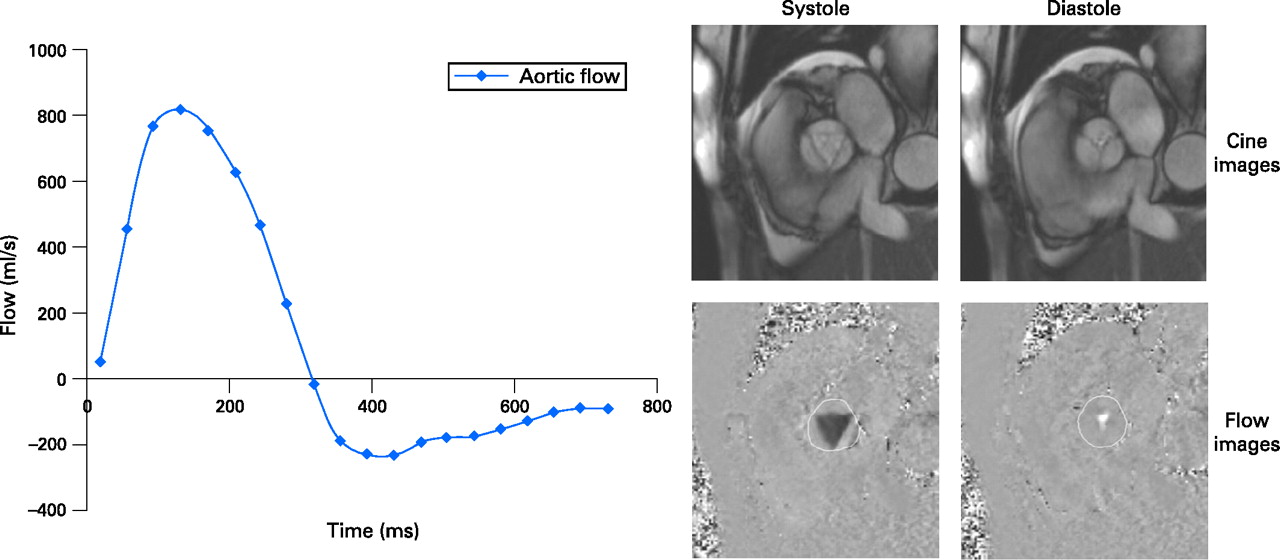
Regurgitant fraction quantification by flow mapping is accurate and robust, particular for the semilunar valves (fig 4). For the atrioventricular valves, regurgitation can be quantified by combined use of volumetric and flow mapping methods. Ventricular volumetric analysis is considered to be the reference standard, which is extremely useful for follow-up and management of regurgitant lesions.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Flow imaging of the aortic valve in a patient with aortic regurgitation. This technique uses a modified gradient-echo sequence where pixel intensity reflects blood velocity rather than tissue composition. Blood velocities within the region of interest throughout the cardiac cycle can be estimated, and flow curves can be derived (graph), allowing measurement of stroke volume, cardiac output, forward and regurgitant flows.
Although rarely used for the diagnosis of endocarditis, CMR can be helpful in assessing myocardial extension of the infectious process and to plan surgical intervention.
Pericardial disease
Although echocardiography is more readily available, complete anatomical and functional information makes CMR an attractive way to assess the pericardium.
Pericardial effusions can be easily visualised and differentiated from mediastinal fat or pleural effusions. In addition, CMR has the advantage of assessing complex or loculated effusions and determining fluid content (eg, haemorrhagic). Signs of tamponade, such as chamber collapse or exaggerated respiratory flattening of the ventricular septum, can also be assessed.
Pericardial thickening can be characterised and quantified for the evaluation of constrictive pericariditis. Again, signs of functional repercussion, such as ventricular interdependence, can also be assessed. Therefore, this technique can be used for differentiation between constrictive pericarditis and restrictive cardiomyopathy. Surgical planning for pericardiectomy is another indication. However, pericardial calcification is not easily seen, and CT is recommended in this scenario.
Pericardial cysts can be easily recognised and usually preclude the need for an invasive diagnostic procedure.
Cardiac masses
The possibility of three-dimensional imaging and tissue characterisation makes CMR one of the most important techniques in the evaluation of suspected or confirmed cardiac masses.
CMR is particularly helpful in determining the relationship to normal intracardiac structures and tumour extension to the pericardium, adjacent vascular and mediastinal structures. The use of multiple sequences, coupled with the use of gadolinium, provides information on tissue characteristics, vascularity, necrosis and fibrosis, and can point towards a specific diagnosis.
Morphological CMR features are independent predictors of lesion type of cardiac and paracardiac masses.33 Thus, CMR yields important information for diagnosis, management and follow-up.
Cardiac thrombi are far more common than cardiac tumours. Recognition is important because anticoagulation may reduce the risk of embolisation. In this regard, LGE CMR is considered the reference technique for detection of ventricular thrombi when compared with other conventional techniques (sensitivity 88% vs 23% transthoracic and 40% with transesophageal echocardiogram).34
Congenital heart disease
A growing application of CMR is in congenital heart disease (CHD), which reflects the increasing number of patients surviving into adulthood due to advances in medical care and in palliative and corrective surgical procedures.
Complete anatomical and functional imaging is usually possible with CMR, which is regarded as a complementary modality to the more standard echocardiography. Advantages of CMR over echocardiography include a wider field of view allowing visualisation of all thoracic structures, more accurate volume estimation of the ventricles and more precise flow measurements over vascular structures.
In suspected CHD, CMR can be useful to assess structures not clearly visualised by the latter (eg, right ventricle, pulmonary artery and veins). Moreover, the Qp/Qs ratio measured by flow mapping can confidently exclude any significant shunt.
For confirmed CHD, CMR may help managing patients by providing additional anatomical information or precise ventricular volumetric and flow measurements. However, this technique is more commonly used in repaired CHD, especially after palliative procedures, where echocardiography is limited by the intrinsically abnormal cardiac arrangements and distorted thoracic anatomy.
Interpretation of congenital studies can be quite challenging. Thus, expertise in CMR is recommended in centres specialised in the care of patients with CHD.
Great vessels
CMR is well established for evaluation of a wide variety of vascular diseases. It is particularly useful for vascular lumen imaging with its ability to generate projection angiograms.
Gadolinium-enhanced magnetic resonance angiography is a well-recognised technique for the aorta and major branches. Diagnosis accuracy is very high when compared with conventional angiography, and is considered to be the most cost-effective technique for evaluation of carotids and peripheral arteries.35
In addition to angiography, the wide variety of soft tissue contrast available on CMR can be applied to vascular imaging to assess features of vessel wall such as thrombus, haematoma, inflammation and atherosclerosis. Velocity mapping can be used to assess and measure blood flow, providing additional functional information.
The versatility of CMR has made the ideal imaging modality for the evaluation of the thoracic and abdominal aorta disease. The lack of radiation or the need for iodinated contrast agents is an advantage for serial follow-up studies.
Of growing interest is pulmonary venous angiography prior to atrial fibrillation ablation. Anatomical information provided by the angiography can then be merged with electrophysiological mapping and aid this type of ablation procedure.
Protocols
Whatever the clinical indication, protocols are encouraged for a comprehensive and systematic approach. A review on standardised CMR protocols can be found elsewhere.36
Limitations
Despite providing the most comprehensive information, CMR is a relatively expensive technique and is not readily available in some institutions. Image acquisition is technically challenging, and image interpretation requires adequate training. In CMR studies, scan times are relatively long, patients have to lie flat, and monitoring and perfusion devices inside the scanning room have to be MR-compatible. Therefore, CMR is not suitable for the very unstable patient and should be avoided in these patients if there are other studies which can give similar information.
Claustrophobia can be problematic, but with reassurance and rarely the use of mild sedation, less than 1% of patients are unable to tolerate the scan.37
Despite pacemakers and implantable electronic devices being regarded as contraindications, CMR can potentially be safely performed when appropriate precautions are taken.38 With the possible exception of intracerebral devices, metallic implants are usually safe. Further information on safety can be found in specific statements,39 or in dedicated websites (eg, http://www.mrisafety.com).
Finally, in patients with end-stage renal failure, gadolinium-contrast agents should be used with caution due to the potential risk of nephrogenic systemic fibrosis,40 although this has been greatly mitigated by the use of the more stable contrast agents which use a cyclic chelation molecule.
Future perspectives
Although most important developments happened in the last 10 years, attention has been given to new exciting areas which may further support the use of CMR in the future. Particular areas of interest are atherosclerosis and plaque characterisation, intravascular and targeted contrast agents, resynchronisation and identification of target areas for deployment of stem cells. Interventional CMR is becoming an attracting alternative in electrophysiological studies, reducing radiation exposure significantly and potentially reducing procedure times, especially in the more complex cases.
Of considerable interest also is the development of high-magnetic-field 3-Tesla machines (as opposed to the current 1.5-Tesla scanners). Although currently in validation against the current scanners, they have advantages which can be mostly explored on myocardial perfusion and coronary angiography, and may become the reference in the mid-term.
Conclusion
Currently, CMR offers the most comprehensive method of all imaging techniques to evaluate the structure and function of the heart.
Extensive research in the last decade has validated this technique in several clinical settings and supports its use in daily practice. Lack of radiation and no use of iodinated contrast agents is a considerable advantage over other techniques, and it is expected to be one of the imaging modalities that will grow the most in the next decade.
However, lack of availability, medical training and cost constrains a more widespread use of this technique. Therefore, it is regarded as complement to echocardiography, since most of the general indications are similar.
Further studies, in particular prospective multicentre trials, are needed to embrace CMR in routine clinical management. Thus, future challenges for CMR include development of strategies that will allow healthcare systems to benefit from the increased diagnostic accuracy, improved risk assessment and therapeutic decision-making.
References
Footnotes
Competing interests None.