Article Text

Statistics from Altmetric.com
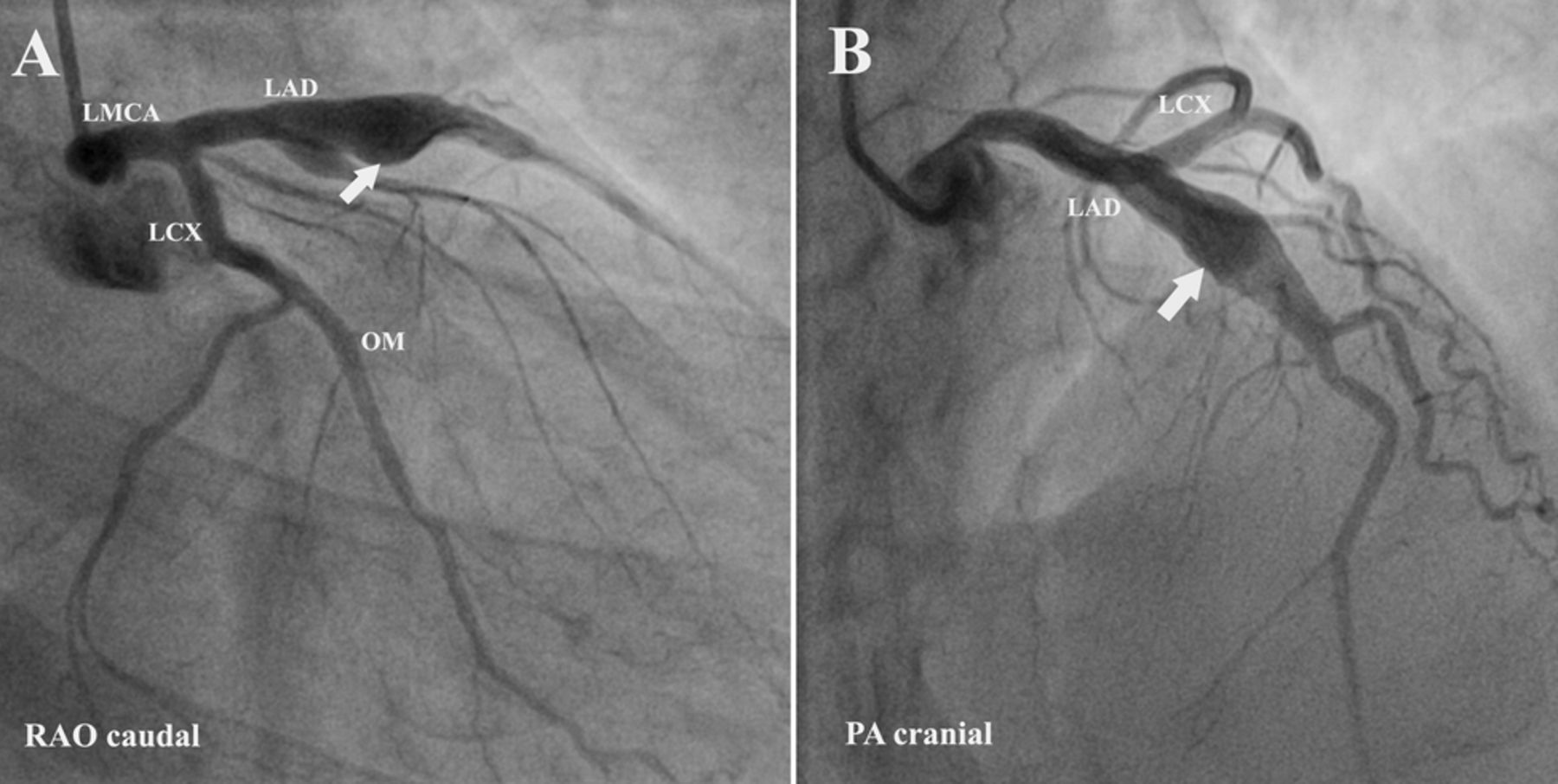
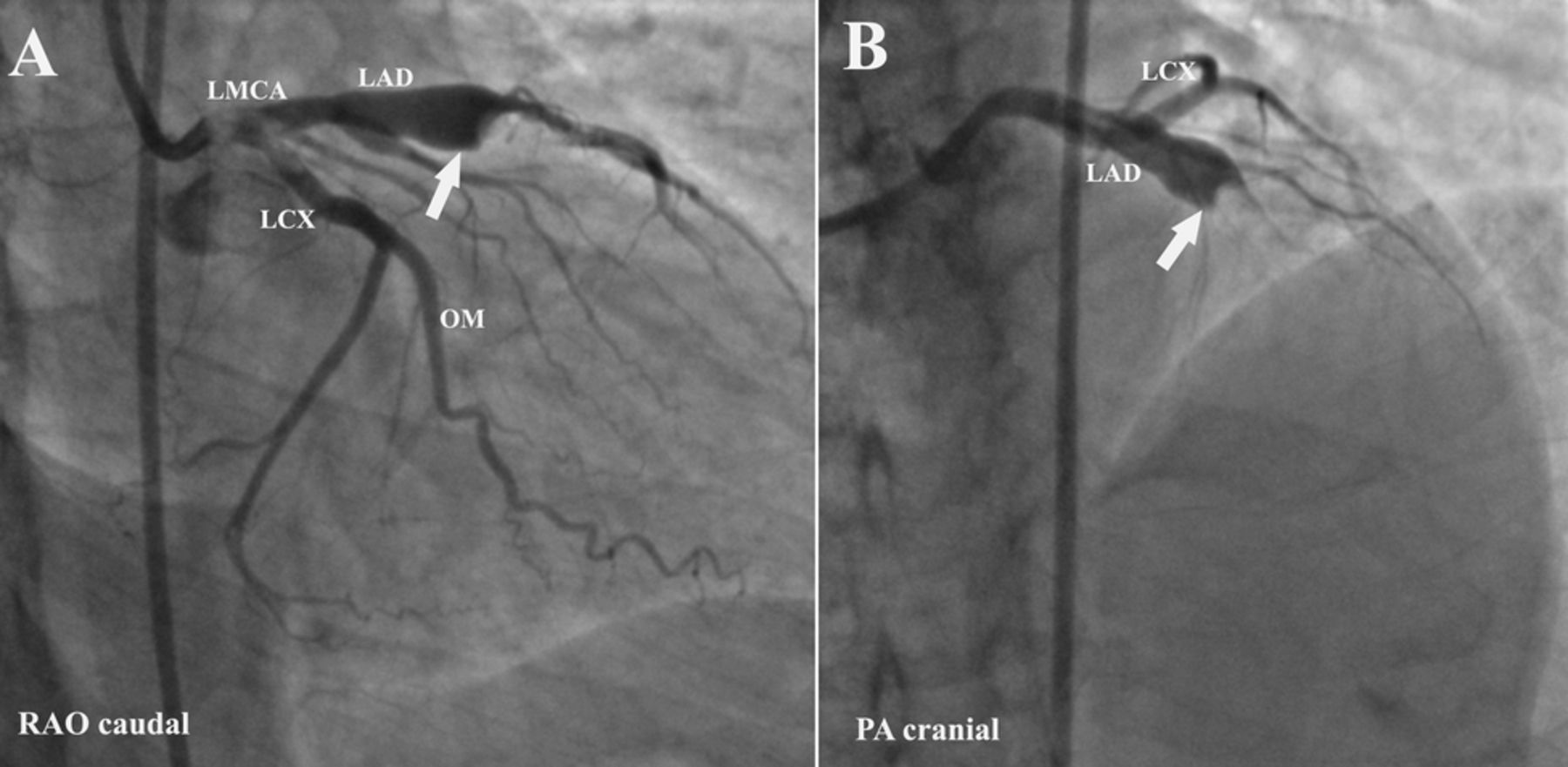
A 28-year-old man with no traditional coronary risk factors presented with history of retrosternal chest pain since 1 h. Physical examination revealed features of acute pulmonary oedema. Electrocardiogram showed acute anterior wall myocardial infarction. Coronary angiogram showed a large fusiform aneurysm (10 mm×6 mm) of mid-left anterior descending coronary artery with high thrombus burden producing total occlusion of vessel (figure 1 A, B and online supplementary movie 1). Thrombus aspiration was done with 5.4 F- thrombus vacuum aspiration catheter (TVAC) followed by intracoronary tirofiban administration in view of high thrombus burden. Postaspiration, coronary angiogram showed TIMI 3 flow in distal left anterior descending coronary artery (figure 2 A, B and online supplementary movie 2). Postprocedure, patient's angina was relieved and electrocardiogram showed good ST resolution. Subsequently, he was started on unfractionated heparin and discharged on warfarin sodium, aspirin and atorvastatin.

A and B: Coronary angiogram (before aspiration) showing fusiform aneurysm (10 mm×6 mm) of mid-left anterior descending coronary artery with thrombus burden producing total occlusion of vessel (Arrow). RAO-right anterior oblique view, PA- posterior anterior view, LMCA-left main coronary artery, LAD-left anterior descending coronary artery, LCX-left circumflex coronary artery, OM-obtuse marginal branch.
{kind=link}
{kind=link}
A and B: Coronary angiogram (after aspiration) showing fusiform aneurysm (10 mm×6 mm) of mid-left anterior descending coronary artery with TIMI 3 flow in distally (arrow). No thrombus seen. RAO-right anterior oblique view, PA- posterior anterior view, LMCA-left main coronary artery, LAD-left anterior descending coronary artery, LCX-left circumflex coronary artery, OM-obtuse marginal branch.
Coronary artery aneurysms are rare and usually defined as dilatation of a segment of a coronary artery more than 1.5 times the normal size.1 The important causes of coronary artery aneurysms are atherosclerosis, Kawasaki disease, Behcet's disease, mycotic, congenital or idiopathic. Spontaneous dissection, spasm or thrombus formation with distal embolisation can occur in coronary aneurysms and, hence, cause myocardial ischaemia or infraction.2
This case highlights the fact that coronary artery aneurysms with intraluminal thrombus can be an important cause for acute myocardial infarction in individuals with no traditional coronary risk factors. These patients may require long-term anticoagulation for preventing future thrombotic events.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online video 1
- Data supplement 2 - Online video 2
Footnotes
-
Contributors KT Sajeer: substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data. Kader Muneer: drafting the article or revising it critically for important intellectual content. C G Sajeev: final approval of the version to be published.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; internally peer reviewed.