Article Text

Abstract
Objective To determine whether a third generation vasodilating β blocker (celiprolol) has long term clinical advantages over metoprolol in patients with chronic heart failure.
Design A double blind placebo controlled randomised trial.
Setting University teaching Hospital.
Patients 50 patients with stable chronic heart failure (NYHA class II-IV) due to idiopathic dilated, ischaemic, or hypertensive cardiomyopathy, with left ventricular ejection fraction < 0.45.
Interventions Celiprolol 200 mg daily (n = 21), metoprolol 50 mg twice daily (n = 19), or placebo (n = 10) for three months with a four week dose titration period. After the double blind period, patients entered an open label study (with placebo group receiving β blockers) and were assessed after one year.
Main outcome measures Clinical response, efficacy, and tolerance were assessed by the Minnesota heart failure symptom questionnaire, six minute walk test, Doppler echocardiography (systolic and diastolic function), radionuclide ventriculography, and atrial and brain natriuretic peptides measured at baseline and after three months.
Results In the metoprolol group at 12 weeksv baseline there was a 47% reduction in symptom score (p < 0.001), improvement of NYHA class (mean (SEM), 2.6 (0.12) to 1.9 (0.13), p = 0.001), exercise distance (1246 (54) to 1402 (52) feet, p < 0.001), and left ventricular ejection fraction (26.9(3.1)% to 31(3.0)%, p = 0.016), and a fall in heart rate (resting, 79 (3) to 62 (3) beats/min, p < 0.001). In the celiprolol group there was a 38% reduction in symptom score (p = 0.02), less improvement in exercise distance (1191 (55) to 1256 (61) feet, p = 0.05), and no significant changes in NYHA class, left ventricular ejection fraction, or heart rate. Mortality at one year was 11% in metoprolol and 19% in the celiprolol group, and symptomatic improvement was maintained in the survivors.
Conclusions Both drugs were well tolerated but the vasodilator properties of celiprolol do not seem to provide any obvious additional benefit in the long term treatment of heart failure.
- β blockers
- heart failure
- metoprolol
- celiprolol
Statistics from Altmetric.com
Increased sympathetic activity is a recognised feature of heart failure.1-3 Although initially supporting the failing heart, prolonged excessive activation of the sympathetic nervous system has many potentially adverse effects, including a direct cytotoxic action on myocardial cells, promotion of arrhythmias, decreased coronary blood flow, excessive vasoconstriction reducing tissue perfusion, and stimulation of myocardial collagen formation.4-7 Plasma noradrenaline, which is an index of sympathetic activity, is increased in heart failure and has been shown to be a powerful predictor of survival.3 ,8Therefore the use of β blockers in chronic heart failure has a logical foundation, but the potential for worsening heart failure through their recognised negative inotropic action has inhibited their use. However, many recent studies have confirmed the initial findings of Waagstein and his colleagues9 that β blocker treatment improves left ventricular ejection fraction and diastolic function, myocardial energetics, and in some studies this is associated with symptomatic improvement and increased exercise capacity, although a reduction in mortality has not been definitively proven.10-18 Metoprolol, which has been the most widely used β blocker, is not tolerated by at least 15% of patients during the initiation of treatment.19 In a previous study we showed that this drug, even in very low doses (6.25 mg), produced a rise in atrial natriuretic factor and brain (ventricular) natriuretic peptide.20 In contrast, the vasodilating β blocker celiprolol was associated with a significant fall in both types of natriuretic peptide and a small rise in cardiac output. Although in that study it appeared that a vasodilating β blocker was superior for initiation of treatment, there are no published data directly comparing the newer third generation vasodilating β blockers with metoprolol for long term treatment of heart failure. We therefore carried out a randomised double blind trial of celiprolol versus metoprolol and placebo over a long period (three months), followed by an open phase for one year to determine whether the initial advantages of a vasodilating β blocker persist.
Methods
TRIAL DESIGN
This was a randomised placebo controlled double blind trial. After baseline measurements patients were randomised to receive treatment with celiprolol, metoprolol, or placebo (in a ratio 2:2:1). All were in identical capsules. There was a four week dose titration period, increasing the dose of celiprolol from 25 mg daily to 200 mg, and of metoprolol from 6.25 mg twice daily to 50 mg twice daily, with a dosage increase at weekly intervals. A maintenance phase followed for eight weeks (total 12 weeks of treatment). At the end of 12 weeks, baseline measurements were repeated.
Clinical assessment, measurement of autonomic function, routine blood tests, and estimation of natriuretic peptides were carried out at four and eight weeks. Compliance was checked by counting the remaining capsules at each visit. The study objectives were to compare the efficacy and tolerability of metoprolol and celiprolol with placebo by assessment of symptoms (questionnaire), exercise capacity (a six minute walking test), left ventricular ejection fraction (radionuclide ventriculography and echocardiography), left ventricular diastolic function (Doppler echocardiography), natriuretic peptides, and autonomic function (heart rate and blood pressure variability). The primary end points were symptom score, exercise time, and left ventricular ejection fraction.
The study had a 90% power to detect a 55% reduction in symptom score, a 20% increase in the six minute walking time, and a 12% increase in left ventricular ejection fraction from baseline, all of which would be considered clinically significant.
STUDY PATIENTS
We recruited 50 patients with a clinical diagnosis of congestive heart failure on standard treatment with diuretics, digoxin, and angiotensin converting enzyme inhibitors, and with a left ventricular ejection fraction of less than 45% (by radionuclide ventriculography or echocardiography). Patients were excluded if they had valvar heart disease as the aetiology of left ventricular dysfunction, active myocarditis, active angina, documented history of sustained ventricular tachycardia (more than 15 seconds) or symptomatic non-sustained ventricular tachycardia, or second or third degree atrioventricular block. Four patients had permanent pacemakers. In addition, patients with symptomatic peripheral vascular disease, chronic obstructive lung disease, asthma, long term alcohol or drug abuse, chronic renal failure (serum creatinine > 200 μmol/l), and hepatic, haematological, neurological, or collagen vascular diseases were excluded. All subjects gave written informed consent and the study was approved by the ethics committee of the faculty of medicine, Chinese University of Hong Kong.
STUDY MEASUREMENTS
Baseline measurements included assessment of symptoms using the Minnesota heart failure symptom questionnaire,21 routine clinical examination (pulse, heart rate, sitting and standing blood pressure, examination of jugular venous pressure, position of apex beat, and presence or absence of heart murmur or lung rales). A six minute corridor walk test was carried out as previously described.22
Cross sectional echocardiography with continuous and pulse wave Doppler studies was performed. Standard M mode measurements of left ventricular end diastolic dimension, end systolic dimension, fractional shortening, ejection fraction, and left atrial size were recorded. Pulse wave Doppler echocardiography was performed by measuring mitral inflow velocity in the apical four chamber view with the sampling window placed at the mitral annulus (to standardise measurements). Diastolic variables were measured from at least three beats: peak early mitral valve filling velocity (E wave), peak atrial filling (A wave), ratio of peak early and atrial filling velocity (E/A), deceleration time of the E wave (DT), and isovolumic relaxation time (IVRT) as described.23 The diastolic mitral flow pattern was divided into normal, abnormal relaxation pattern, and restrictive filling pattern, as previously described.24 ,25 In this study, the grouping of Doppler transmitral flow pattern into restrictive and non-restrictive categories was based on the E/A ratio where E/A < 1 was considered non-restrictive, E/A > 2 was considered restrictive, and E/A = 1–2 was considered indeterminate and required the deceleration time of the E wave to be measured as well. A deceleration time of > 140 ms was classified as non-restrictive and < 140 ms as restrictive. All patients in this study were grouped according to the restrictive or non-restrictive pattern, using the combination of the E/A ratio and deceleration time. Routine radionuclide ventriculography (MUGA) at rest was performed. Results were considered to be unreliable in four patients in the metoprolol group and five in the celiprolol group because of arrhythmias. All recordings were satisfactory in the placebo group.
Natriuretic peptides (atrial natriuretic factor and brain ventricular natriuretic peptide) were assayed as previously described.20 ,26 A 24 hour ECG (Holter) monitoring was carried out in all patients for assessment of arrhythmias, hourly heart rate, and heart rate variability (Marquette Holter System).
Routine laboratory tests were performed, including a complete blood count and renal and liver function tests. A chest radiograph was taken at baseline only.
Patients meeting the inclusion criteria entered into the study. Routine blood tests and samples for atrial natriuretic factor and brain ventricular natriuretic peptide were repeated at four and eight weeks, and all baseline measurements were repeated at 12 weeks.
OPEN LABEL PERIOD
Following the double blind study period, patients continued with their previous treatment in an unblinded fashion. Those who had been receiving placebo were converted to metoprolol (or carvedilol, one patient). After 12 months of treatment repeat clinical assessment was undertaken with echocardiography.
STATISTICAL ANALYSIS
Differences between the treatment groups were evaluated by repeated measures analysis of variance for continuous variables (anova), with Bartlett’s test for homogeneity of variances and Tukey-Kramer multiple comparison test if p was < 0.05. Within group differences were tested by a paired t test, Wilcoxon signed rank test for non-parametric data, or χ2 test for discrete variables. For comparison of baseline variable all patients were included. For comparison of 12 weeks with baseline data only those patients still in the trial were analysed. Results are expressed as mean (SEM). Differences were considered significant if the probability (p) value was < 0.05.
Results
BASELINE CHARACTERISTICS
Fifty patients were recruited in this study and were randomised to receive metoprolol (n = 19), celiprolol (n = 21), or placebo (n = 10). The baseline characteristics are shown in table 1. The treatment groups did not differ significantly with respect to gender, aetiology, New York Heart Association (NYHA) functional class, symptom questionnaire score, exercise tolerance (six minute walking test), baseline sitting and standing blood pressure, heart rate, left ventricular ejection fraction by radionuclide ventriculography, left ventricular end diastolic dimension, fractional shortening, natriuretic peptide concentrations, frusemide dosage, and numbers of patients taking angiotensin converting enzyme inhibitors or nitrates. The age of the metoprolol group was significantly different from the celiprolol group, but not different from placebo. This was because of one young patient who was recruited into the metoprolol group.
Baseline clinical characteristics of study patients
WITHDRAWALS AND TOLERANCE
Two patients in the metoprolol group were withdrawn at week 3 and 5 for increasing chest tightness, fainting attacks, and generally feeling unwell. Four patients in the celiprolol group did not complete the randomised period, and two patients died at five and 11 weeks, respectively. Two patients were withdrawn at week 1 and week 3 because of nausea and increasing angina. Two patients were withdrawn from the placebo group, one with angina and one because of increasing heart failure, but there were no deaths in the placebo group during the double blind period. Three patients in the metoprolol group were unable to tolerate the full dose (50 mg twice daily) and were maintained on 25 mg twice daily (two patients) or 50 mg morning and 25 mg in the evening. All but one patient tolerated the full dose of celiprolol. Compliance was otherwise good.
SYMPTOMS
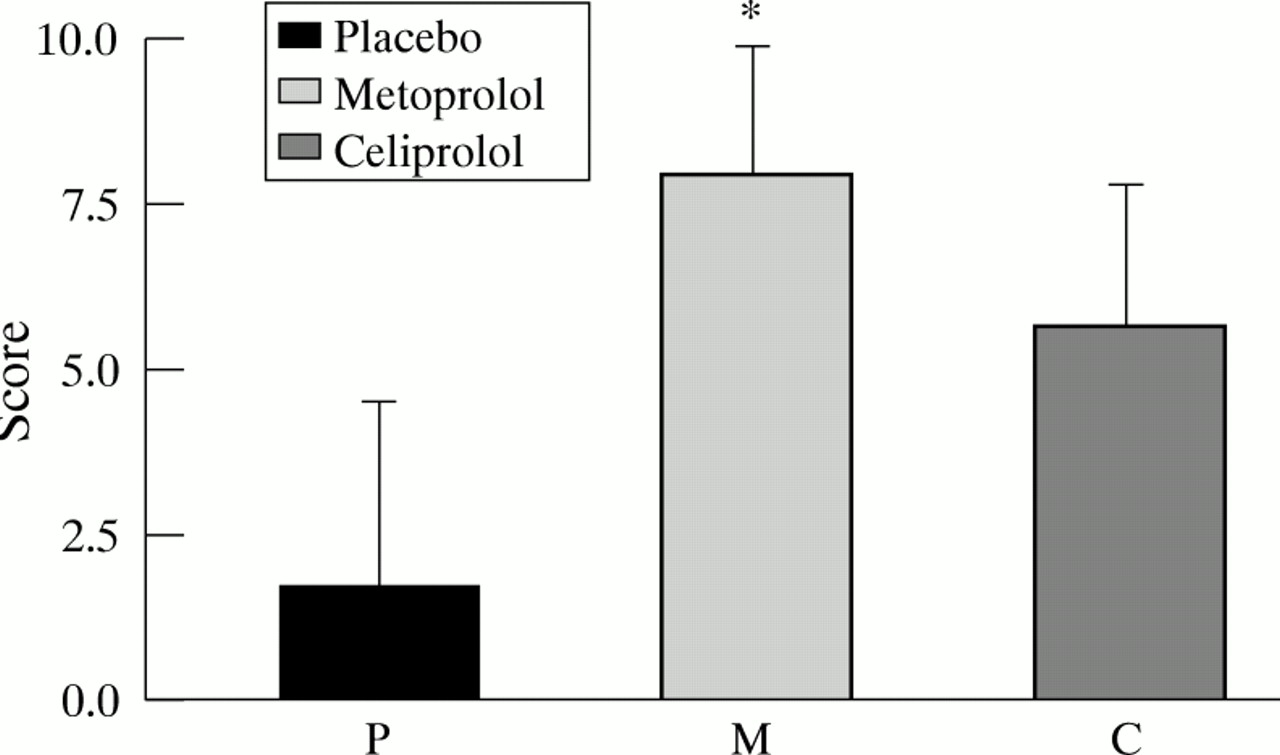
The results of the symptom questionnaire score and NYHA functional class are shown in table 2. There was a significant reduction in a symptom score on metoprolol (p = 0.003). The improvement of celiprolol was similar but smaller (p = 0.018), but there was no significant difference between metoprolol and celiprolol. There was no significant change in symptoms in the placebo group (p = 0.6) (fig1). Similarly, NYHA functional class improved in the metoprolol group from 2.6 (0.12) at baseline to 1.94 (0.13) (p = 0.001). There was no change in the placebo group, and a small but non-significant reduction in the celiprolol group (p = 0.11).
Symptoms, exercise capacity, blood pressure, and heart rate

Reduction in symptom score after 12 weeks of placebo (P), metoprolol (M), or celiprolol (C) treatment. *p = 0.073 v placebo.
EXERCISE CAPACITY
There was a significant increase in exercise capacity on metoprolol, as judged by distance covered, from 1246 (54) to 1402 (52) feet (p = 0.0006). A smaller improvement was seen with celiprolol (1191 (55) to 1256 (61) feet; p = 0.049) (table 2). There was a non-significant change in the placebo group. However, the mean increase in distance for metoprolol and celiprolol were not significantly different from the placebo group. The mean increase in exercise distance on metoprolol was 154 (39) feet compared with 67 (32) feet on celiprolol, but the difference is not significant (p = 0.09).
LEFT VENTRICULAR SYSTOLIC FUNCTION
Left ventricular ejection fraction measured by radionuclide ventriculography rose in the metoprolol group from 26.9(3.1)% to 31 (3.4)% (p = 0.016) (table 3). In the celiprolol group, the mean value rose from 30.2(2.1)% at baseline to 36.6(3.8)% at 12 weeks, but this was statistically non-significant (p = 0.2). The median left ventricular ejection fraction was 32% at baseline and 33% at 12 weeks, and there was a fall in the value in the placebo group (p = 0.047). Compared with placebo, the increase in left ventricular ejection fraction was significant for both metoprolol and celiprolol (p = 0.005 and p = 0.03 respectively, fig 2) but there was no significant difference between the two drugs. Echo derived fractional shortening showed a trend to increase in the metoprolol group (p = 0.09) with no significant change in celiprolol group (p = 0.23). Despite these improvements in left ventricular systolic function, left ventricular end diastolic dimension did not change significantly in any group.
Change in left ventricular size and systolic function between weeks 0 and 12

Changes in left ventricular ejection fraction (LVEF) after 12 weeks of placebo (P), metoprolol (M), or celiprolol (C) treatment. *p = 0.0049, †p = 0.028 v placebo.
LEFT VENTRICULAR DIASTOLIC FUNCTION
There was a trend for a less restrictive filling in those patients receiving metoprolol, with a rise in the deceleration time of the E wave from 149 (32) to 207 (25) ms, but this was not significant (p = 0.17) (table 4). Similarly, the percentage of patients with a restrictive filling pattern at baseline fell from 62% to 50%. By contrast in the celiprolol group the percentage of patients with a restrictive filling pattern increased from 50% to 67%.
Changes in diastolic function by Doppler echocardiography between weeks 0 and 12
NATRIURETIC PEPTIDES
Although there was an initial fall in atrial natriuretic factor concentrations in both metoprolol and celiprolol groups at eight weeks compared with baseline, by 12 weeks the differences were non-significant. Brain natriuretic peptide concentrations showed little change in any patient group between baseline and 12 weeks, although there was a non-significant trend for the values to increase in the placebo group (table 5).
Changes in natriuretic peptides, weeks 0, 4, 8, and 12
HOLTER ANALYSIS
At baseline there was no significant difference in heart rates between the three treatment groups throughout the 24 hour period. However, after 12 weeks of treatment there was significant reduction in resting heart rate in the metoprolol group (p < 0.001) (fig 3). There was no significant change in either the placebo or the celiprolol group, either in resting heart rate or throughout the 24 hour period (fig 3), and the difference between metoprolol and celiprolol was significant (p < 0.001).

{kind=link}
{kind=link}
{kind=link}
24 hour heart rate (Holter) analysis at baseline and after 12 weeks of treatment with placebo (P), metoprolol (M), or celiprolol (C).
ONE YEAR FOLLOW UP DATA
At one year after entering the study (table 6) the overall mortality was two of 19 patients (11%) in the metoprolol group, four of 21 (19%) in the celiprolol group, and three of 10 (30%) in the placebo group. Seven patients from the placebo group were transferred to β blocker treatment and three continued with their previous treatment. Symptomatic improvement was maintained with no significant difference in NYHA class from the end of the 12 week randomised period and at one year. Improvement in left ventricular fractional shortening was maintained. In diastole the E wave deceleration time remained longer in both metoprolol and celiprolol group than at baseline, and the values were comparable to the measurements at the end of the randomised study period.
One year follow up
Discussion
This study is the first directly to compare metoprolol with a third generation vasodilating β blocker in the treatment of chronic heart failure. We were unable to show any significant differences between the vasodilating β blocker celiprolol and metoprolol compared to placebo with long term treatment, despite the apparent superiority of celiprolol during the initiation of treatment.20 In contrast, many of the results suggest that metoprolol may be more effective, with clearer improvement in symptoms, exercise capacity, and left ventricular ejection fraction compared to baseline, and significant improvement in left ventricular ejection fraction compared to placebo. It is well documented that initial treatment with β blockers can have deleterious effects, and Hall et al 15 showed that in patients treated with metoprolol there was an initial decline in ventricular function over the first day but a significant and marked improvement later, which was clearly apparent at three months. Similarly in the USA carvedilol heart failure study group, seven deaths occurred during the run in period and an additional 17 patients (1.4%) were not randomised because of worsening heart failure during this phase.14 In an earlier trial with carvedilol, seven of 56 patients died or could not tolerate the drug, and an additional 37% had worsening heart failure while the dose was being increased.27 In a previous study we showed that celiprolol did not have acute deleterious effects when given to patients with severe heart failure and was associated with a fall in atrial and brain ventricular peptides and a small rise in cardiac output; this contrasted with a rise in both types of peptide after a small dose of metoprolol.20 However, it is apparent that these initial advantages of celiprolol, presumably the result of the ancillary vasodilator properties, do not produce any prolonged benefit. This may be relevant to the mechanisms, still unexplained, that underly the improvement in ejection fraction, symptoms, and exercise capacity following treatment with β blockers.
The vasodilating action of celiprolol is the result of various mechanisms. Celiprolol possesses some weak β2 agonist activity.28 There is evidence that it also has weak α2 blocking activity and a direct smooth muscle relaxing effect. Its relaxing effect on human arteries and veins is not completely inhibited by β blockade.28 Celiprolol has been widely used for the treatment of hypertension and angina and has been shown to have the equivalent antihypertensive efficacy to other β blockers such as propranolol, atenolol, metoprolol, and pindolol.29 ,30 The drug also has similar antihypertensive effect to an angiotensin converting enzyme inhibitor such as enalapril.29 It induces a reduction of peripheral vascular resistance with maintenance of resting heart rate, cardiac output, and renal perfusion. It also causes modest improvements in plasma lipid profiles.30 Therefore celiprolol has actions which are theoretically attractive for the treatment of heart failure, though there may be concern about its β2 agonist activity because in heart failure the β1/β2 ratio is reduced; however, this is due to a relative rather than an absolute increase in the numbers of β2 receptors,31and it is unclear whether these changes are functionally important. Nevertheless it seems that the recognised vasodilating activity of celiprolol does not improve symptoms or systolic function compared to β blockade alone, and this underlines the importance of the β blocking function. The major difference we observed between the two drugs was the markedly different effect on heart rate. It is difficult to be sure whether this was due to the β2 agonist activity of celiprolol or reflected its vasodilating action. The final dose given to the patients (200 mg daily) has been shown to be effective in hypertension and angina, so that underdosing is unlikely to be the explanation. However, the effect of β blockers on the heart rate alone may be their most important property in heart failure.16
Diastolic dysfunction is virtually universal in patients with systolic heart failure and affects both the left and right ventricles.32 In this study we found a trend (not significant) towards improving diastolic dysfunction (less restrictive filling) in patients receiving metoprolol but not in those receiving placebo or celiprolol. Recently Anderson et al 33 showed that in patients with idiopathic dilated cardiomyopathy, metoprolol treatment was associated with changes in Doppler flow variables which implied a less restrictive filling pattern, such as an increase in E wave deceleration time, similar to the results in our study. They suggested that these effects on diastolic filling may account for the subsequent myocardial systolic recovery. There is little doubt that metoprolol causes a significant improvement in the ejection fraction9-17—also confirmed in this study—and β blockade is associated with significant effects on left ventricular mass and geometry.34 However, the improvement is only apparent after one month of treatment.15 It is possible that a simple reduction in heart rate will improve ventricular filling and this secondarily leads to improved systolic function by a change in geometry of the heart.
LIMITATIONS OF THE STUDY
Our study had a small number of patients and there is a possibility of type II error. The small number of placebo patients and the wide scatter of values meant that many potential differences did not quite reach statistical significance and because of this the advantages of both the β blockers versus placebo may have been underestimated. However, this study was not designed for detecting small changes (which may by themselves be significant) but to determine whether celiprolol had any clinically significant advantages over metoprolol, particularly in terms of symptoms, exercise capacity, and ejection fraction. In addition we used a wide range of well validated techniques, including the Minnesota symptom questionnaire and the six minute walk test. In two recent trials in congestive heart failure, the six minute walk test was found to provide useful and reliable information, paralleling the results obtained with formal treadmill exercise testing and changes in symptom status, and there is a clear independent inverse relation between the six minute walk test and both mortality and morbidity.22 ,35 ,36
CONCLUSIONS
In summary, in this study we have confirmed the beneficial effects of metoprolol in patients with chronic heart failure but were unable to show any significant advantages of a vasodilator β blocker over metoprolol. This would suggest that newer β blockers with additional vasodilator properties may not have significant advantages for relief of symptoms compared to metoprolol, and indicates that perhaps the most important property of these agents is the adrenergic blockade and the subsequent reduction in heart rate.
Acknowledgments
This research was supported in part by a grant from Rhone-Poulenc-Rorer.