Article Text

Statistics from Altmetric.com
A 22-year-old man presented to our District General Hospital with a 17-h history of dull central chest pain. The pain developed suddenly following weightlifting. He denied any cardiac risk factors, nor the use of illicit or performance enhancing drugs. His admission ECG demonstrated widespread ST segment changes with deep T wave inversion in the anterior chest leads. His troponin I at admission was 3.7 µg/L. An echocardiogram showed anterior hypokinaesia and he was treated with aspirin and clopidogrel and transferred to the Royal Free Hospital, London, UK for urgent coronary angiography.
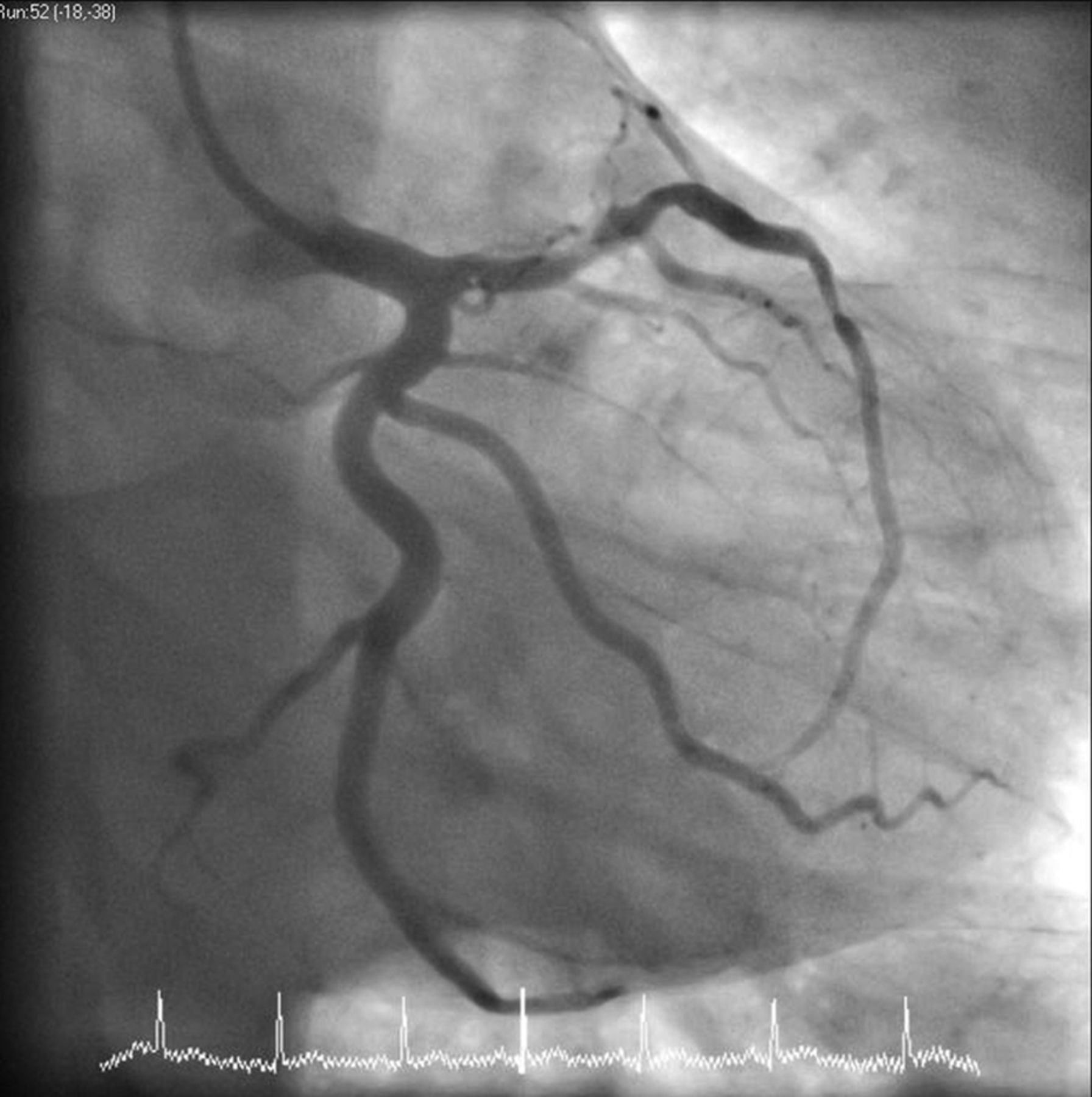
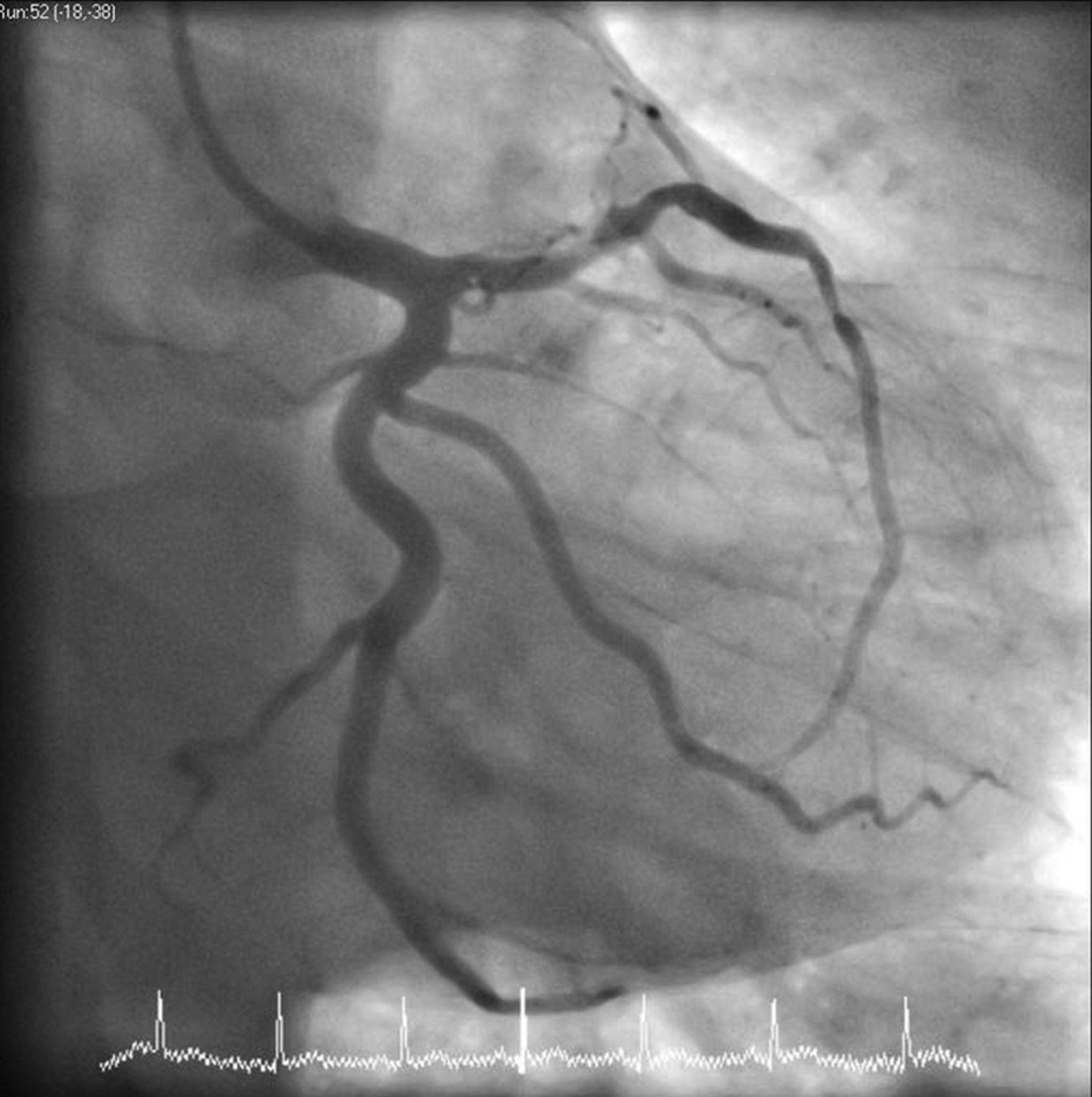
Coronary angiography demonstrated complete occlusion of the mid left anterior descending artery with other vessels normal. Primary coronary intervention was performed with aspiration of red thrombus. The lesion was dilated and a drug-eluting stent was deployed with a good result (figures 1 and 2).

Angiogram before intervention, demonstrating complete occlusion of the left anterior descending artery.
Angiogram after stent deployment, demonstrating return of flow in the left anterior descending artery.
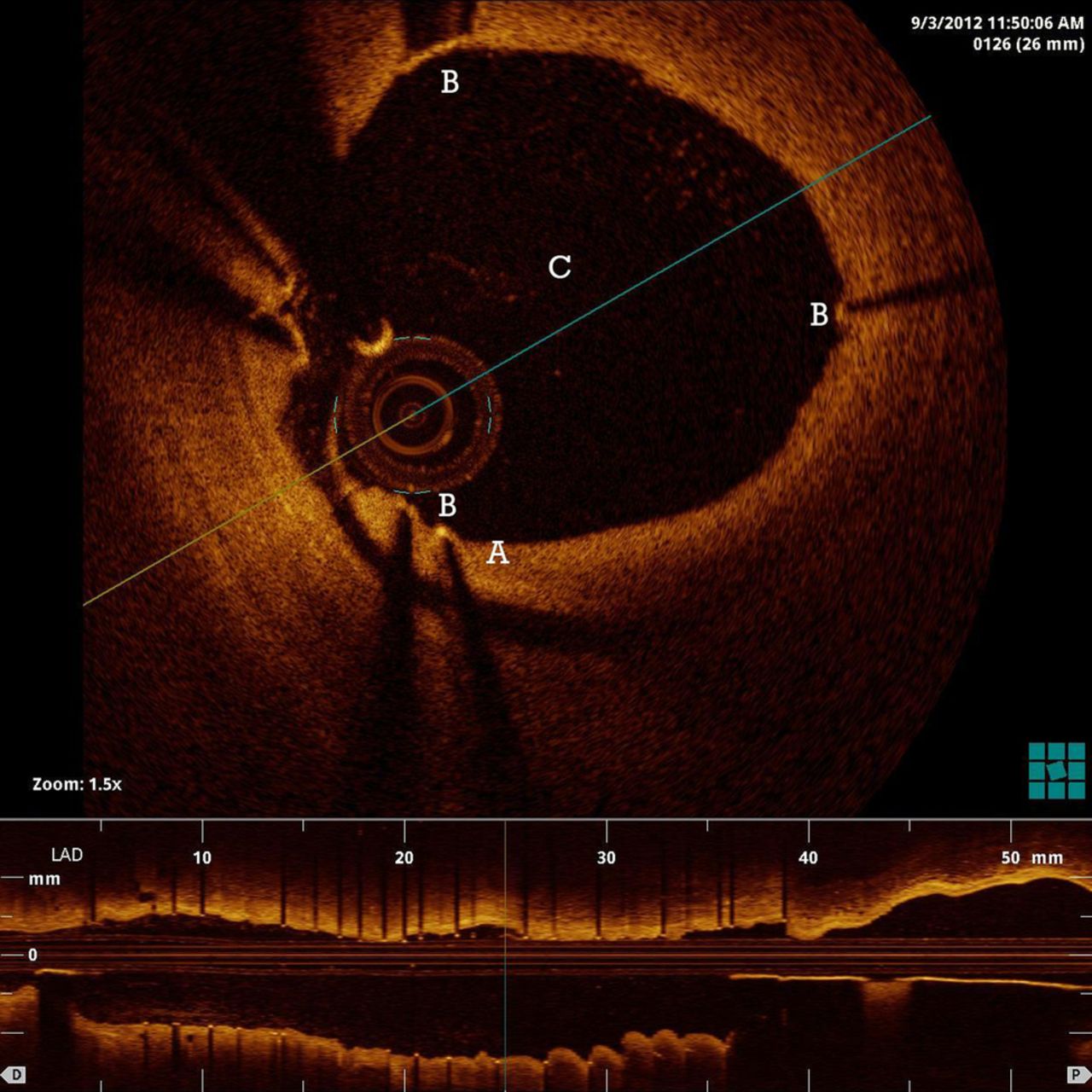
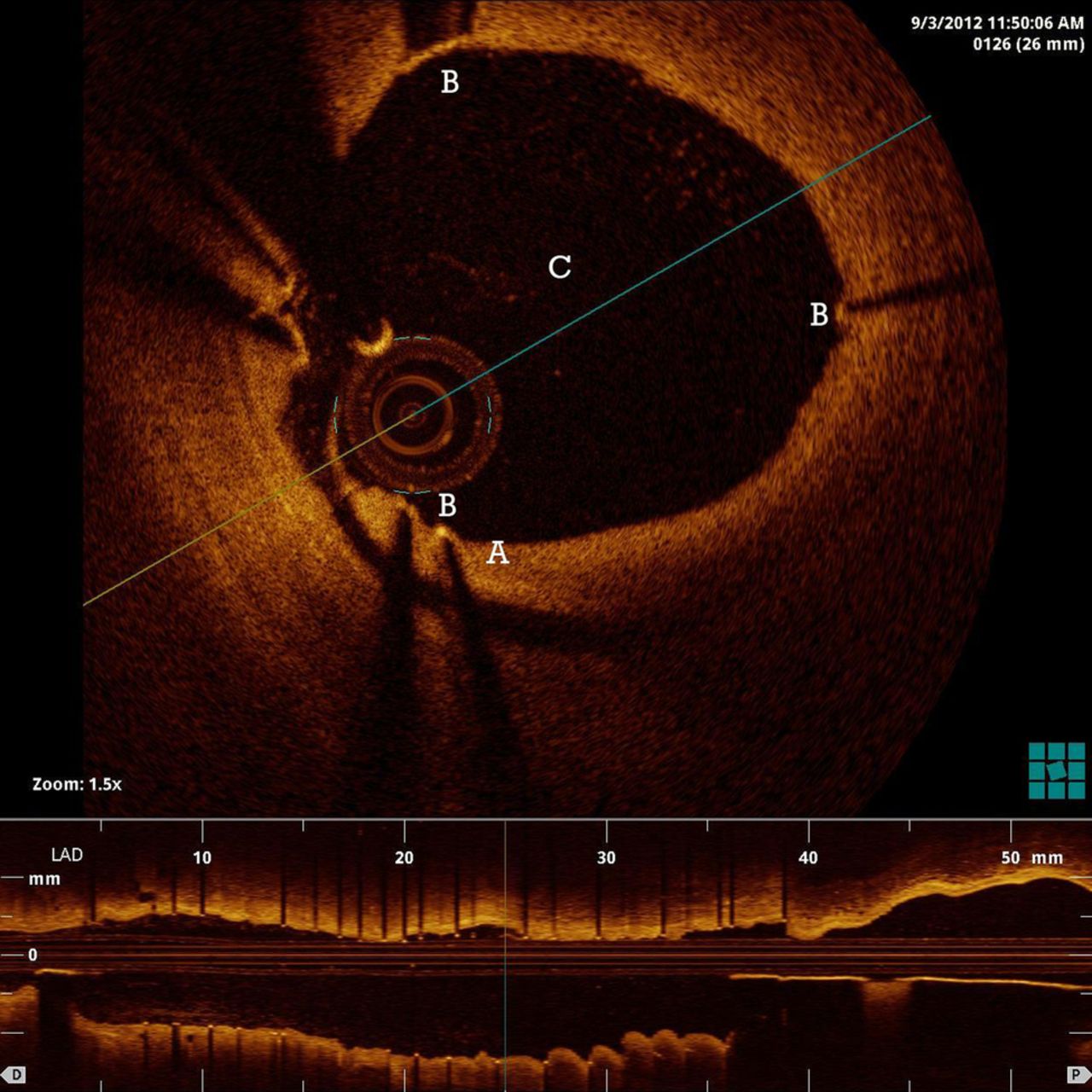
Blood tests revealed a mildly elevated total cholesterol level. A thrombophilia screen was negative. Echocardiography performed 24 h post angiography revealed preserved left ventricular function without region wall motion abnormalities. Repeat angiography with optical coherence tomography (OCT) was performed at 24 h. OCT captures µm-level resolution three-dimensional images; in this case subsurface images of the intracoronary clot and coronary artery wall were captured. A long intimal tear with an area of reduced signal in the intimal space was seen, as shown in figure 3. This is highly suggestive of coronary artery dissection.
{kind=link}
{kind=link}
{kind=link}
Optical coherence tomography image from within the left anterior descending artery after primary coronary intervention, demonstrating the intimal dissection flap (A), the struts of the deployed drug eluting stent (B) and the lumen of the artery (C).
Coronary artery dissection is rare in the population but should be in the differential diagnosis for acute coronary syndromes. OCT has emerged as a novel technique to identify underlying aetiologies in patients with cardiac issues.
Footnotes
-
Contributors ASM: coauthor and guarantor. JS: coauthor. RR: analysed and revised submission, performed angiogram with OCT image. DP: performed initial angiogram with deployment of intracoronary stent.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; internally peer reviewed.