Article Text

Abstract
Objectives The study determined the prevalence of hospitalisation due to congestive heart failure (CHF) among adult patients aged 19 years and above in the Philippines and its 17 regions in 2014. It also determined the demographic profile of these patients, aetiology and type of CHF, comorbidities, duration of hospitalisation and the overall in-hospital mortality rate.
Methods Data collection was done using the hospitalisation claims database of the Philippine Health Insurance Corporation (PhilHealth). All patient claims for CHF, that is, patients who were admitted from 1 January to 31 December 2014, were included. Descriptive statistics were utilised to obtain the results.
Results The prevalence rate was 1.6% or 1648 cases of CHF for every 100 000 patient claims for medical conditions in 2014. The mean age was 52.6±15.1 years. There was no sex predilection. Only 22.67% of the hospitalisation claims for CHF listed possible specific aetiologies, the most common of which was hypertensive heart disease (86.7%). There were more cases of systolic compared to diastolic heart failure. The mean length of hospital stay was 5.9 days (+8.2) days (median 4 days), with an overall in-hospital mortality rate of 8.2%.
Conclusions There were 16 cases of heart failure for every 1000 Filipino patients admitted due to a medical condition in 2014. Hypertension was possibly the most common aetiologic factor. Compared to western and Asia-Pacific countries, the local mortality rate was relatively higher.
- HEART FAILURE
Statistics from Altmetric.com
Introduction
Congestive heart failure (CHF) is an important public health problem, with prevalence reported to range from 1% to 12% in western countries,1 and 0.5%2 to 6.7%3 ,4 in Southeast Asian countries. It is defined as a clinical syndrome resulting from any structural or functional cardiac disorder that leads to an impaired ventricular filling or incomplete ejection of blood.1 The current three types of heart failure based on the recent revisions of the European Society of Cardiology5 are: (1) reduced with ejection fraction (EF) <40% (HFrEF); (2) preserved with EF ≥50% (HFpEF); and (3) mid-range with EF 40–49%.5–8 Although their clinical presentations are mostly the same, patients with HFrEF are more likely to be male and have coronary artery disease (CAD),1–4 ,6 ,9 ,10 while HFpEF are more likely to be female, elderly, and have hypertension.1–4 ,6 ,9 ,10 Patients with HFrEF have increased mortality and recurrent hospitalisations.7–10
The DEAR HEART Registry, a 2-year study on CHF, described the demographic profile of patients hospitalised for heart failure in six hospitals located in some urban areas in the Philippines.11 Another heart failure registry, the ADHERE Asia-Pacific study, included 722 Filipino patients (7.1% of the study population).9 Despite these studies, there are no data available regarding the prevalence of hospitalisation for CHF in the Philippines.
Currently, the most comprehensive database regarding hospitalisation claims in the country is with the Philippine Health Insurance Corporation (PhilHealth). PhilHealth is a government corporation tasked with administering the National Health Insurance Program of the country.12 Approximately nine out of 10 hospitals or healthcare facilities accredited by the Department of Health are also accredited by PhilHealth.12 ,13 As of December 2014, 87% of the projected population of the country is either a member or a beneficiary of PhilHealth.
In view of the importance of CHF, this study was conducted to estimate the prevalence of hospitalisation for CHF in the Philippines. Because of PhilHealth's wide coverage, the study used its claims database to obtain a representation of the overall hospitalisation prevalence of CHF in the country.
The general objective of this study was to determine the prevalence of CHF among adult patients aged 19 years and above who were admitted to PhilHealth-accredited hospitals in 2014, with specific objectives as follows: (1) to determine the overall and regional prevalence of CHF in the country; (2) to determine the demographic profile and comorbid conditions of patients with CHF; (3) to determine the aetiology and type of CHF; (4) to determine the duration of hospitalisation of CHF, as regard mean length of hospital stay, and length of hospital stay per region; and (5) to determine overall and regional mortality rates for all admissions of CHF.
Methodology
Study design, source of data and inclusion criteria
The prevalence of CHF was determined through a review of all records for hospitalisation for CHF for adult patients aged 19 years and above who were admitted to PhilHealth-accredited hospitals from 1 January 2014 to 31 December 2014. The data were retrieved from the anonymised records in the PhilHealth database which consisted of healthcare data from 87% of the population of approximately 99.6 million Filipinos.13 The International Classification of Diseases-10 (ICD-10) codes of the WHO were used to define the disease conditions.14 Data retrieval of CHF cases included information on the patients' demographic profile, diagnosis, comorbid conditions, aetiology of CHF (if available), specialty of attending physicians, duration of hospitalisation and condition on discharge. The regions mentioned in the PhilHealth database refer to the 17 regions of the country as of 31 December 2014 (the study period being 1 January 2014 to 31 December 2014). By 29 May 2015, the Philippine government officially added another region, that is, the Negros Island Region, thereby removing the Negros provinces from the Western (Region VI) and Central Visayas (Region VII) regions, respectively.15
Ethical considerations
The data gathering was done purely through review of anonymised PhilHealth records. There was no patient interaction. The protocol was reviewed and approved by the Institutional Ethics Committee of the De La Salle Health Sciences Institute (DLSHSI) in Dasmarinas, Cavite, Philippines.
Data analysis
The data encoding and analysis was done using Microsoft Excel 2016. Quantitative data were summarised and presented as means and SD. Qualitative data were tabulated and presented as frequency and per cent distribution.
Results
There were a total of 6 914 410 PhilHealth claims for hospitalisation for either medical or surgical causes during the time period of the study. Of these, 2 673 546 were claims for hospitalisation due to medical causes.
Of the claims for medical causes, 44 046 were due to heart failure. This represented a prevalence rate of 1.6% or 1648 cases of CHF for every 100 000 patient claims for medical causes. As illustrated in table 1, the majority of these came from Region IV-A (13.5%), National Capital Region (NCR) (10.7%), and Region III (10.3%). Patient claims without assigned regions (0.9%) were attributed to those who were admitted in non-PhilHealth accredited hospitals who were probably subsequently reimbursed in the local PhilHealth offices that may or may not have been the region where they were confined. Also shown in table 1 is the 2010 Philippine population, the latest population count done before 2014, to demonstrate the burden of the disease per region.16 The country's annual growth rate from 2010 to 2015 was 1.72%.17 The total patient claims reported above represented individual unique claims or individual patients.
Number of patients who were hospitalised for CHF and the population in the Philippines and its regions in 2014
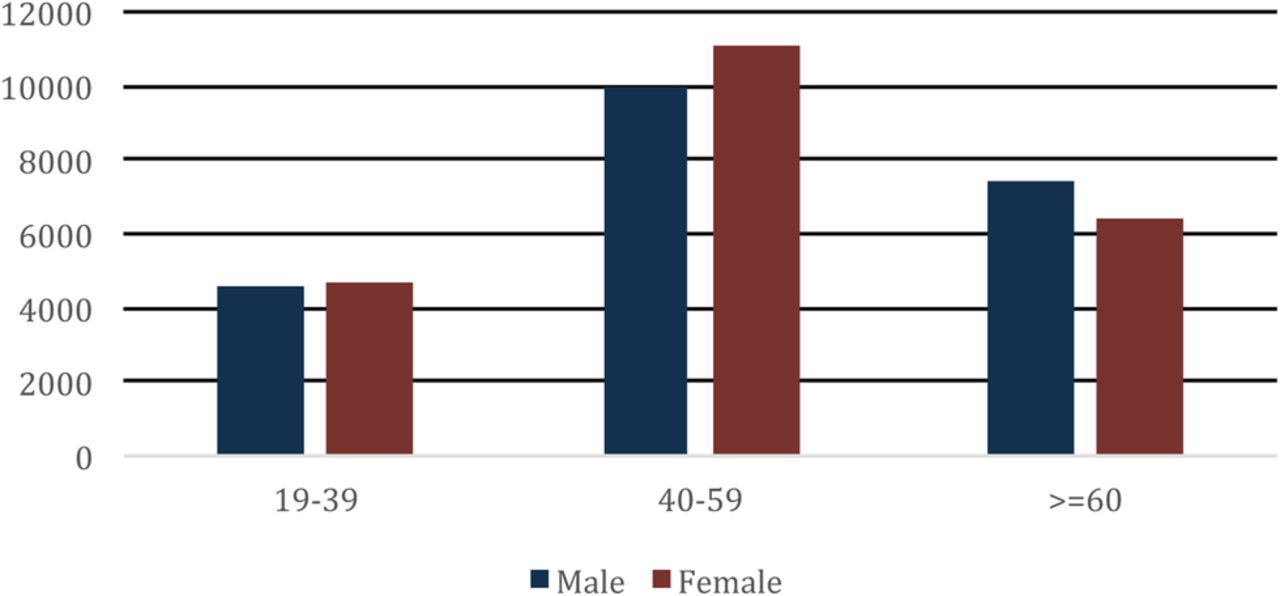
The mean±SD age of patients confined for CHF was 52.6±15.1 years old, and ranged from 19 to 114 years. Figure 1 shows patient distribution according to age and sex. Almost half of the patients, 48%, (10 008 males and 11 036 females) were in the 40–59 years age bracket. Although there was a slight preponderance of females in this group, there was no sex predilection in the total study population (49.9% males vs 50.1% females).
{kind=link}
Distribution of patients hospitalised for congestive heart failure in the Philippines in 2014 according to age and sex.
In terms of aetiologies for heart failure, only 9984 claims (22.7%) for the disease had possible specific aetiologies. In view of this, 9984 rather than 44 046 (total number of CHF patients) was used as the denominator in determining the percentage of the possible aetiologies of CHF hospitalisation. The most common possible aetiology was hypertensive heart disease, which accounted for 86.7% of the cases. The other reported possible aetiologies were rheumatic heart disease, CAD, cardiomyopathy and congenital heart disease. Possible aetiologies for CHF are listed in table 2.
Associated conditions that are possible aetiologies of CHF hospitalisation in the Philippines in 2014 (based on ICD-10 codes)
No patients were admitted for heart failure due to heart transplantation, post-procedural heart failure following cardiac surgery, or post-procedural heart failure following other surgery.
Table 3 shows the comorbid conditions of the patients who were hospitalised for CHF. Similar to table 2, the number used as the denominator was the one which represented the number of records where the comorbid conditions were indicated, that is, 9984. The most common condition was pneumonia (0.84%), followed by arrhythmia (0.53%) and diabetes mellitus (0.45%). Cardiomyopathy (2.2%) was based on the encoded ICD codes for dilated cardiomyopathy and unspecified cardiomyopathy.
Other associated conditions or comorbidities of CHF hospitalisation in the Philippines in 2014 (based on ICD-10 codes)
Most (96.3%) of the CHF records in the hospitalisation claims database did not specify the type of the patients' CHF. This leaves only 1634 (3.7%) records where the type of CHF was indicated. Of these, 1591 cases were attributed to left ventricular failure. These data on the specific type of CHF are found in table 4.
Types of congestive heart failure in the Philippines in 2014 (based on ICD-10 codes)
Because the length of hospitalisation in days had a non-normal distribution, it was expressed in median (Q1; Q3). There was not much variation in the length of hospitalisation among the regions. The median length of stay (LOS) was 4 days (Q1=3; Q3=7 days). On the other hand, the mean mortality rate was 8.1% (SD 2.45). The highest mortality rate among the regions was 12.8% and this was seen in a region located in the southern part of the country (Region XIII). The lowest mortality rate, 2.9%, was noted in a region located in the northern part of the country (Region II).
Discussion
Based on the PhilHealth data on hospital admissions, the prevalence of hospitalisation for heart failure among those admitted for medical cases in the country for 2014 was 1.6%, similar to that of western countries1 and the countries of China, Japan and Australia,4 ,18 but was lower compared to its Southeast Asian neighbours, namely Malaysia (6.7%) and Singapore (4.5%).4 The lower prevalence of heart failure in the country compared to Malaysia and Singapore might be due to two reasons: (1) difference in reporting in other countries, for example, Singapore, because they have better healthcare systems compared to the Philippines; (2) cultural and economic causes, such as deferring consultation or admission, or allocation of household budget to other needs besides health (eg, education) and foregoing the need of the patient to consult a physician or to be hospitalised.
The mean age at presentation was similar to the Philippine component of the ADHERE-Asia Pacific study (52.6 years vs 54 years)9 but was younger compared to the DEAR Heart registry (52.6 years vs 60 years).11 The ADHERE-Asia Pacific study was a registry that included 10 171 heart failure patients (722 from the Philippines) hospitalised in 43 hospitals in eight countries from the Asia-Pacific region from January 2006 to December 2008.9 The DEAR Heart registry, on the other hand, was a descriptive study among 1076 patients from six tertiary hospitals in the Philippines hospitalised from 1 November 2002 to 1 December 2004.11
The present study showed that both sexes had almost similar ages at presentation; this finding is different to previously published worldwide data, which showed that females were more likely to be older.1–5 ,8 ,10 This could be because of the shift in lifestyle and rise in the incidence of non-communicable diseases such as hypertension and diabetes,4 which were identified risk factors for heart failure. The 2012 epidemiologic study of Sy et al19 showed a lower prevalence of smoking compared to the findings of DEAR Heart study,11 but this was mainly because of a decline in male smokers, while the number of female smokers increased. There was also an increase in the prevalence of females who were obese.17 This may imply that heart failure patients would be less productive at a much earlier age compared to the national retirement age of 65 years, with an added earlier financial burden to their families.11 Other risk factors present in western countries1 ,10 and other Southeast Asian nations,4 such as diabetes mellitus, chronic kidney disease, dyslipidaemia and chronic obstructive pulmonary disease, were reported in <1% of patient claims. Rheumatic heart disease, an illness practically eradicated in developed countries, was present in 1.7% of patients, which may reflect the persistent burden of this disease in the country.
As a whole, there was no sex predilection in the occurrence of heart failure (49.9% males vs 50.1% females). There were more males than females with systolic (51.3% vs 48.7%) and diastolic (53.8% vs 46.1%) heart failure, but among those with combined systolic and diastolic heart failure the number of males and females were equal. Differences from the worldwide trend might be because the majority of patient claims were encoded as plain heart failure (I50) or heart failure, unspecified (I50.9). Other reasons might include an increasing number of risk factors brought about by negative lifestyle changes on both sexes, such as smoking and a sedentary lifestyle.4
Hypertension and CAD were seen to be common risk factors worldwide.1–4 ,6 ,9 ,10 HFpEF patients were mostly hypertensive, while HFrEF patients mostly had CAD.1–4 ,6 ,8–10 CAD as the major underlying cause of CHF was also seen in the DEAR Heart registry.11 This was not observed in the current study based on the PhilHealth database, where atherosclerotic heart disease was reported in only 0.3% of cases. Instead, the current study showed hypertension as a common aetiology of CHF, similar to the findings of a recent paper by Reyes et al20 on heart failure in Asia, where the prevalence of hypertension was higher compared to CAD. Since most claims with encoded aetiology did not have any data on whether they had systolic and/or diastolic heart failure, similarities or differences to international patterns regarding systolic or diastolic heart failure could not be inferred.
One aspect that might have a direct impact on patient management and economic burden was the duration of hospitalisation of these patients. A paper in 2007 on the epidemiology of heart failure in western countries showed a declining average LOS from 21.1 days during the 1980s to 12.9 days during the latter part of the 1990s.10 An epidemiologic study in 2015 showed an improved LOS in western countries (4.2 days).4 However, the same paper showed that Southeast Asian countries still have a longer LOS of 6 days.4 The DEAR Heart registry showed a mean LOS of 10 days (median LOS 7 days).11 Although the current study showed that the nationwide overall mean LOS was about 40% lower (mean 5.9 days, median 4 days) compared to the DEAR Heart registry, the population of the latter study was mostly from the NCR rather than nationwide. Current data showed that LOS in the NCR was longer at 7.2 days, although still 30% lower than that of the DEAR Heart registry.11 The longer LOS might be reflective of more complicated cases being managed in the NCR compared to other areas of the country. NCR contains many of the tertiary centres where patients from the other regions are referred to or transferred to for further management.
International data demonstrated a decreasing trend in mortality among patients with heart failure.1 ,4 ,10 Although the current local data showed an improvement in the overall mortality rate of 8.2% compared to that seen in the DEAR Heart registry (10%),11 this was still high compared to its Asia-Pacific neighbours (4.8%)9 and the USA (3.0%).6 The relatively high mortality might have been due to any of the following:
Differences in facilities used in the management of these patients. Tertiary hospitals in developed countries are equipped with state-of-the-art equipment, and are better staffed. In comparison, tertiary hospitals are poorly distributed in the country with most hospitals in the urban cities, with the less equipped secondary and primary healthcare facilities left to those in the rural areas.
Healthcare delivery through out-of-pocket expenses. In many western countries, healthcare is primarily subsidised or provided by the government. In contrast, healthcare is mostly obtained through out-of-pocket expenses locally.21 Because of economic constraints, some patients consult late in the course of the disease thereby increasing the chance of having concomitant complications. Ironically, when complications pile up and LOS extends, most marginalised patients have difficulty sustaining financial support for the medical treatments necessary to improve patient survival.
Study limitations
There were several limitations to the study. (1) The final diagnosis written in the PhilHealth form for encoding might not have always been present, that is, the encoder might have had to search for the ICD 10 codes of the diagnosis, or it might not have been complete. As such, the aetiology and type of heart failure, and the comorbidities, might not have been properly encoded. (2) In describing whether the disease entity was either a comorbidity or an aetiology (such as hypertensive heart disease, ischaemic heart disease, rheumatic heart disease), some assumptions were made based on the ICD 10 codes used. Also, all the comorbidities might not have been included because PhilHealth's coverage policy is only for two disease entities per hospitalisation (final diagnosis and one comorbidity). Therefore, there might be underestimation of the prevalence of comorbidities. (3) The possibility of human error during database encoding could not be discounted. (4) PhilHealth's policy and non-coverage of re-admissions for the same disease condition within a 90-day period (excluding the highly unlikely event of the benefit payment not being fully consumed) have made the determination of re-admission rates for CHF improbable. The extent of the effects of each limitation to potential bias, however, would be difficult to gauge. Moreover, the extent of the error in estimation is difficult to estimate.
Conclusions
For every 1000 Filipino patients admitted due to a medical condition during 2014, 16 cases were because of heart failure. The age at presentation was younger compared to previously published local data, but was similar in age compared to the latest international study. There was no gender predilection. Hypertension was possibly the most common aetiologic factor. Although overall length of hospital stay was shorter compared to western and Asia-Pacific countries, mortality rate was still relatively high.
Key messages
What is already known about this subject?
Congestive heart failure is widely studied in developed countries. In the Philippines, there was one study regarding its demographics and this was done more than 10 years ago, although it was published in 2007. This study involved a few hospitals located in the national capital region of the country. In 2006–2008, about 700 Filipino patients were included in a registry of heart failure patients in the Asia-Pacific region.
What does this study add?
As the current study involves hospitals nationwide, it gives a more encompassing picture of the prevalence of the hospitalisation due to heart failure, its demographic profile as well as the current in-hospital mortality rate in the country. The present study can also serve as a basis for the determination of the economic impact of heart failure in the Philippines.
How might this impact on clinical practice?
Both the prevalence and economic study might be used for developing guidelines and policies to improve the clinical and financial support for patients hospitalised for heart failure in the Philippines.
Acknowledgments
The authors wish to acknowledge the help of Ms Jenna M Gonzalez and Mr Paulus Magnus Bacud, Planning Officer III, PhilHealth CorPlan, in the collection of vital data for this study.
Footnotes
Contributors All authors have contributed to the protocol development. BATM and AB-DS polished the protocol, monitored the collection of data, prepared the draft of the paper and did revisions before submission to Heart Asia. VLM cleaned and analysed the data, as well as contributing to the writing/revision of the drafts. FEP reviewed the draft of the paper before submission for possible publication and gave important input. NSP, RBN, LAS and RN also contributed to the data collection. BAT-M is the guarantor. All authors have given approval to this version for publication.
Funding Funding was through a research grant to De La Salle Health Sciences Institute, Dasmarinas, Cavite by Novartis Healthcare Philippines, Inc. The sponsor did not interfere in the any part of the development of the paper.
Competing interests None declared.
Ethics approval Institutional Ethics Committee, De La Salle Health Sciences Institute.
Provenance and peer review Not commissioned; externally peer reviewed.