Article Text

Abstract
Valvular heart disease is a growing public health problem, with an increasing prevalence due to an ageing population. Despite advances, the medical management of symptomatic valvular heart diseases remains suboptimal, necessitating surgical correction. The challenge remains in identifying an asymptomatic or mildly symptomatic patient who will benefit from timely surgery before irreversible changes in cardiac function have occurred. The potential risks of surgery versus watchful expectancy require careful decision-making. This review is a focused update on the existing guidelines and identifies the knowledge gaps and avenues of future research in the management of patients with valvular heart diseases
Statistics from Altmetric.com
Valvular heart disease is a major public health problem with prevalence estimates of 2.5% in the general population and up to 11.7% in those above 75 years of age.1 With the ageing population, the relative burden of valvular disease is expected to increase. Unfortunately, not only is this problem under-recognised as a public health concern, but management protocols in valvular heart disease are not as clearly defined as that for other cardiac problems. Despite advances in surgical management and the introduction of less invasive techniques, there is controversy regarding the optimal timing of a corrective surgery. In the absence of contraindications the symptomatic patient clearly qualifies for surgical intervention, but it is the asymptomatic patient that poses a dilemma. On the one hand, the development of symptoms and cardiac remodelling portend a poor prognosis and argue for an early corrective management approach. On the other hand, subjecting an asymptomatic patient to a risky procedure is equally debatable. The ensuing sections of the manuscript provide separate discussions on management of each of the valvular lesions, collating existing evidence and evolving concepts.
Aortic stenosis
Aortic stenosis (AS) results from postinflammatory or degenerative or atherosclerotic disease affecting either a normal tricuspid valve or a congenitally malformed bicuspid or unicuspid valve.2 The prognosis for asymptomatic patients with aortic stenosis may be similar to age- and gender-matched populations.3 However, most of these patients will develop symptoms within 5 years with a rapidly declining prognosis.4 5 Patients with symptoms have a clear indication for aortic valve replacement (AVR). Because of the difference in prognosis between asymptomatic and patients with symptoms with aortic stenosis, one recommendation would be to closely follow asymptomatic patients to symptom development before surgical intervention. Close follow-up should include aggressive treatment of hypertension, possibly the use of statins to delay AS progression. The latter intervention remains controversial and is being studied in two large, multicentre, double-blinded, randomised clinical trials.6 7
Pre-emptive AVR could theoretically prevent the development of symptoms and also reduce the progression of cardiac remodelling that occurs as a compensatory mechanism due to the haemodynamic obstruction from the aortic stenosis. Operating on a patient with relatively preserved myocardial function might also be potentially beneficial, as myocardial dysfunction is a predictor of heart failure and death after AVR.8 Recent data suggest that an elevated pulmonary artery systolic pressure increases perioperative risk in patients undergoing AVR.9 Furthermore, AS with a preserved ejection fraction (EF) but reduced cardiac reserve also portends a higher risk.6 The potential downside is to subject an asymptomatic patient to the immediate perioperative risk of surgery and the more long-term risks of thromboembolism, endocarditis and anticoagulation-related bleeding. The average risk of mortality for AVR in experienced centres is 1–2%.10 This makes it critical to identify the subgroup of patients with asymptomatic aortic stenosis in whom the risk of pre-emptive AVR will be outweighed by the potential benefits from the surgery.
There are some indicators that predict symptom development and worse prognosis in patients with aortic stenosis, and may help guide management. Patients with peak aortic jet velocity ⩾4.5 m/s are more likely to develop symptoms compared with patients with aortic jet velocity <4.5 m/s.4 Furthermore, a progressive decrease in aortic valve area increases the likelihood of developing symptoms by a relative risk of 1.26 for each 0.2 cm2 in valve area. The aortic jet velocity and the rate of change of aortic jet velocity also predict clinical outcome.4 11 No single echocardiographic parameter can predict the time course of symptom onset.6 Exercise stress testing in patients with asymptomatic aortic stenosis has some prognostic value. Symptom-limited exercise stress testing predicts a symptom-free survival of 49% compared with a symptom-free survival of 89% in patients who do not develop symptoms during an exercise stress test.12 Moreover, exertional dizziness has been suggested to be a better prognosticator during stress testing than angina or dyspnoea.12 In general, event-free survival is expected to be better in patients with negative exercise stress test.13 Thus, exercise stress testing seems to be a reliable method to guide clinical decision-making in patients with asymptomatic aortic stenosis. Assessment of the extent of aortic valvular calcification has also been used for risk stratification. Quantitative assessment by electron beam computed tomography (EBCT) seems to have value in predicting event-free survival.14 Routine use of EBCT may have potential clinical value and should be considered for incorporation in future clinical guidelines iterations.
Current ACC/AHA guidelines recommend AVR surgery for asymptomatic patients with left ventricular ejection fraction (LVEF) <50% and for patients undergoing coronary artery bypass grafting (CABG), aorta or other valve surgery.10 Other clinical indicators favouring surgery include development of symptoms or a drop in blood pressure during exercise stress testing and non-invasive markers of rapid progression of AS. Figure 1 suggests an approach in the management of these patients based on ACC/AHA and the European Society of Cardiology guidelines.6 10 15

Stepwise evaluation of patients with severe aortic stenosis (AS) on the basis of American College of Cardiology/American Heart Association and European Society of Cardiology recommendations. Levels of evidence are provided in parentheses. Reproduced with permission from Dal-Bianco et al.6 AVA, aortic valve area; AVC, aortic valvular calcification; AVR, aortic valve replacement; BNP, brain natriuretic peptide; BP, blood pressure; CABG, coronary artery bypass grafting; CAD, coronary artery disease; CR, contractile reserve; EBCT, electron beam computed tomography; LV, left ventricle; LVEF, left ventricular ejection fraction.
Aortic balloon valvulotomy currently is recommended as a palliative procedure only for patients with severe symptomatic aortic stenosis who cannot undergo surgery due to comorbidities or as a bridge to AVR in haemodynamically unstable patients.10
The benefits are mainly symptom-related and short-lived, with restenosis and clinical deterioration occurring in most patients. A future role for balloon valvulotomy for management of high-risk asymptomatic AS adult patients is unclear. Percutaneous aortic valve replacement is an emerging therapeutic strategy that can also be considered. This is reserved for patients with symptoms only at this stage.
Open aortic valve replacement is the current treatment of choice for symptomatic aortic stenosis. However, due to the presence of advanced age and comorbidities, almost 30–60% of eligible patients are deemed to be at too high a risk for conventional surgery.16 A transcatheter approach of delivering a balloon expandable stented valve (Edwards Sapien Transcatheter Heart Valve; Edwards Lifesciences, Irvine, California) in such patients has been shown to be feasible in early studies.16 A randomised prospective controlled trial is under way, comparing the outcomes after deployment of the Edwards Sapien Transcatheter Heart Valve with optimal medical management.16
Mitral regurgitation
Mitral regurgitation can be organic, due to structural defects of the valvular and/or of the chordal apparatus, or functional, due to dilatation of the left ventricle and annulus with increased tethering forces restricting proper valve closure. The aetiology for organic mitral regurgitation includes mitral valve prolapse (MVP), rheumatic heart disease, infective endocarditis, certain drugs and collagen vascular diseases. The aetiology of functional mitral regurgitation usually relates to CAD or dilated cardiomyopathy.
Mitral regurgitation can present acutely, in the setting of chordal rupture from infective endocarditis, or from papillary muscle ischaemia or infarction. The management of these patients is almost always emergency surgery.
The more common chronic form of mitral regurgitation (MR) can remain asymptomatic for many years; as a compensatory mechanism, the left atrium increases in size, accommodating regurgitant blood flow without any significant increase in left atrial pressure and preventing symptoms of pulmonary congestion. The compensated phase of mitral regurgitation may last for many years. The ensuing left ventricular remodelling eventually results in left ventricular contractile dysfunction, leading to further dilatation, elevated filling pressures and worsening the MR. The 10-year natural history of the disease is associated with excessive morbidity and mortality and 90% of the patients die or require surgery.17 Quantitative classification of regurgitation according to the regurgitant volume and effective regurgitant orifice has been shown to independently predict the clinical outcome. In a study by Sarano and colleagues from the Mayo Clinic, patients with an effective regurgitant orifice of at least 40 mm2 were seen to have a 5-year survival rate that was lower than expected on the basis of US Census data. This study suggested that patients with an effective regurgitant orifice of at least 40 mm2 should be considered for cardiac surgery.18 Factors associated with poor prognosis and thus qualifying a patient for surgery include ejection fraction less than 60% and NYHA class III–IV symptoms. Notably severe symptoms also portend a worse prognosis postoperatively.
A dilemma when considering patients with combined mitral regurgitation and left ventricular dysfunction for surgery is deciding on whether the mitral regurgitation is a result of left ventricular remodelling or whether myocardial dysfunction is the result of chronically elevated preload due to mitral regurgitation. In the latter case, surgery seems to be beneficial, even in the face of moderate to severe left ventricular dysfunction if the underlying chordal architecture can be preserved.19 The mitral valve surgery has less clear benefits in patients with primary cardiomyopathy leading to mitral valvular regurgitation, but in select patients the procedure may be promising.20
The ACC/AHA guidelines recommends surgery for patients with symptoms with an EF >30% or an end-systolic dimension <55 mm.10 Asymptomatic patients should be operated on if the EF is between 30 and 60% or the end-systolic dimension is >40 mm. The experience of the surgical centre and the operability of the valvular defects play a major role in deciding on the appropriate management strategy. In cases where the anatomy of the defect and experience of the centre lend themselves to repair, other “softer” criteria may be considered. These include asymptomatic patients with chronic severe mitral regurgitation and left ventricular ejection fraction >60% and end-systolic dimension <40 mm. The presence of new-onset atrial fibrillation and severe pulmonary hypertension also constitutes a relative indication for surgery when the likelihood of surgical repair is high.
Asymptomatic patients should be followed with history, physical examination and echocardiography every 6–12 months.10 Exercise stress testing can be useful in patients who are poor historians or have equivocal symptoms.10
In chronic ischaemic mitral regurgitation, repair of the valvular closure mechanism is more complex. The performance of CABG by itself may relieve mitral regurgitation in some patients, but in severe cases concomitant MVR surgery might be indicated.21
The role of medical management in mitral regurgitation is not well established. Beta blockers and ACE inhibitors in the case of primary left ventricular dysfunction leading to mitral regurgitation are effective in reducing the severity of the mitral regurgitation.22 23 The emerging role of cardiac resynchronisation when used as indicated in advanced cardiomyopathy incidentally shows an improvement in the severity of MR.24 Multiple promising percutaneous mitral repair strategies are emerging for patients who cannot undergo conventional surgery, and these need to be studied further before practical application is a reality.25
Aortic regurgitation
Aortic regurgitation (AR) can be due to valvular or aortic root disease. The commonest aetiology of AR is seen with a congenital bicuspid aortic valve or degenerative aortic diseases like annuloaortic ectasia.26 Rheumatic heart disease continues to be an important cause of aortic regurgitation in the developing world.26
Aortic regurgitation can develop acutely as a complication of infective endocarditis, aortic dissection or trauma. It generally presents with acute haemodynamic failure and constitutes a medical emergency requiring emergency surgery.
The prognosis of severe chronic aortic regurgitation is poor.27 Symptom development in the form of dyspnoea or angina is associated with worse outcomes. The presence of symptoms classified as New York Heart Association (NYHA) and Canadian Cardiovascular Society (CCS) class III or IV is associated with an annual mortality of up to 25%.27 This subgroup of patients has a definite indication for surgical intervention. There is some evidence that even patients with milder symptoms at NYHA or CCS class II also may benefit from surgery.28 Patients with equivocal symptoms on history that become manifest on exercise stress testing are also candidates for AVR.
The asymptomatic patients as a group do not carry a higher risk of death compared with the general population.27 29 The subgroup of asymptomatic patients with left ventricular dysfunction, with an end-systolic diameter of greater than 25 mm/m2 of body surface area or an EF <55% do face an increased risk of death.27 In these patients, a delay in surgery while awaiting symptom development is associated with a significant risk of postoperative myocardial dysfunction and death.30 Echocardiographic quantitation of AR severity and indexed end-systolic volume provides an independent prediction of clinical outcome in asymptomatic patients. Asymptomatic patients with severe AR and indexed end-systolic volume ⩾45 ml/m2 versus have been shown to have a higher cardiac event rates in comparison with those with indexed endsystolic volume <45 ml/m2 (10 years: 87 (SD 8)% vs 40 (10)%, p<0.001).31 In addition, a lower ejection fraction is also associated with a poorer postoperative outcome.32 However, this should not automatically exclude patients with a low EF, as these patients can gain a significant improvement in EF postoperatively with reduction in afterload.32
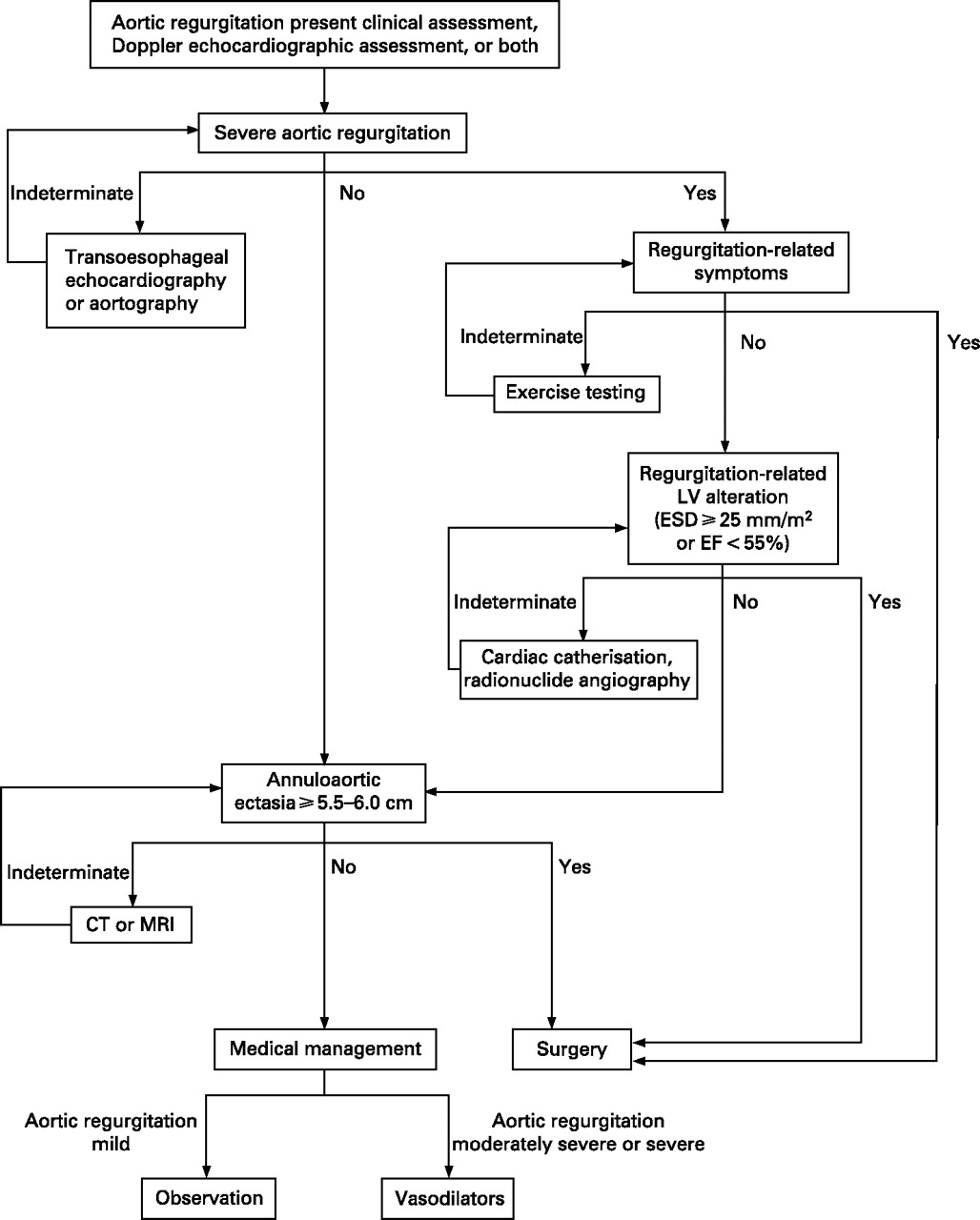
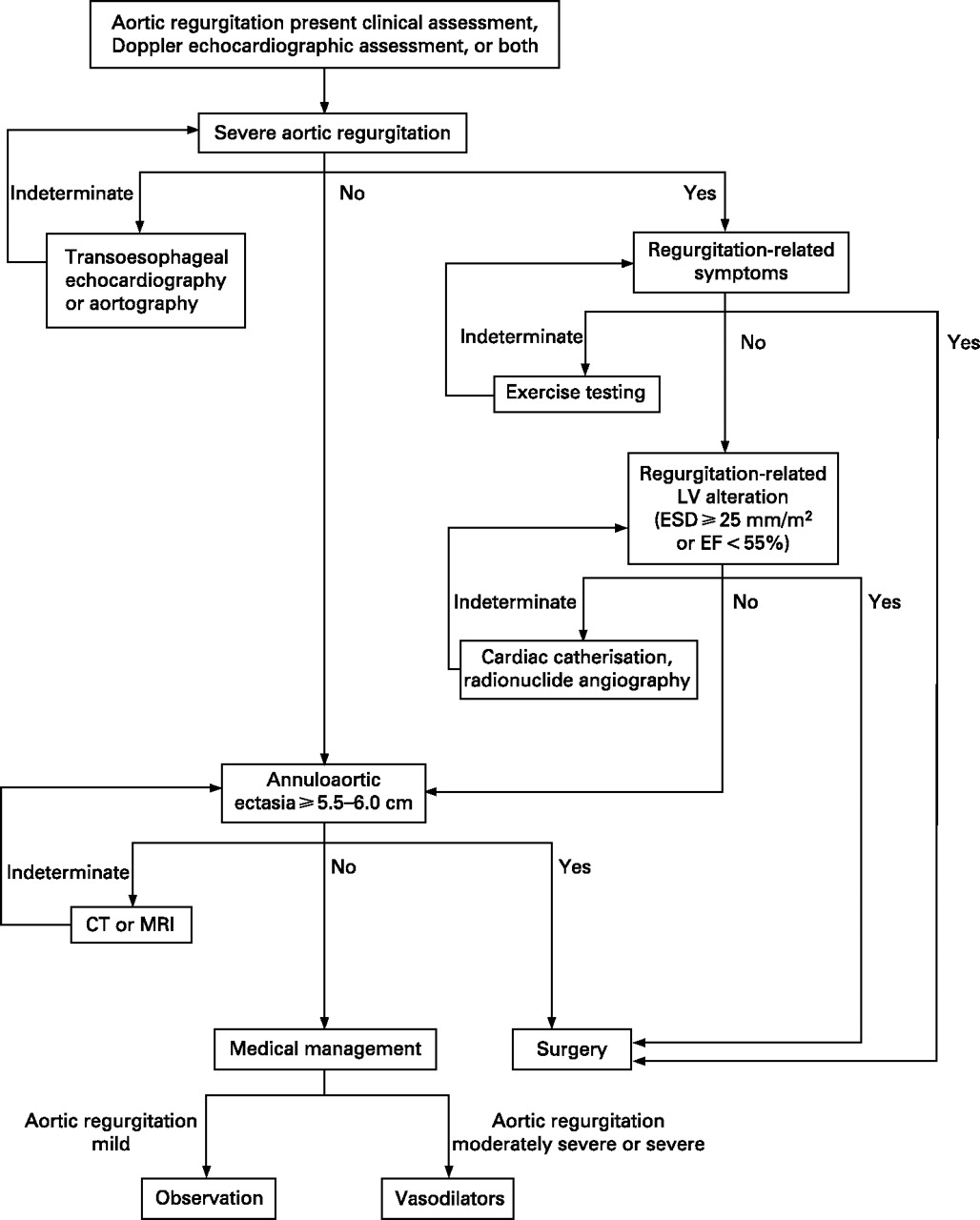
An end-diastolic dimension of >75 mm is also an ACC/AHA indication for AVR. AVR is also indicated in patients with asymptomatic chronic AR who are undergoing other cardiac surgery on another valve, aorta or CABG. A suggested plan for optimal management of AR is shown in fig 2.
{kind=link}
{kind=link}
Management algorithm for patients with aortic regurgitation. Reproduced with permission from Enriquez-Sarano and Tajik.34 EF, ejection fraction; ESD, end-systolic diameter; LV, left ventricle; LVEF, left ventricular ejection fraction.
The option of medical management is reserved either for patients with symptoms who are deemed to have an excess surgical risk or for asymptomatic patients in whom it is desirable to delay operation. The mainstay of treatment is vasodilator therapy with nifedipine and ACE inhibitors.33 34 Patients with Marfan syndrome and aortic root dilatation require lifelong beta-blocker therapy to reduce the likelihood of aortic dissection.
Sinus of Valslava aneurysms are congenital malformations of the connective tissue suspending the aortic cusps. It is commonly associated with aortic regurgitation. Repair of the sinuses can result in an improvement in the severity of AR, but more often than not surgical management of the aortic valve is needed at the same time.35
Mitral stenosis
Worldwide, the major cause of mitral stenosis is rheumatic heart disease, in which valvular inflammation leads to thickening, calcification and commissural fusion followed by obstruction. Mitral stenosis is an indolent, slowly progressive disease, and even after symptom development, it may take up to 10 years for the disease to become disabling.36 The 10-year survival for asymptomatic or minimally patients with symptoms is up to 80%; with development of disabling symptoms, this drops to up to 15%, and in the presence of pulmonary hypertension the mean survival is only 3 years.36 37
Symptomatic patients do automatically qualify for surgery due to the above reasons. Hence, earlier correction is helpful in avoiding the development of significant pulmonary hypertension. Also, unlike the aortic valve management, the procedure of choice for mitral valve correction is percutaneous mitral balloon valvulotomy if the anatomy is suitable. The second and third preferred approaches are surgical mitral valve repair and mitral valve replacement respectively.10
The medical management of mitral stenosis focuses on increasing ventricular filling duration by increasing the diastolic filling period by judicious use of beta blockers. Salt restriction and diuretics also constitute important elements in the symptomatic management of patients with MS.
Tricuspid and pulmonary valve disease
Tricuspid regurgitation (TR) is the most common pathology of the tricuspid valve, and in contradistinction to the left-sided cardiac valves, this condition is usually a sequel to chronically elevated right ventricular systolic or diastolic pressures.26 Causes of primary valvular abnormality leading to regurgitation include rheumatic heart disease, infective endocarditis, drug-induced, carcinoid syndrome, and external or internal trauma to the valve. Tricuspid regurgitation is a common complication after cardiac transplant and secondary to trauma from repeated endomyocardial biopsies.38 39 TR can also occur as a complication to permanent pacemaker or ICD placement.40
Tricuspid regurgitation is well tolerated in the absence of pulmonary hypertension. The presence of pulmonary hypertension either as the initial cause of tricuspid regurgitation or as a secondary event leads to manifestations of right heart failure, with ascites, congestive hepatomegaly and anasarca. The prognosis of tricuspid regurgitation depends on the underlying pathology that led to the development of the tricuspid regurgitation—for example, the improvement in pulmonary vascular pressures after mitral valve surgery will often lead to correction of the tricuspid regurgitation.10 However, if the tricuspid regurgitation persists even after relief of pulmonary hypertension, surgery could be attempted, but results are inconsistent.41 For rheumatic valve disease, surgery may be unavoidable, and repair seems to be the preferred approach over replacement.42 Similarly tricuspid regurgitation caused by flail leaflets is associated with excess mortality and high morbidity. Tricuspid valve repair can often be performed with low risk, allowing symptomatic improvement.43
Similar to tricuspid valve disease, the most common pathology affecting the pulmonic valve is regurgitation secondary to pulmonary hypertension. The correction of underlying cause of pulmonary vascular hypertension like mitral valvular disease can ameliorate pulmonic regurgitation. Surgical management of the valve itself is reserved almost entirely for congenital causes affecting the valve.
Future directions
Acquired valvular heart disease in the Western world is mainly a disease of older people who have several comorbidities, complicating their management. In one study from Europe, almost a third of qualifying patients with severe symptomatic single valve disease did not undergo surgery due to comorbidities.44 Older age, low EF and previous sternotomy are only some of the factors which preclude these patients from obtaining the benefits of surgery.45 In developing countries, expense and resources required for conventional valvular surgery also call for shorter, less invasive surgical techniques. Fortunately, several advancements are on the horizon. These new developments include the use of less invasive techniques like minithoracotomy and the use of small port access, which avoids full sternotomy and cardiopulmonary bypass, thus allowing surgery on a beating heart. Non-surgical techniques like percutaneous valve surgery remain an area of extensive research. One of the major limitations is the use of a stiff, relatively large valve system through a potentially atherosclerotic peripheral vascular system. However, with scientific ingenuity, it is not difficult to contemplate a major future role for this approach for valvular surgery, at least for high-risk patients. It is foreseeable that in the near future, technological advancements in safer valvular repair will tilt the management algorithms towards early surgical intervention for patients with valvular disease. Similarly, development of novel markers may identify specific subgroups of patients who can safely be watched without being subjected to surgery.
References
Footnotes
Competing interests None.