Article Text

Abstract
Objective Estimate the incidence and outcomes of in-hospital cardiac arrest (IHCA) in a tertiary-care hospital in Abu Dhabi emirate, United Arab Emirates (UAE).
Methods Retrospective data from 685 inpatients who experienced an IHCA at a hospital in Abu Dhabi (UAE) between 1 January 2013 and 31 December 2015 were analysed. Sociodemographic variables were age and gender, and IHCA event variables were shift, day, event location, initial cardiac rhythm and the total number of IHCA events. Outcome variables were the return of spontaneous circulation (ROSC) and survival to discharge (StD).
Results The incidence of IHCA was 11.7 (95% CI 10.8 to 12.6) per 1000 hospital admissions. Non-shockable rhythms were 91.1% of the cardiac rhythms at presentation. The majority of IHCA cases occurred in the intensive care unit (46.1%) and on weekdays (74.6%). More than a third (38.3%) of patients who experienced an IHCA achieved ROSC and 7.7% StD. Both ROSC and StD were significantly higher in patients who were younger and presenting with a shockable rhythm (all p’s≤0.05). Survival outcomes were not significantly different between dayshifts and nightshifts or weekdays and weekends.
Conclusions The incidence of IHCA was higher and its outcomes were lower compared with other high-income/developed countries. Survival outcomes were better for patients who were younger and had a shockable rhythm, and similar between time of day and days of the week. These findings may help to inform health managers about the magnitude and quality of IHCA care in the UAE.
- heart arrest
- in-hospital cardiac arrest
- myocardial infarction
- resuscitation
- survival
- United Arab Emirates
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
- heart arrest
- in-hospital cardiac arrest
- myocardial infarction
- resuscitation
- survival
- United Arab Emirates
Key messages
What is already known about this subject?
In-hospital cardiac arrest (IHCA) is a major cause of morbidity and mortality in healthcare settings, contributing to 80% of in-hospital mortality rates worldwide.
What does this study add?
The United Arab Emirates (UAE) is a young country with a rapidly developing healthcare system coupled with a youthful population that has high rates of chronic diseases, especially diabetes and cardiovascular disease.
While there is a growing body of research on the epidemiology of out-of-hospital cardiac arrests in the UAE and Gulf countries, this is the first study to estimate the incidence and outcomes of IHCA in the UAE.
The incidence of IHCA in the UAE was higher than other developed countries but survival to discharge was two times lower compared with Europe and North America.
How might this impact on clinical practice?
This paper provides novel and current data on the epidemiology of IHCA that may help to inform health managers and stakeholders about the magnitude and quality of IHCA care in the UAE.
Survival outcomes did not differ by shift or days of the week in our study and the quality of in-hospital post-arrest care needs to be standardised throughout the 24-hour and 7-day cycle in all UAE healthcare facilities.
Introduction
In-hospital cardiac arrest (IHCA) is a major cause of morbidity and mortality in healthcare settings globally. Approximately 1–5 patients per 1000 hospital admissions experience an IHCA worldwide1 contributing to 80% of in-hospital mortality.2 In the USA, approximately 209 000 adult cases and 6000 paediatric cases of IHCA are reported every year.3 Despite advancements in resuscitation technology and care, survival outcomes following IHCA remain low at 15%–25%,4 and vary drastically between 0% and 42% worldwide.1 Research shows that various patient and healthcare-related factors are associated with the survival outcomes of IHCA.1 Major patient-related factors are age, gender, initial cardiac rhythm, underlying medical condition, comorbidities and time of the IHCA event, whereas major healthcare-related factors are policies and protocols for IHCA care, duration and method of resuscitation, skills of healthcare professionals, response time of the emergency response team and location/hospital unit of the IHCA event.1 2
Evidence suggests that improving the quality of resuscitation care and minimising other healthcare-related risk factors can remarkably increase survival outcomes and recovery from IHCAs.4 5 Reliable and updated estimates of the burden and outcomes of IHCA are vital for monitoring and improving the delivery and quality of IHCA care in any healthcare setting. In the United Arab Emirates (UAE), studies have shown low survival rates (1%–2%) from out-of-hospital cardiac arrest.6 However, unlike European countries and the USA, the epidemiology of IHCA is unknown in the UAE, signifying the need for research in this area. Therefore, this study aimed to provide the first estimates of the incidence, characteristics and outcomes of IHCA at a tertiary-care hospital in the UAE.
Methods
Study design
Retrospective data analysis was performed on patients who experienced an IHCA event between 1 January 2013 and 31 December 2015.
Study setting
Data were obtained from a large 400-plus bed tertiary-care public hospital with over 30 specialty departments located in the emirate of Abu Dhabi, UAE. Each hospital unit was equipped with an emergency trolley (crash cart) that contained all necessary equipment, medications and defibrillators for resuscitating patients with cardiac or respiratory arrest. The hospital resuscitation policy was aligned with the American Heart Association (AHA) 2015 guidelines.7 The hospital had a medical emergency response team (MERT) that provided resuscitation treatment and care. The team consisted of an intensivist, an intensive care unit (ICU) nurse, a respiratory therapist, a nurse supervisor, a medical physician for adult cases and a paediatrician for paediatric cases. All members of the MERT were certified in Basic Life Support and Advanced Cardiovascular Life Support for adults and Paediatric Advanced Life Support for infants and children. The MERT was only called for medical emergencies that involved cardiac arrest and/or respiratory arrest. The MERT was called when a patient was found unresponsive, whether witnessed or unwitnessed, with no pulse and not breathing or gasping for air. Any healthcare provider could activate the MERT code (BLUE or PINK) in the hospital (see figure 1).
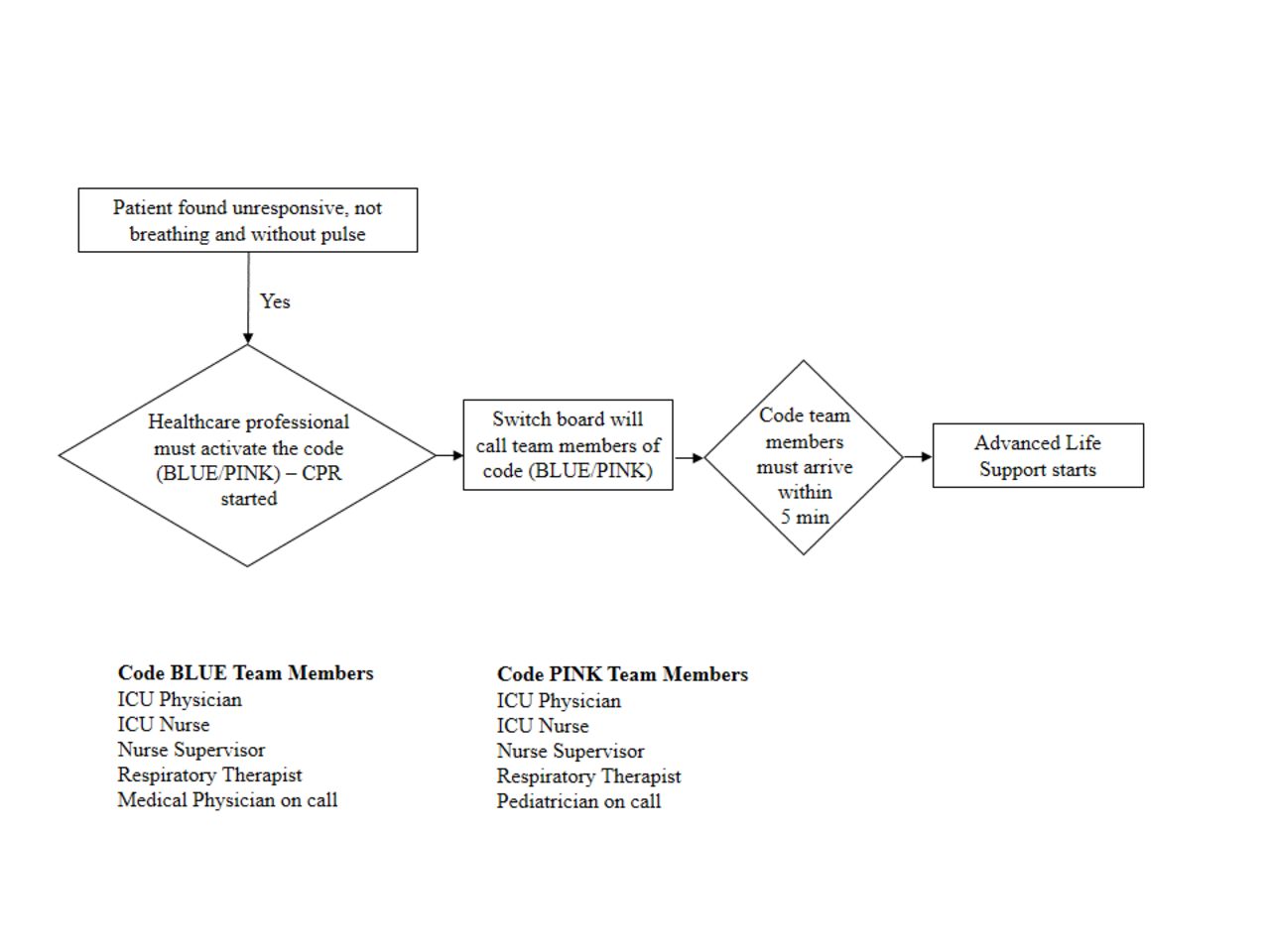
In hospital cardiac arrest and medical emergency response team flow diagram. CPR, cardiopulmonary resuscitation; ICU, intensive care unit.
Participants
All patients (regardless of age) who experienced an IHCA and underwent resuscitation between 1 January 2013 and 31 December 2015 were included in the analysis.
Study variables
Sociodemographic variables were age and gender of patients who experienced an IHCA. An IHCA was defined using the AHA 2013 Consensus Statement definition as a cardiac arrest that occurs in a hospital and for which resuscitation was attempted with chest compressions, defibrillation or both.8 Variables related to the IHCA event included time (day (07:00–18:59) vs night (19:00–06:59)), day (weekdays (Sunday to Thursday) vs weekends (Friday and Saturday)), the location of IHCA event, time of the MERT arrival at the scene, initial cardiac rhythm that caused the cardiac arrest and the total number of IHCA events. Outcome variables were the return of spontaneous circulation (ROSC) and survival to discharge (StD) from the hospital.
Data sources/measurement
At the time of an IHCA event, a member of the MERT recorded the data in the paper-based cardiopulmonary resuscitation (CPR) code form. Three copies of the code form were generated, one for the Life Support team, one for the nursing supervisor and one for the unit manager. The leader of the MERT (ICU physician) verified the data, approved the code form and then submitted it to the unit manager of where the IHCA event had occurred. The unit manager dispatched one code form to the Life Support Training Centre (LSTC). The original code form and one copy were kept in the patient file as a legal document. At the LSTC, two clinical research nurses entered the data into the database after examining the accuracy and completeness of the forms. To ensure that all cardiac arrest events were captured, the clinical research nurses periodically monitored the quality of the data and retrieved it for the analysis. In case of any missing data or discrepancy between the three sources of information, the clinical research nurses contacted the nurse supervisor to check the forms. There were no missing data (ie, 100% data capture) as it is mandatory for all citizens and residents in Abu Dhabi to have health insurance. The health insurance system and law in the emirate Abu Dhabi requires every patient encounter with a healthcare provider to be documented; therefore, no patient can be admitted to a hospital or receive treatment without documentation. In line with UAE law during the study period, the hospital policy did not allow the issuance of ‘Do Not Attempt Resuscitation’ orders for any patients (ie, all patients underwent CPR regardless of condition and/or prognosis).
Statistical methods
Data were extracted in a Microsoft Excel sheet and transferred to Stata V.14.2 for statistical analysis. Qualitative variables were tabulated as frequencies and percentages (%) and continuous variables as means±SD. In line with the AHA 2013 Consensus Statement, the incidence of IHCA per 1000 admissions was calculated by dividing the total number of patients who received chest compressions, defibrillation, or both by the number of patients admitted to the hospital during that period.8 Outcome variables were cross-tabulated with factors and characteristics. Chi-square and Fisher exact tests were performed to estimate differences in proportions of outcomes. The alpha value of p ≤0.05 was chosen to determine statistical significance.
Results
Participants
A total of 685 patients (66.3% men) experienced at least one IHCA event during the 3-year period under analysis (2013–2015) (table 1). The mean (±SD) age of patients was 57.3±23.3 years with 63.2% aged 40–79 years (table 1).
Characteristics and outcomes of patients who experienced an IHCA in a tertiary-care hospital, Abu Dhabi, United Arab Emirates, 2013–2015
Descriptive data
Non-shockable rhythm was more common (91.1%) than shockable rhythm (8.9%) and nearly half (46.1%) of the events occurred in the ICU. The majority (69.8%) of patients experienced only one IHCA event. The overall incidence of IHCA was 11.7 (95% CI 10.8 to 12.6) per 1000 hospital admissions (table 2). The incidence was the lowest in 2013 and highest in 2014 (table 2). Figure 2 shows the incidence of IHCA per 1000 admissions by months during the period of 2013 to 2015. No specific pattern was observed in the incidence of IHCA. The highest mean incidence was observed in January, February and April, while it was the lowest in March, September and October (figure 2).
Incidence of IHCA in a tertiary-care hospital, Abu Dhabi, United Arab Emirates, 2013–2015

{kind=link}
{kind=link}
Mean incidence of in-hospital cardiac arrests (IHCAs) per 1000 admissions by month in a tertiary-care hospital, Abu Dhabi, United Arab Emirates, 2013–2015.
Outcome data
Overall, 38.3% of patients who experienced an IHCA achieved ROSC and 7.7% survived to discharge from the hospital (table 1). The ROSC differed significantly with respect to age (p=0.047) and it was the highest in infants (46.1%). The StD was not significantly different among age groups (p=0.063). Patients presenting with shockable rhythm achieved the higher ROSC and StD compared with patients with non-shockable rhythms (table 1). Survival to discharge was significantly higher in non-ICU compared with ICU (table 1). Those patients experiencing two or more IHCA events had a significantly higher ROSC but a non-significant lower StD than patients experiencing only one IHCA (table 1).
Discussion
Summary of major findings
This is the first study reporting the epidemiology of IHCA and its outcomes in the UAE. In the present study, the overall incidence of IHCA between 2013 and 2015 was 11.7 per 1000 admissions, which ranged from 9.0 to 13.6. Non-shockable rhythm was more common than shockable cardiac rhythm at presentation. Most of the cases occurred in the ICU and on weekdays, while the proportion was equal during daytime versus night-time. In outcomes, 38.3% of patients who experienced IHCA achieved ROSC and 7.7% survived to discharge from the hospital. Both survival outcomes were significantly higher in younger age groups and patients with a shockable rhythm.
Comparison with previous studies
The incidence for the UAE (11.7) reported in our study between 2013 and 2015 was considerably higher than 0.7–1.7 in Israel from 1995 to 2015,9 1.5 reported in Italy in 2012–2014,10 1.6 in the UK in 2011–2013,11 1.7 in Sweden from 2006 to 2015,12 4.5 in the USA between 2000 and 2009,4 and 1.3–6.1 in population studies and 0.6–6.1 in cohort studies in Australia and New Zealand between 1987 and 2014.13 The comparison of incidence across studies is difficult due to marked differences in the characteristics and underlying conditions of patients, quality of care and data, and criteria for defining IHCA.4 10 14 Despite these differences, the high incidence of IHCA reported in our study is a concern and warrants the need for further longitudinal research and the development of a national UAE Register of Cardiopulmonary Resuscitation. Overall, 38.3% of patients with IHCA achieved ROSC in this study, which was higher than a single-site tertiary hospital in Uganda (7.4%5) and close to the value reported by Redeschi et al 10 (35.7%) in their cohort of patients in Italy. However, other studies conducted in Canada (46.9%15), Italy (52.8%10), Iran (42.9% in diabetic patients; 61.0% in non-diabetic patients16), Israel (12.8%–14.2%9), South Korea (54.1%–69.5%17), Thailand (58.9%18) and the UK (45.0%11) have reported better ROSC. A systematic review of 30 studies conducted in Australia and New Zealand representing more than 11.5 million hospital admissions between 1987 and 2014 reported that ROSC was achieved in 46.0% of patients with a trend for ROSC improving from 31.8%–43.8% between 1987 and 2007 to 54.1%–58.3% between 2009 and 2014.13 Survival to discharge was 7.7% in the present study. This is markedly lower than StD reported in Canada (13.1%15), Taiwan (14.1%19), Italy (14.8%10), the Get With The Guidelines–Resuscitation database in the USA (17.0%; 12.7% for recurrent IHCA and 22.1% for no recurrent IHCA20), the National Cardiac Arrest Audit in the UK (18.4%11) and in the Swedish Register of Cardiopulmonary Resuscitation (28.5%12). Overall, survival outcomes were lower in our study compared with other high-income/developed countries. However, it is difficult to explore the reasons for these marked differences without accurate and reliable data on pre-arrest, intra-arrest and post-arrest factors. The development and implementation of an integrated national UAE Register of Cardiopulmonary Resuscitation covering public and private hospitals across all seven emirates collecting detailed IHCA data would permit future studies to further explore the IHCA epidemiology within the UAE and make comparisons internationally.
Our study did not find any significant difference in survival outcomes with regard to gender, following the trend of similar studies in Canada,15 Italy,10 India,14 Israel,9 South Korea17 and Thailand18; however, female gender was associated with decreased 30-day survival in Sweden.12 Our study showed an increase in ROSC and a decrease in StD with age, excluding infants 0–12 months and from the age group <20 years old. There is a scarcity of studies documenting an association between age and survival after cardiac arrest,1 but there is emerging evidence that demonstrates an inverse association between age and survival rate in adult patients.1 9 10 12 A systematic review of 30 studies in Australia and New Zealand reported a positive association between age and mortality in three studies; specifically, ROSC was reduced by 35% (p=0.002) and StD by 36% (p=0.004) with each decade of life.13 In contrast, a recent study in three Canadian tertiary-care centres did not find an association between patient age and StD.15
More than 90% of patients who experienced an IHCA in our sample had a non-shockable initial cardiac rhythm, which is higher than other studies in Australia and New Zealand (68.6%13), Thailand (71.8%18) and the UK (72.3%10), but closer to the estimates reported for Canada (91.9%15), Israel (82.2% 2006–20159), and for recurrent IHCA (89.0%) and no recurrent IHCA (79.9%) in the USA.20 Interestingly, two recent studies have shown an increase in the prevalence of non-shockable initial arrest rhythms over the past two decades. Thompson et al 21 used data from United States Medicare beneficiaries (age ≥65 years; n=45 567) and reported that the prevalence of non-shockable initial arrest rhythms increased from 76.0% in 2000–2003 to 82.6% in 2008–2011. In Israel, the prevalence of non-shockable initial arrest rhythms has increased from 70.3% between 1995 and 2005 to 82.2% between 2005 and 2015.9 Based on the available patient data in our sample, it is unclear why there was a higher prevalence of non-shockable initial cardiac arrest rhythm in the UAE compared with other countries, but it may possibly be due to the high burden of diabetes and cardiovascular disease risk factors among the UAE national and expatriate population.22–25 In addition, the UAE has a high prevalence of trauma patients resulting from road traffic, occupational and childhood injuries,22 and this may account for the higher prevalence of non-shockable rhythms compared with other high-income/developed countries. As suggested by a reviewer, the observed higher incidence of non-shockable rhythms may also relate to delayed recognition of clinical deterioration. Previous research has shown that the outcome of IHCA is better when the first monitored rhythm is shockable rather than non-shockable.1 9 11–13 18 Consistent with earlier studies, the ROSC in our study was greater than 70% in patients with a shockable rhythm compared with 35% in non-shockable rhythm.11 The reason may be due to the fact that VF/VT can be assisted with defibrillation on time or deteriorates to asystole, which will lead to a worse outcome. In contradiction, a study reporting survival trends after IHCA in 374 hospitals in the USA found that survival outcomes increased regardless of whether the initial cardiac rhythm was treatable by defibrillation possibly due to improvements in both acute resuscitation survival and post-resuscitation survival.26
In our study, the most common location of occurrence of IHCA was the ICU. These results are expected as patients admitted to ICU are normally in a more serious condition compared with non-ICU.1 13 15 26–28 However, better survival outcomes were seen in patients in the coronary care unit (data not shown), which may be explained by the close monitoring of cardiac conditions in this unit and the immediate availability of staff who are specialised in providing advanced life support.1 28 A study conducted in a tertiary-care hospital in India reported that the most frequent location for IHCA was the general wards, but the best survival rate was in the cardiac catheterisation laboratory (60%).14 Moreover, a recent systematic review of 30 studies conducted in Australia and New Zealand reported that ROSC was higher in monitored arrests (64.3% vs 36.4%).13 The time response to an IHCA event can influence the outcome and the patient’s survival. Sandroni et al reported that no patient survived more than 6 min from the start of the IHCA to when the emergency team started advanced life support.28 In the present study, the ROSC and the StD were not significantly different between more and less than 3 min for the emergency team to arrive and initiate resuscitation.
The incidence of IHCA and survival outcomes were similar during the day versus the night shift in our study, which is in contradiction to some existing studies reporting that daytime cardiac arrests were associated with better ROSC and StD.11 13 27–29 The Get With the Guidelines–Resuscitation Registry is a prospective multisite registry of IHCA events in the USA and a recent study examined the temporal trends in survival differences between on-hours (ie, 07:00-22:59 Monday to Friday) and off-hours (23:00-06:59 Monday to Friday or anytime on weekends) IHCA using data from 151 071 adults at 470 US hospitals during 2000 to 2014.30 The study reported that survival was significantly lower in patients who arrested during off-hours (16.8%) compared with on-hours (20.6%; p<0.0001) and while survival increased in both groups between 2000 and 2014, the survival difference persisted (4.1% in 2000; 3.3% in 2014).30 The absence of a survival difference in our study might indicate similarity in the quality of care provided both during daytime and night-time. According to a systematic review of IHCA in Australia and New Zealand, daytime cardiac arrests were associated with greater ROSC (41.1% vs 17.0%, p=0.001) and survival (58.9% vs 41.0%, p=0.04).13 A small hospital-based study in the USA reported lower StD after midnight compared with day/evening time,31 and a prospective study showed a higher incidence of unwitnessed cardiac arrests during the night.32 The proportion of IHCA events during the weekend was 25.4%, and this was similar to a study in Italy that reported that 28.5% of the IHCA events occurred during the weekend.10 A study of 5 years of experience in South Korea showed that the likelihood of IHCA was not significantly different between the weekend and weekdays.17 Finally, recent studies have shown lower survival among patients who experienced an IHCA with type 2 diabetes mellitus compared with non-diabetes in both Iran (24-hour survival 19.0% vs 44.1%16) and the USA (StD 25.1% vs 27.0%33). In view that approximately ~9%–11% of expatriates23 25 and ~4%–19% of UAE citizens34 35 have type 2 diabetes mellitus, the documentation and reporting of comorbidities may be an important prognostic factor for IHCA survival in the UAE population.
Strengths and limitations
To our knowledge, this is the first study that has estimated the incidence and outcomes of IHCA and assessed its factors in the UAE. However, this study has several limitations: (1) data were recorded from a single hospital in the largest UAE emirate in terms of land mass and population, thus limiting the generalisability of the study findings to other hospitals in different UAE emirates; (2) the database did not collect information on factors such as ethnicity, nationality, education status, comorbidities or quality of care; and (3) neurological deficits are common in patients who experienced an IHCA; however, this study could not assess the rate of neurological deficits due to unavailability of data.
Implications for clinicians and policy makers
There are a number of clinical and strategic implications from the current study findings. Although the study was limited by the lack of data on the reason for admission, the incidence of IHCA was relatively high and StD was low compared with other high-income/developed countries, and this may indicate the need for improvements in patient care and monitoring during admission to prevent IHCA. Similarly, the higher incidence of IHCA may be related to other factors such as low health literacy among the UAE population leading to late presentation and admission of patients with underlying acute or chronic health conditions that may lead to IHCA; however, we have no data to support this proposition. Notably, more than 90% of patients who experienced an IHCA had a non-shockable rhythm, and this highlights the need to focus on the early identification of IHCA and immediate intervention with non-shockable protocols including intravenous administration of epinephrine. It is unclear why survival outcomes were lower than other high-income/developed countries, but this information could be used by clinicians to better inform family members about prognosis and end-of-life decisions, which are important in any country, especially the UAE where the laws and customs are rooted in Islamic principles. Finally, policy-makers need to implement an inter-emirate UAE Register of Cardiopulmonary Resuscitation that collects detailed information on all IHCA that could be used to develop prognostic models for the UAE.
Areas for future research
Our study was limited by the lack of detailed information required to further our understanding of the factors associated with an IHCA event and survival. In view of this limitation, future studies may want to consider collecting and reporting data on pre-arrest factors (eg, age, sex, nationality, reason of admission, aetiology of cardiac arrest, underlying disease, blood chemistry), intra-arrest factors (eg, witnessed IHCA, duration of CPR, dose of epinephrine, deviations from protocol) and post-arrest factors (eg, post-arrest care and monitoring, post-arrest events such as coma, seizures and infections). Currently, there is a lack of data on post-discharge survival and longitudinal studies and nationwide registries should endeavour to collect longer-term follow-up survival statistics at 7 and 30 days after discharge, in addition to 6, 12 and 24 months postdischarge. A recent study in Thailand reported poor postdischarge survival in patients who experienced an IHCA with a decline in survival from 23.8% StD to 17.8% at 7 days, 14.4% at 30 days, 9.4% at 6 months and 7.9% at 12 months.18 A retrospective register study based on the Swedish Register of Cardiopulmonary Resuscitation analysed data (n=18 069) from 66 out of 73 hospitals (2006–2015) and reported survival rates of 28.5%, 28.3% and 25.0% for patients who experienced an IHCA at discharge, 30 days and 12 months, respectively.12 Moreover, the study found that a delay of >1 min from cardiac arrest to call, to start of CPR, a delay of >2 min from call until the arrival of the rescue team, a delay of >3 min from cardiac arrest to defibrillation, and treatment with hypothermia, intubation and treatment with adrenalin and other vasopressors during resuscitation were associated with decreased 30-day survival.12 The following factors were associated with increased 30-day survival: arrests occurring between 08:00 and 20:00 on working days, primary arrhythmia as the precipitating sign, monitored and witnessed arrests, and VT/VF as the presenting rhythm.12 A study in the USA used data on Medicare beneficiaries (age ≥65 years; n=45 567) with an IHCA occurring between 2000 and 2011 at Get With The Guidelines–Resuscitation Registry participating hospitals and reported that 1-year survival nearly doubled from 8.9% in 2000–2001 to 15.2% in 2011.21 Clearly, postdischarge factors are important for long-term morbidity and mortality, and future studies could incorporate telephone, web-based or app-enabled data collection tools during the postdischarge follow-up period. As suggested by a reviewer, future studies may want to consider close tracking of vital signs preceding an IHCA as abnormal vital signs are related to clinical deterioration that occurs minutes to hours before a serious adverse event.36–38 Thus, breaches of accepted thresholds for normal vital signs may act as an early warning sign that a patient is experiencing clinical deterioration that could lead to an IHCA.
Generalisability
This paper contains the first data on the epidemiology of IHCA in the UAE. However, as mentioned in the limitations, the IHCA estimates are from a single hospital in the emirate of Abu Dhabi over a 3-year period from 2013 to 2015. While this study provides novel and original data on the epidemiology of IHCA in the UAE, the results are not generalisable to all tertiary-care hospitals in the UAE or Gulf region. This study highlights the need for a national UAE Register of Cardiopulmonary Resuscitation that requires all government and private hospitals across the seven UAE emirates to report detailed information on the incidence of IHCA and accompanying pre-arrest, intra-arrest and post-arrest factors. A coordinated and harmonised registry across all UAE hospitals and different health systems would also facilitate postdischarge data collection on morbidity and mortality.
Conclusion
This study, the first in the UAE, showed a higher incidence of IHCA and lower rates of survival outcomes in a large tertiary-care hospital compared with other high-income/developed countries. This study also found that survival outcomes of IHCA were similar with respect to time of day and week, but were different with regard to location, initial cardiac rhythm and age. These findings may help to inform health managers and stakeholders about the magnitude and quality of IHCA care in the UAE.
References
Footnotes
Contributors All authors have made substantial contributions to all of the following: EHD and TL conceived the study and provided the data; FA wrote the first draft, analysed and interpreted the data; MSP contributed to the writing of the manuscript; TL revised the article and provided critical and important intellectual content. All the authors read and accepted the final version of the manuscript for publication.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval This study was approved by the Al Ain Hospital Research and Ethics Governance Committee (#AAHEC-02-18-082).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All relevant data are within the paper. Access to the raw data is legally governed by the Institute of Public Health, United Arab Emirates University (United Arab Emirates) and the Ambulatory Healthcare Services, Abu Dhabi (United Arab Emirates). Data are available after application and agreement with the Institute of Public Health (United Arab Emirates University) and the Ambulatory Healthcare Services. In addition to this application, an existing or new approval from the Hospital Research and Ethics Governance Committee may be required. Details on this procedure are available from the corresponding author, TL, who may be contacted through email (tom.loney@mbru.ac.ae).