Article Text

Statistics from Altmetric.com
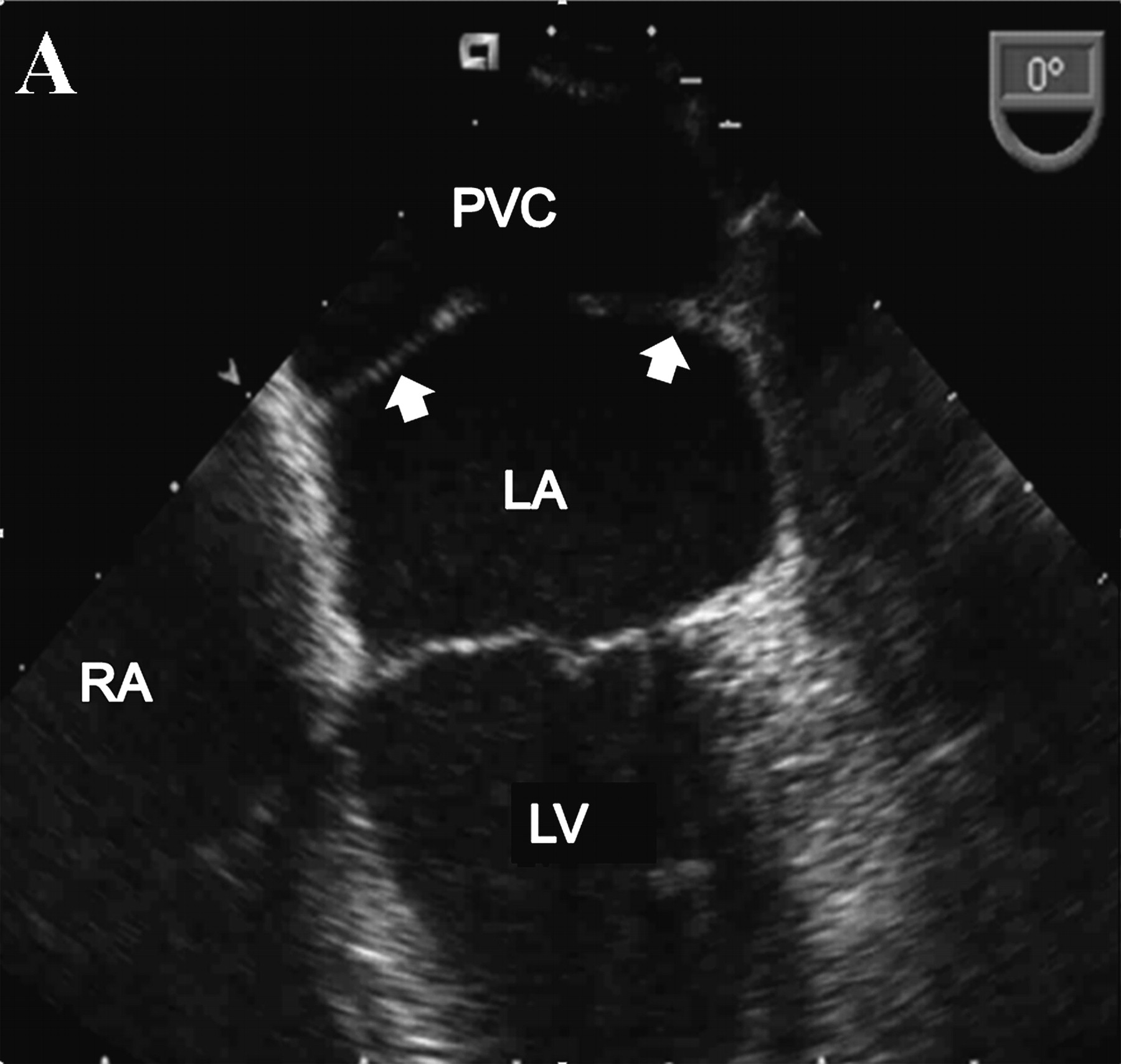
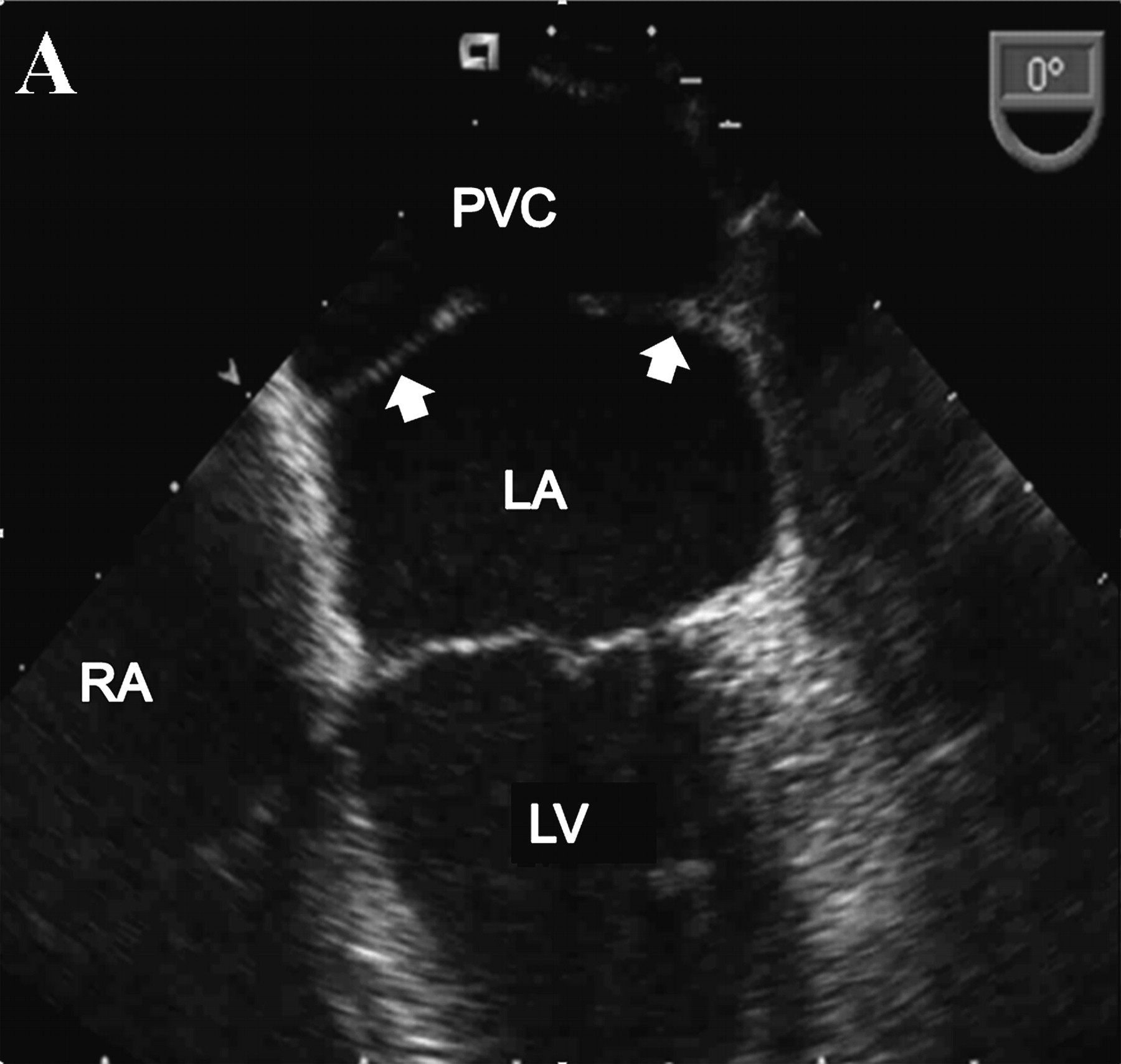
A 67-year-old lady was referred to our institution 3 years ago with a heart murmur, having had an atrial septal defect (ASD) repair with a Dacron patch 20 previously. Transthoracic echocardiography demonstrated a linear echo-density in the left atrium. On transesophageal echocardiogram (TOE; panel A), a septum (white arrows) divided the left atrium into two chambers connected by a visible channel (LA, left atrium; LV, left ventricle; PVC, pulmonary venous chamber; RV, right ventricle). Doppler echocardiography revealed minimal trans-membrane gradient suggesting a non-obstructive form of cor triatriatum sinistrum.
During follow-up, she developed exertional dyspnoea and peripheral oedema, associated with elevated right heart pressures. Cine MR images (panel B) demonstrated a sizeable transverse septum dividing the left atrium (black arrowheads) with turbulent flow on the pulmonary venous side.

{kind=link}
{kind=link}
Although she had haemodynamically significant obstruction, she declined referral for corrective surgery.
Discussion
In classical Cor triatriatum sinistrum, a fibromuscular membrane separates the left atrium into a common pulmonary venous chamber (receiving blood from the pulmonary veins) and the true left atrium (communicating with the mitral valve and left atrial appendage). The membrane may contain one or more restrictive orifices. Most cases present in the neonatal period or infancy, and 70–80% of cases are associated with an ASD.
When there is a large communication between the chambers, presentation can occur in adulthood and may be found incidentally on cardiac imaging. Late conversion to a symptomatic state may be caused by fibrosis and calcification in the orifice of the separating diaphragm.1
Cor triatriatum sinistrum may be missed on TOE due to poor spatial resolution in the posterior left atrium, close to the transducer. Cardiovascular magnetic resonance (CMR) imaging is useful for imaging cor triatriatum. In general, it provides better spatial resolution and superior tissue contrast compared with echocardiography and imaging is easily performed in multiple planes.2
Preoperatively, CMR provides excellent delineation of the dividing membrane and guides the surgical approach.3 Cine imaging clearly depicts fenestrations in the membrane and is useful for demonstrating any turbulent flow across it.
Footnotes
Competing interests None.
Patient consent Obtained.