Article Text

Statistics from Altmetric.com
Despite declining prevalence of Eisenmenger Syndrome (ES) in the West, such patients are not uncommon in the developing world. Important clues to the level of shunt are provided by differential cyanosis and clubbing indicating a patent ductus arteriosus (PDA) or the degree of splitting of second heart sound.1 The reason for the differential cyanosis and clubbing is that due to the right-to-left shunt across the PDA, deoxygenated blood from the right ventricle is preferentially directed into the aorta distal to the left subclavian artery and into the lower extremities.
With PDA, ES and right-to-left shunt, an erroneous diagnosis of primary pulmonary hypertension may be made on echocardiography since no obvious septal defect is visualised. Contrast echocardiography using agitated saline, with opacification of abdominal aorta without opacification of left-sided chambers is helpful in such cases.
We describe a 38-year-old male with no known previous congenital heart disease who presented with exertional dyspnoea and haemoptysis since the last 5 years. Examination revealed obvious differential cyanosis and clubbing (figure 1), closely split second heart sound with right atrial and right ventricular dilatation, elevated right ventricular systolic pressure and severe pulmonary artery hypertension on echocardiography (figure 2). Contrast echocardiography findings (figure 3, supplementary video 1) revealed rapid opacification of descending aorta, clearly visualised in the subcostal view, establishing the diagnosis of PDA with ES.

Differential cyanosis and clubbing.
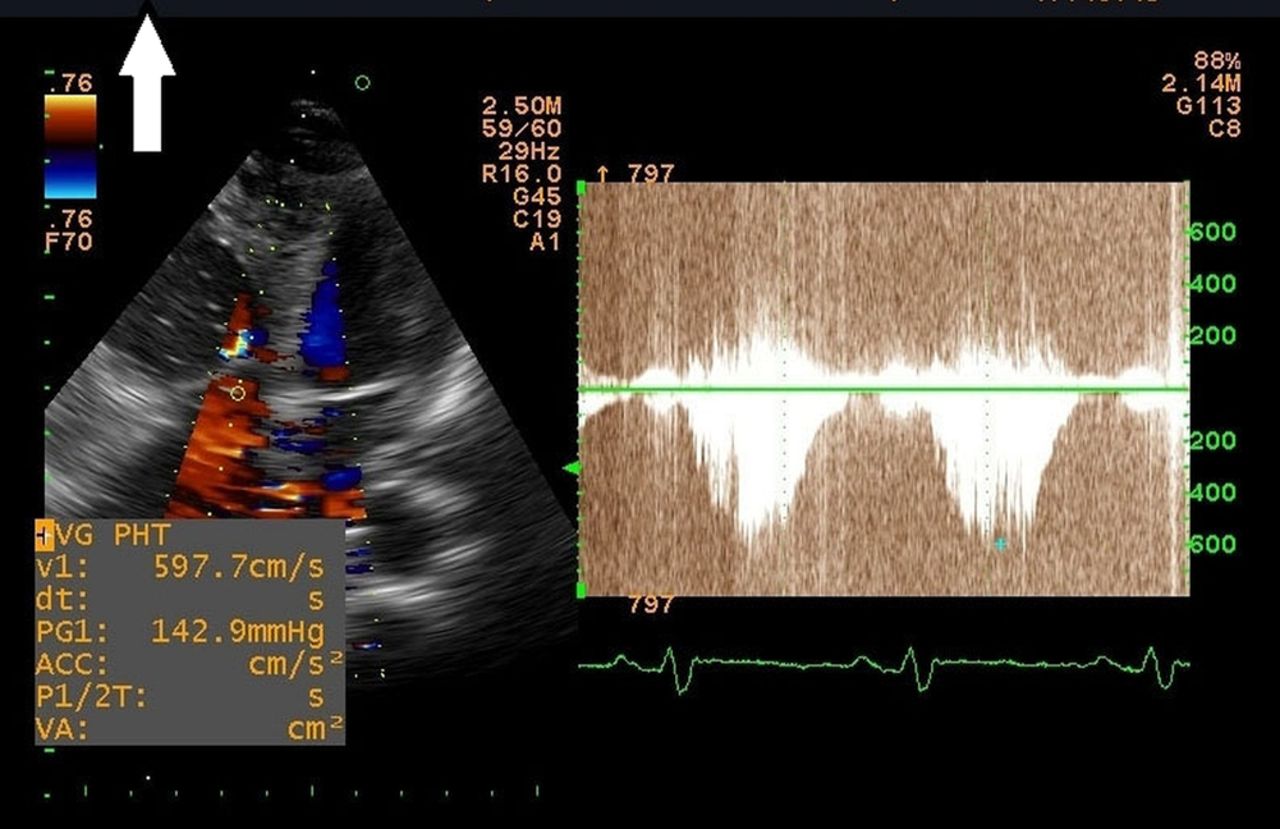
2D echocardiography showing dilated right atrium and right ventricular (RV) tricuspid regurgitation and severely elevated RV systolic pressure.
{kind=link}
{kind=link}
{kind=link}
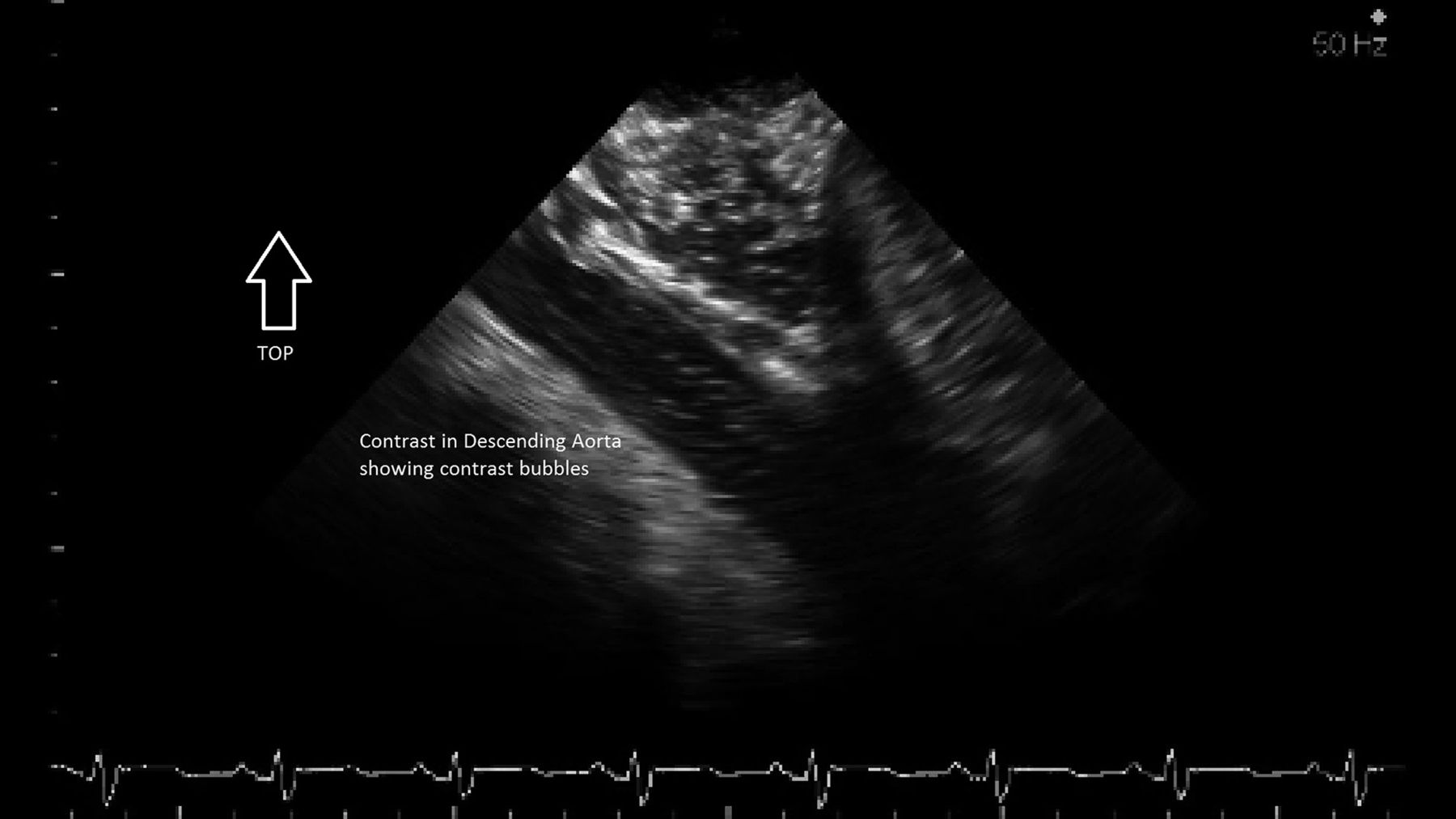
Contrast echocardiography revealed rapid opacification of descending aorta, clearly visualised in the subcostal view.
Reference
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online video
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; internally peer reviewed.