Article Text

Abstract
Objective Women have been under-represented in randomised clinical trials for primary prevention implantable cardioverter defibrillators (ICDs), and there are concerns about the efficacy of devices between genders. Our study aimed to investigate gender differences in the use of primary prevention ICD in patients with heart failure from the northern region of New Zealand.
Methods Patients with heart failure with systolic dysfunction who received primary prevention ICD/cardiac resynchronisation therapy-defibrillator (CRT-D) in the northern region of New Zealand from 1 January 2007 to 1 June 2015 were included. Complications, mortality and hospitalisation events were reviewed.
Results Of the 385 patients with heart failure implanted with ICD/CRT-D, women comprised 15.1% (n=58), and no change in utilisation of these devices was observed over the study period among women. Women were more likely to have non-ischaemic cardiomyopathy and have higher perioperative complications (8.6% vs 2.5%, P=0.02), with non-significant higher trend towards increased lead displacement (5.2% vs 1.8%, P=0.12). Women appeared to have lower all-cause (10.3% vs 18.7%, P=0.12), cardiovascular (5.2% vs 11.9%, P=0.13) and heart failure (3.5% vs 7.9%, P=0.22) mortalities but was not statistically significant. There were no gender differences in all-cause (70.7% vs 67%, P=0.58) or heart failure (19% vs 25%, P=0.32) readmissions.
Conclusion Perioperative complications were significantly more common in women referred for ICD/CRT-D. Although there has been a significant increase in ICD implantation rates, gender differences in the use of these devices still exist in New Zealand, in keeping with the demographics of ischaemic heart disease and systolic dysfunction between genders.
- implantable cardioverter defibrillator (icd)
- heart failure
- sudden cardiac death
Statistics from Altmetric.com
Introduction
Clinical trials on the use of implantable cardioverter defibrillators (ICDs) and cardiac resynchronisation therapy (CRT) have demonstrated overall survival benefits in selected patients with heart failure (HF).1–5 ICDs reduce the risk of sudden cardiac death (SCD), whereas the mortality benefit of CRT is related, in part, to favourable left ventricular reverse remodelling with attenuation of both HF death as well as SCD.
The role of primary prevention ICD in women with HF has not been well established. Many of the clinical trials of ICDs were underpowered to assess risks and benefits of ICDs in women. Traditionally women have been under-represented in trials of HF and ICD therapy, with only small numbers of women being enrolled.1 6 7 According to current international guidelines, recommendations for primary prevention ICD/CRT-D are not different for men and women with HF and impaired left ventricular function. A meta-analysis of the five primary prevention trials (Multicenter Unsustained Tachycardia Trial [MUSTT], Multicenter Automatic Defibrillator Implantation Trial II [MADIT II], Defibrillator in Acute Myocardial Infarction Trial [DINAMIT], Defibrillators in Non-Ischemic Cardiomyopathy Treatment Evaluation [DEFINITE], and Sudden Death in Heart Failure Trial [SCD-HeFT]) showed that men, but not women, derived a survival benefit from ICD as compared with antiarrhythmic drugs.8 However, a recent primary prevention trial in patients with HF confirmed equal survival advantage in both men (HR 0.76, 95% CI 0.67 to 0.87, P<0.001) and women (HR 0.78, 95% CI 0.66 to 0.92, P=0.003).9 These findings support the use of primary prevention ICD in eligible patients regardless of gender.
Despite women accounting for 50% of HF admissions, eligible women were less likely to receive an ICD compared with men (40% lower odds).10 In New Zealand, a gender difference in ICD implantation was documented by Larsen et al 11 during the period of 2000–2007. The study showed the majority (71%) of the primary prevention ICDs being implanted were in men.11 Currently there are no data on the use of primary prevention ICD for women with HF in New Zealand. Our study aimed to examine the gender differences in the use of primary prevention ICDs in patients with HF in the northern region of New Zealand.
Methods
This was an observational study that included patients with HF who received primary prevention ICD/CRT-D in the northern region of New Zealand. The northern region of New Zealand is defined as the four northernmost district health boards (DHBs) areas and consists of Auckland DHB, counties Manukau DHB, Northland DHB and Waitemata DHB. The four DHBs in the northern region serve 38% of the total New Zealand population, with an estimated 1.76 million people in this region.12 The study period was from January 2007 to 1 June 2015. We included patients undergoing all de novo ICD and CRT-D implants, all pacemaker upgrades to ICD and CRT-D, and epicardial lead placement with CRT-D. Procedures involving solely ICD and CRT-D pulse generator replacement were excluded.
Patient demographic data, procedure-related data, acute (within 24 hours of implant), early (>24 hours to 2 weeks from implant) and late (≥2 weeks after device implantation) complications were obtained via review of pacing database and clinical records held on electronic clinical record information system.
Mortality data were collected using New Zealand mortality collection and National Minimum Datasets (NMDS) inpatient hospitalisation data. These include all registered deaths rather than just deaths in the hospital. The cause of death data were available up until the end of 2013. For those with no cause of death data from NMDS, review of clinical records was performed to further determine the cause of death.
Hospitalisation events were identified using the administrative data of the Ministry of Health and NMDS inpatient hospitalisation data via National Health Index (NHI) linkage up to December 2015. The NHI number is a unique identifier that is assigned to every person who uses health and disability support services in New Zealand. HF hospitalisation was defined using the International Classification of Diseases-10 diagnosis codes (I110, I130, I132, I500, I501 and I509).
Statistical analysis
Baseline demographics were summarised as means with 1 SD or frequencies with percentage (%). Comparisons of baseline characteristics between genders were conducted with either the Wilcoxon rank-sum test, the χ2 test or the two-sample Z test. Plots to depict the implantation frequency of ICD and CRTD among men and women over the course of the study were constructed. Kaplan-Meier survival curves were generated to depict the distribution of cardiovascular and HF mortalities over time. The difference of the survival distributions between men and women was evaluated with the log-rank test.
The difference in complication rates, device therapy treatment rates and mortality rates between genders was assessed with the χ2 test or the two-sample Z test. Readmission rates between genders were compared with the two-sample Z test. Logistic regression was used to determine predictors of all-cause mortality and HF mortality after adjusting for baseline characteristics.
Statistical analyses were performed using the statistical package SAS V.9.3. All P values resulted from two-sided tests and a P value of <0.05 was considered statistically significant.
Results
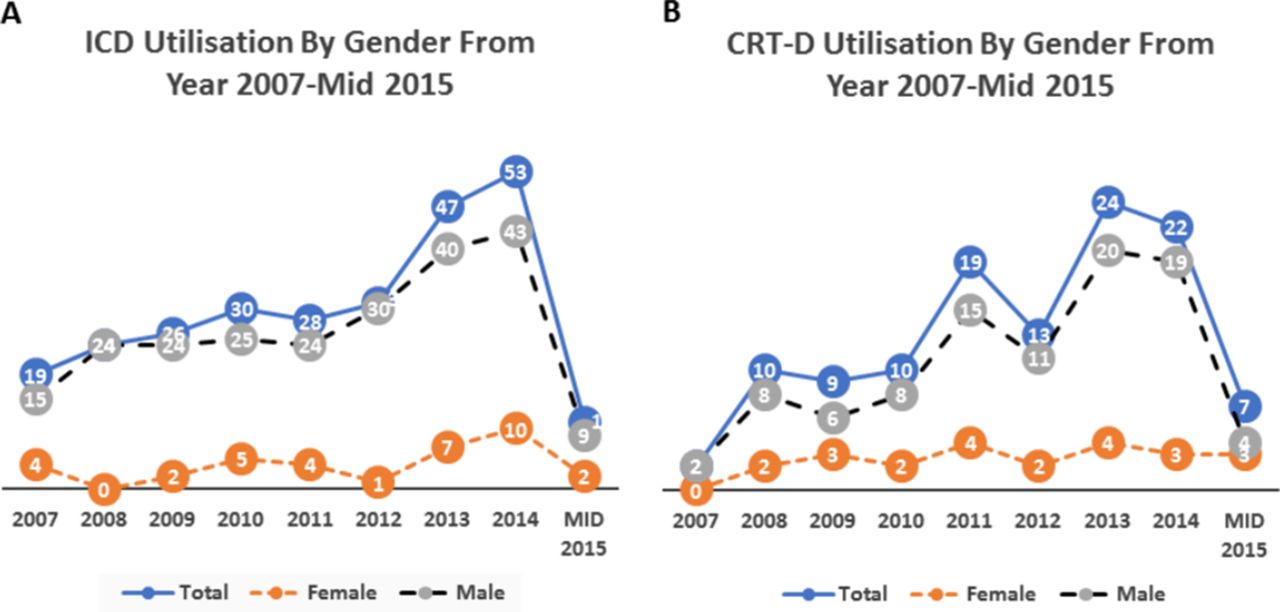
From January 2007 to June 2015, a total of 385 patients with HF underwent 404 procedures. Women comprised 15.1% (n=58) of the study cohort. Throughout the study period, there were differences in ICD/CRT-D utilisation in men and women. In men, there was a steady increase in ICD/CRT-D utilisation, but this trend of increase was not seen in women (figure 1A,B).

(A) Overall implantable cardioverter defibrillator (ICD) utilisation in men and women over the study period. (B) Overall cardiac resynchronisation therapy-defibrillator (CRT-D) utilisation in men and women over the study period.
Differences in baseline characteristics were summarised in table 1. Women were more likely to have non-ischaemic cardiomyopathy (NICM) and cardiac sarcoidosis than men. In addition, women had a higher prevalence of left bundle branch block (LBBB) (43.1% vs 32.4%) but were less likely to have chronic atrial fibrillation (AF). No significant differences were found in age, mean left ventricular ejection fraction (LVEF), New York Heart Association functional classes or other comorbidities.
Baseline characteristics of women and men with primary prevention ICD
Complications
During the 24 hours immediately after device implantation, acute perioperative complications were more common in women compared with men (8.6% vs 2.1%, P=0.008) (figure 2). In particular, women had a non-significant higher trend of lead displacement (5.2% vs 1.8%, P=0.12) and cardiac tamponade requiring interventions (0.18% vs 0) when compared with men.

Acute, early and late complications by gender.
No significant differences were observed in early and late complications between men and women (figure 2).
Device therapy
Overall 19.7% of patients received antitachycardia pacing (ATP) and 17.1% had appropriate ICD shocks for ventricular tachyarrhythmias. There was no gender difference in the need for appropriate ATP (13.8% in women vs 20.8%, P=0.22) or shocks (12.1% in women vs 18%, P=0.27). There was no gender difference in the time to first ATP (3.6±2.6 years vs 3.61±2.3 years, P=0.89) or time to first appropriate ICD shocks (3.7±2.6 years vs 3.6±2.2 years, P=0.77).
At the end of the follow-up, 9.1% of patients had received inappropriate shocks, but no gender difference was noted (8.6% vs 9.2%, P=0.89).
Mortality
The total duration of follow-up was 10.2 years with a mean duration of 3.64±2.17 years. At the end of the follow-up, a total of 67 (17.4%) patients had died: 61 (18.7%) men and 6 (10.3%) women (P=0.12). Women appeared to have lower cardiovascular mortality (5.2% vs 11.9%, P=0.13) and HF mortality (3.5% vs 7.9%, P=0.22) compared with men but was not statistically significant. There were only two sudden arrhythmic deaths and both were men. Figure 3A,B showed the Kaplan-Meier survival curve for cardiovascular and HF mortalities in women and men.

{kind=link}
{kind=link}
{kind=link}
(A) Kaplan-Meier survival curve for cardiovascular mortality. (B) Kaplan-Meier survival curve for heart failure mortalities.
After adjusting for baseline differences including gender, low LVEF (OR 0.94, 95% CI 0.892 to 0.99, P=0.02) was the only predictor of all-cause mortality, whereas CRT-D use was associated with improved all-cause survival (OR 0.419, 95% CI 0.183 to 0.962, P=0.04). No predictors were of statistical significance in HF mortality.
All-cause and HF readmissions
During follow-up, there were 1194 all-cause hospital readmissions in 260 patients, which include 275 (23%) HF admissions. All-cause readmissions occurred in 70.7% of women compared with 67% of men (P=0.58). HF admissions occurred in 19% of women compared with 25% of men (P=0.32).
Discussion
We examined the gender differences in the use of primary prevention ICD/CRT-D in real-world HF population in the northern region of New Zealand. The following are the main findings: (1) Women comprised only 15.1% of those who received primary prevention ICD/CRT-D. (2) In women undergoing implantation, there was a higher prevalence of NICM, LBBB with broader complex width and a lower prevalence of AF. (3) Women have overall higher periprocedural complication rates but similar early and late complication rates. (4) No gender differences were noted in rates of appropriate and inappropriate ICD shocks. (5) No gender differences were noted in all-cause and HF rehospitalisation rates and mortality.
Epidemiological and clinical studies have suggested gender-related differences in the delivery of guideline-recommended HF treatments.13 14 In the Get With the Guidelines-Heart Failure programme, a significant increase in ICD use was observed over time in patients with history of HF and LVEF (≤35%), but gender differences persisted.15 A study by Hernandez et al 16 showed that while 44% of eligible men with HF and LVEF ≤30% received ICD, only 28% of eligible women received ICD therapy. New Zealand traditionally has had lower implant rates/million population for ICD.11 Taking into account affordability and capacity constraints, the published 2010 New Zealand guidelines are relatively conservative (box 1) and this may result in low referral rates.17 In our study, the percentage of ICD/CRT-D utilisation in men gradually increased from year 2007 to mid-2015, but this is not seen in women and a gender discrepancy remained in the use of these complex devices (figure 1A ,B). The original trials of ICD/CRT-D showed the benefit derived from ICD is greater in patients with ischaemic cardiomyopathy, which is more common in men and occurs at a younger age.1 3 7 Women are more likely to have HF with preserved systolic function and present at a later age.18 Similarly, we have observed women with different clinical profiles compared with men (table 1), which may account for the lower ICD/CRT-D implant rates in women. The mean age of women who received these devices was younger because of our more restrictive recommendations, otherwise they shared similar baseline characteristics to other published data.17 19 20
New Zealand primary implantable cardioverter defibrillator implantation and cardiac resynchronisation therapy guidelines17
Recommendations for primary ICD implantation in New Zealand
Patients with ICM at least 1 month after acute MI or an NICM present for at least 3 months.
EF ≤30% measured ≥3 months after optimal heart failure treatment.
NYHA class II or III.
On maximal heart failure medications, including ACE inhibitors or angiotensin receptor blockers, beta-blockers and spironolactone as tolerated for at least 3 and preferably 6 months.
No clinical symptoms or findings that would make them a candidate for a revascularisation procedure.
At least 3 months remote from any revascularisation procedure.
No associated disease with a likelihood of survival <18 months.
Age ≤75 years.
Recommendations for cardiac resynchronisation therapy in New Zealand
EF ≤35% after ≥6 weeks of optimal heart failure treatment, with QRS duration >149 ms or 120–149 ms with two additional criteria for dyssynchrony (aortic pre-ejection delay >140 ms, interventricular mechanical delay >40 ms or delayed activation of the posterolateral left ventricular wall).
NYHA class III.
No major cardiovascular event in the prior 6 weeks and be in sinus rhythm.
No major comorbidity reducing survival <18 months or seriously impairing quality of life.
EF, ejection fraction; ICD, implantable cardioverter defibrillator; ICM, ischaemic cardiomyopathy; MI, myocardial infarction; NICM, non-ischaemic cardiomyopathy; NYHA, New York Heart Association.
MacFadden et al 20 reported a 50% higher occurrence of any major or minor complications in women at 45-day follow-up. Similarly, recent findings from the National Cardiovascular Data Registry (NCDR) demonstrated a higher risk of cardiac perforation and pneumothorax in women.19 In our current study, women had higher perioperative complication rates than men, but there were no gender differences in the longer term device-related complications. This differs from the previously described increased risk of complications in women in general. This may be explained by the small number of women included in the study, and therefore no conclusive evidence of gender differences in late complications could be drawn.
Some studies have shown that women receiving primary prevention ICDs have a lower risk of death and appropriate ICD shocks than men. In a large multicentre French registry, women who had ICD implantation for primary prevention had a significantly lower likelihood of receiving appropriate ICD therapies (17.4% vs 23%, P<0.001) but had similar mortality compared with men (HR=0.87, 95% CI 0.66 to 1.15, P=0.324).21 There was no gender difference observed with inappropriate shocks (6.7% vs 6.7%, OR 1.0, 95% CI 0.74 to 1.35, P=0.997).21 Similarly, Seegers et al 22 showed that women received 50% less appropriate ICD shocks than men (3.6% vs 6.3% per year, P=0.002), although both groups have similar mortality (P=0.08). In a recent systematic review and meta-analysis, women were found to have a lower incidence of first appropriate ICD shocks and death than men but a similar risk of receiving inappropriate ICD shocks.23 Contrary to the published studies, our study showed that there was no gender difference in the appropriate and inappropriate ICD shocks. There appeared to be a trend towards lower all-cause, cardiovascular and HF mortalities in women, but it was not statistically significant. This may be explained by the small number of women, and our results would be consistent with the literature with lower mortalities observed in women.
There has been increasing interest in the optimisation of ICD programming to prevent inappropriate and appropriate but unnecessary device therapy. Prior to 2013, our ICD programming was not standardised and often comprised manufacturer defaults, which were tailored to each patient by depending on history, results of defibrillation threshold testing and the electrophysiologists’ preferences. Three different trials demonstrated recently that a longer number of intervals to detect ventricular fibrillation (NID) and a high rate cut-off reduce ICD therapies in primary prevention patients.24–26 Subsequent to these publications, we have moved to a programming strategy of longer NID in line with the published expert consensus statement on optimal ICD programming and testing.27
HF is a chronic, long-term health condition, but improved survival has brought with it significant financial burdens on our healthcare system. In New Zealand, approximately 5500 patients are hospitalised with decompensated HF each year.28 Poor outcomes are common after hospitalisation for HF, with 1-year readmission rates >50% and 1-year mortality >30%.29 Findings from the NCDR showed that women had higher HF readmission rates than did men (14% vs 10%, P<0.001).19 Even all-cause readmissions within 6 months were higher in women than in men, and these differences persisted after adjusting for baseline differences (OR 1.22, 95% CI 1.16 to 1.28, P<0.001).19 However, in our study there were no gender differences in all-cause hospitalisation rates including HF hospitalisation rates. It is possible that the small number of women included in our study could not account for differences. It is also possible that higher CRT use in women in our population (39.7%) potentially contributed to the comparable HF hospitalisation rates. A recent meta-analysis revealed that women derived greater benefit from CRT than men.30 However, additional studies with a larger number of women are needed to determine if there are other unmeasured confounders that might contribute to gender differences and outcomes in our population.
Limitations
First, our study lacks the denominator describing women with HF who were eligible but not implanted to demonstrate a real disparity in the use of these complex devices. Second, our study is limited by the small number and sample size of women included, which in itself may not be powered enough to detect differences in the outcome. Third, our study was a non-randomised observational study from four DHBs; therefore, our results may not apply to other centres in New Zealand. However, given the paucity of data of these devices in New Zealand, our study represents the real-world data on the use of these devices in HF women and their outcomes.
Conclusion
In our study, the incidence of early complications was higher in women referred for primary prevention ICD/CRT-D. Women also presented with a different clinical profile from men and account for a minority of ICD/CRT-D recipients. The differences in disease pattern and left ventricular impairment between genders may have contributed to our results. Although these results should not preclude eligible women from receiving these devices, a broader perspective on outcomes such as cost and quality of life is needed to inform decisions around primary ICD implantation in women with HF.
Key messages
What is already known about this subject?
Many of the clinical trials of implantable cardioverter defibrillators (ICDs) were underpowered to assess the impact of primary prevention ICDs for women.
What does this study add?
ICD implantation was less common in women in New Zealand, likely in keeping with the demographics of ischaemic heart disease and heart failure with preserved systolic function.
Perioperative complications were more common in women referred for primary prevention ICDs.
Women appeared to have lower long-term all-cause, cardiovascular and heart failure mortalities, although not statistically significant.
How might this impact on clinical practice?
This study shows that despite the higher perioperative complications in women who received primary prevention ICDs, they appeared to have lower long-term mortality compared with men.
This study highlights the importance of ongoing gender-specific analysis in medical device clinical studies to further improve the application of available evidence on ICDs in appropriate eligible women with heart failure.
Acknowledgments
The authors thank Charlene Nell, Desktop Support Team Administrator at Green Lane Cardiovascular Services/Cardiology Department, for her secretarial support.
References
Footnotes
Contributors KLL was involved in conception and design of the study. KLL, LC, LD and DS were involved in data collection. KLL and KS were involved in analysis and interpretation of data. KLL, KS, LC, AG and NL contributed to the writing of the manuscript as well as jointly developing the structure and arguments for the paper. All authors reviewed and approved the final manuscript.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethics approval for the study was obtained from the Central Health and Disability Ethics Committee (ethics ref: 15/CEN/58/AM02).
Provenance and peer review Not commissioned; externally peer reviewed.