Article Text

Statistics from Altmetric.com
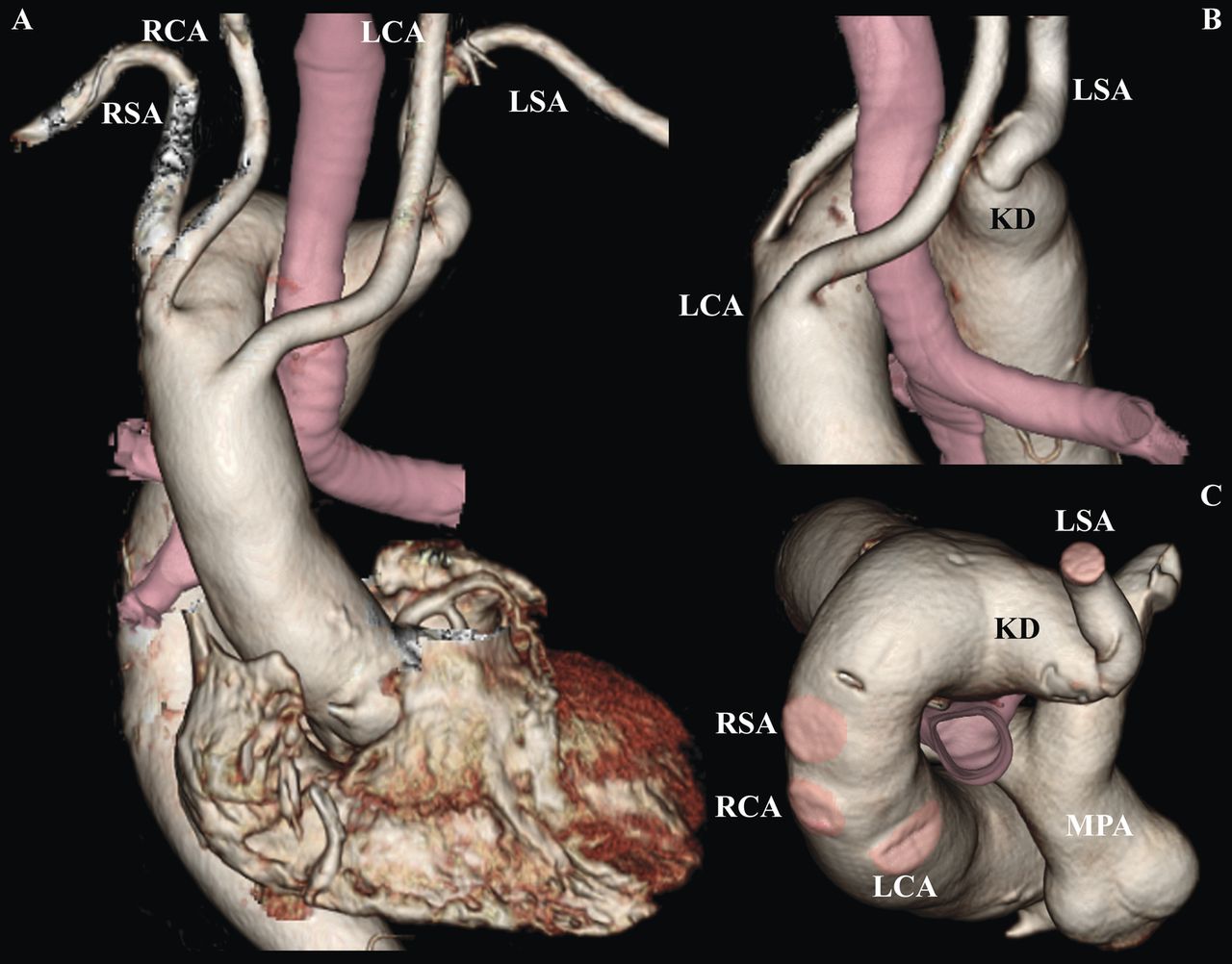
A 73-year-old man was referred for evaluation of ischaemic heart disease. During the evaluation a chest x-ray examination showed a right aortic arch (RAA) (figure 1). Three-dimensional CT showed a RAA with the Kommerell diverticulum (KD), from which arose an aberrant left subclavian artery (LSA) (figure 2A). The RAA separated branches arising in the following order: left common carotid artery, right common carotid artery, right subclavian artery (RSA) and aberrant LSA. Three-dimensional CT from the left posterior (figure 2B) and cephalic (figure 2C) view with resected branches clearly illustrated that the trachea was caught by the encircled space called the vascular ring, which comprised the KD and the RAA with residual ligamentum arteriosum to the descending aorta.

Chest radiograph from a posteroanterior view showing the abnormal shape of the aorta.

{kind=link}
{kind=link}
Three-dimensional reconstruction of CT image showing the right-sided aortic arch with aberrant left subclavian artery originating from a Kommerell diverticulum from (A) a front view; (B) a left posterior view. (C) Cephalic view with retro-oesophageal LSA. LCA, RCA, left, right carotid artery; LSA, RSA, left, right subclavian artery; MPA, main pulmonary artery.
A KD was first described by Kommerell1 in 1936 as a rare congenital aneurysm of the origin of the aberrant subclavian artery. Development of KD with RSA occurs in 0.5–1.0% of the population, whereas RAA with LSA is extremely rare, occurring in 0.05–0.1% of the population.2 A cause of KD is an embryological abnormal regression of the primitive fourth aortic arch and ventral aortic root. Aneurysm of the KD may cause serious complications, including dissection and rupture. Three-dimensional CT is an important tool for the diagnosis and evaluation of complex vascular anomalies, and facilitates comprehension of anatomy by providing viewpoints in multiple orientations.
Acknowledgments
We are very grateful to Tsukasa Ueda in our Radiology Centre at Nippon Medical School Chiba Hokusoh Hospital for contributing to reconstruction of the image.
Footnotes
-
Contributors TI, YS and KM contributed equally to the preparation and writing of the manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ethics committee at Nippon Medical School Chiba Hokusoh Hospital.
-
Provenance and peer review Not commissioned; internally peer reviewed.