Article Text

Statistics from Altmetric.com
Introduction
Metastatic sarcomas to the heart involve the myocardium more often than the pericardium. All types of sarcomas metastasise to this organ and this occurs via the haematogenous route. Bilateral or diffuse involvement is seen in 30–35% of cases. Only in 5% of cases may endocardium or chamber cavities be involved, as was the case in our patient. The clinical signs and symptoms of metastatic cardiac neoplasms include dyspnoea, cough, chest pain, palpitations, superior vena cava syndrome, right ventricular outflow tract obstruction and pericardial effusion. Only 25 antemortem cases of metastatic osteogenic sarcoma to the heart have been diagnosed over the past 50 years.
Case report
A 38-year-old man presented with a history of osteosarcoma in the left femur 5 years prior to his recent admission. Four courses of chemotherapy had been carried out over a period of 3 years. However, on account of the poor response to therapy resulting in local recurrence, he underwent left hip disarticulation 2 years before his recent admission.
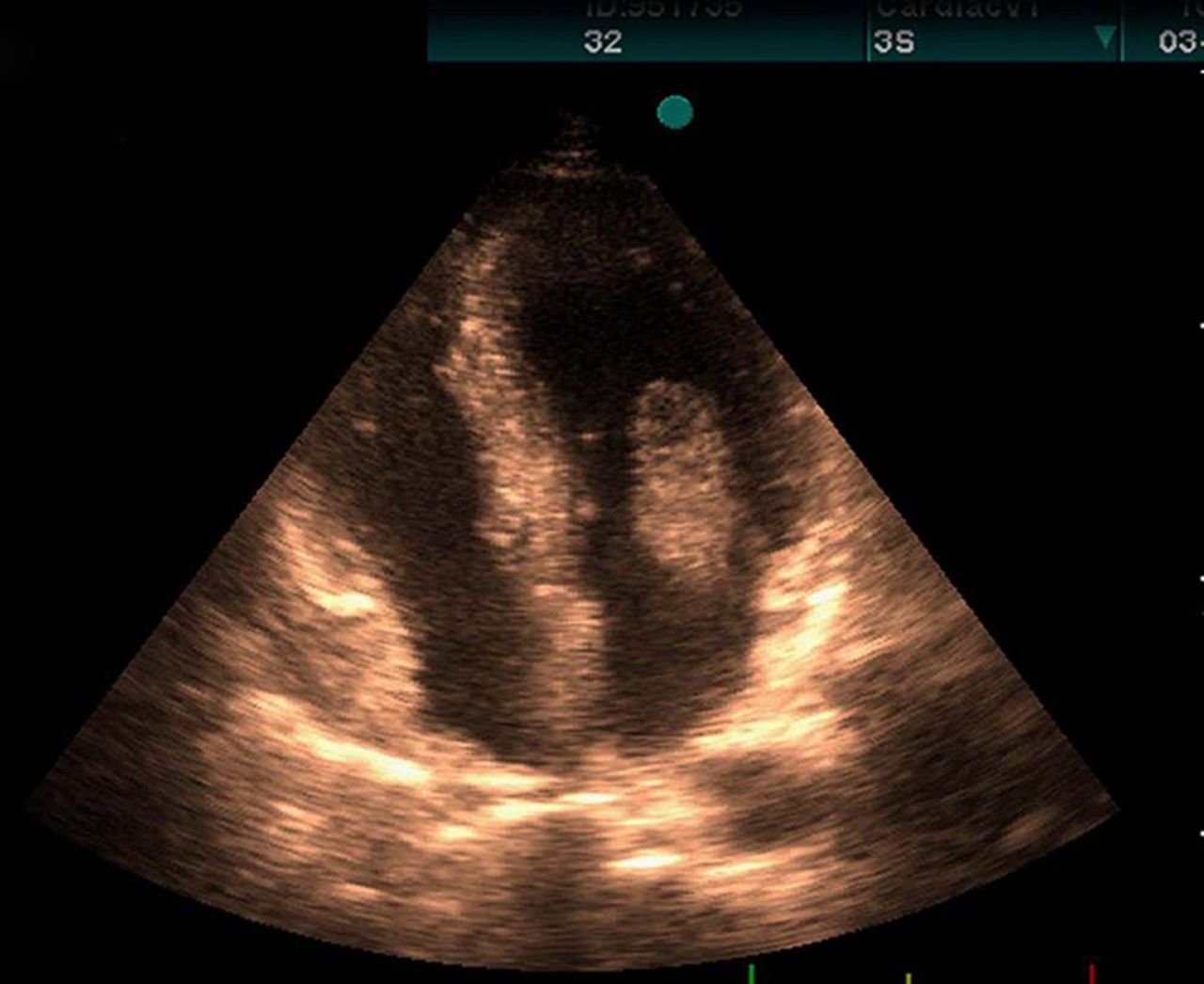
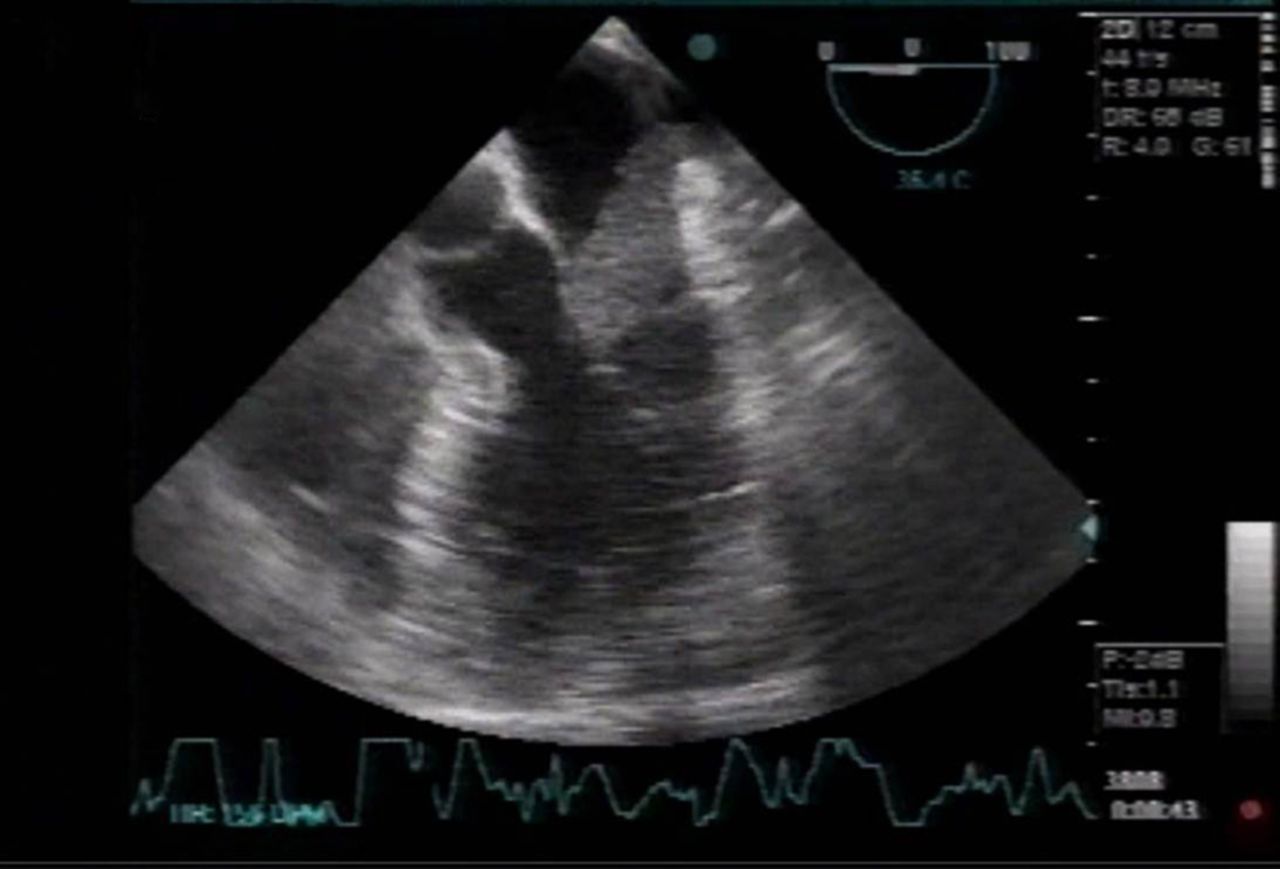
The patient had no further complaints until 5 months before his referral to us when he developed diffuse ischaemic lesions in his right leg due to popliteal artery obstruction. Both transthoracic and transesophageal echocardiographic studies were done in order to determine the precise source of his emboli, with the following findings: both ventricles had normal size and function, trivial mitral and tricuspid valves regurgitation, and normal pulmonary artery pressure. Also, a large lobulated and highly mobile mass (3.5×2.1 cm) was seen in the left atrium, which originated from the lower left pulmonary vein (figures 1 and 2, online supplementary movie 1).
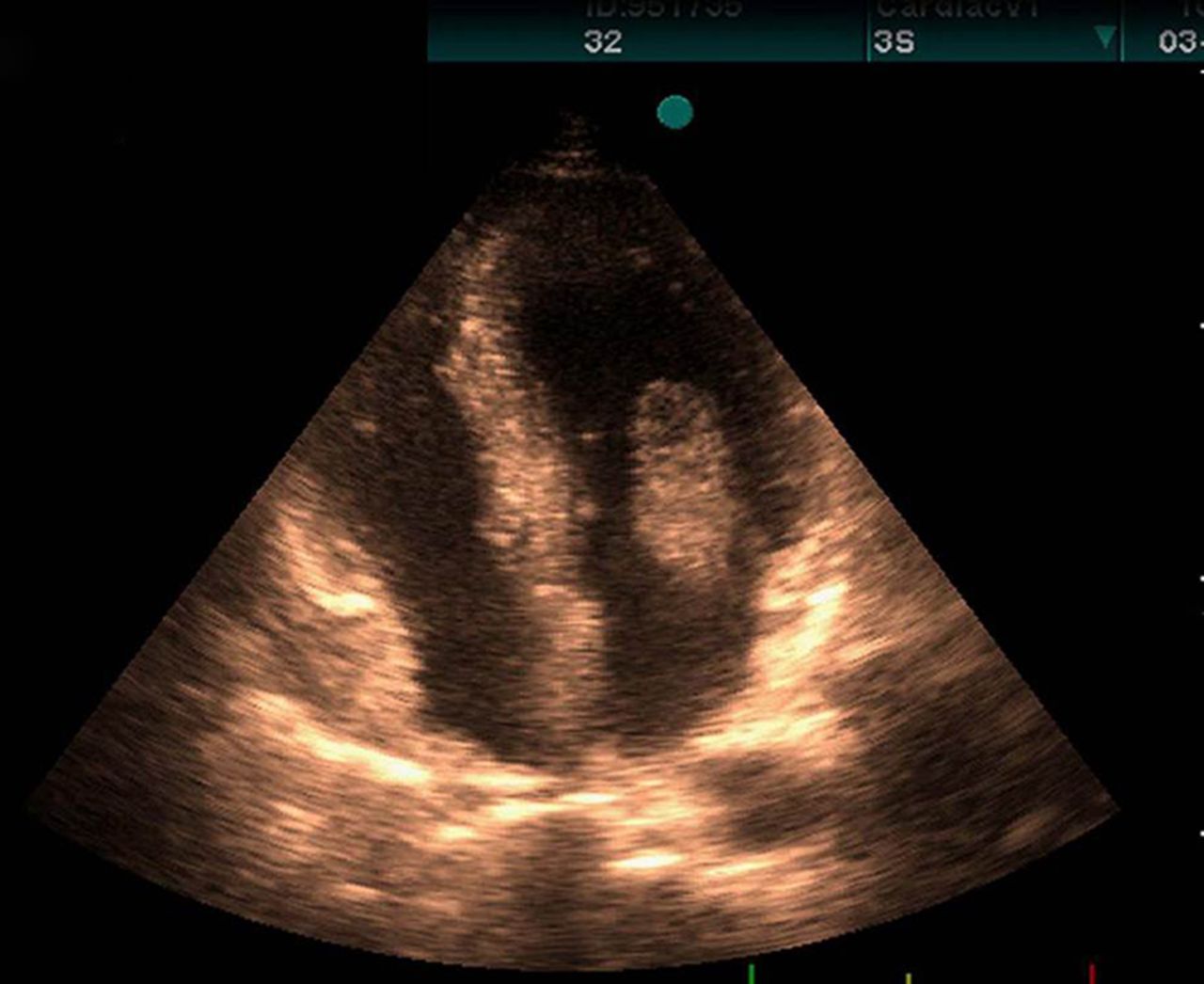
Mobile mass in left atrium that protrudes to left ventricle.
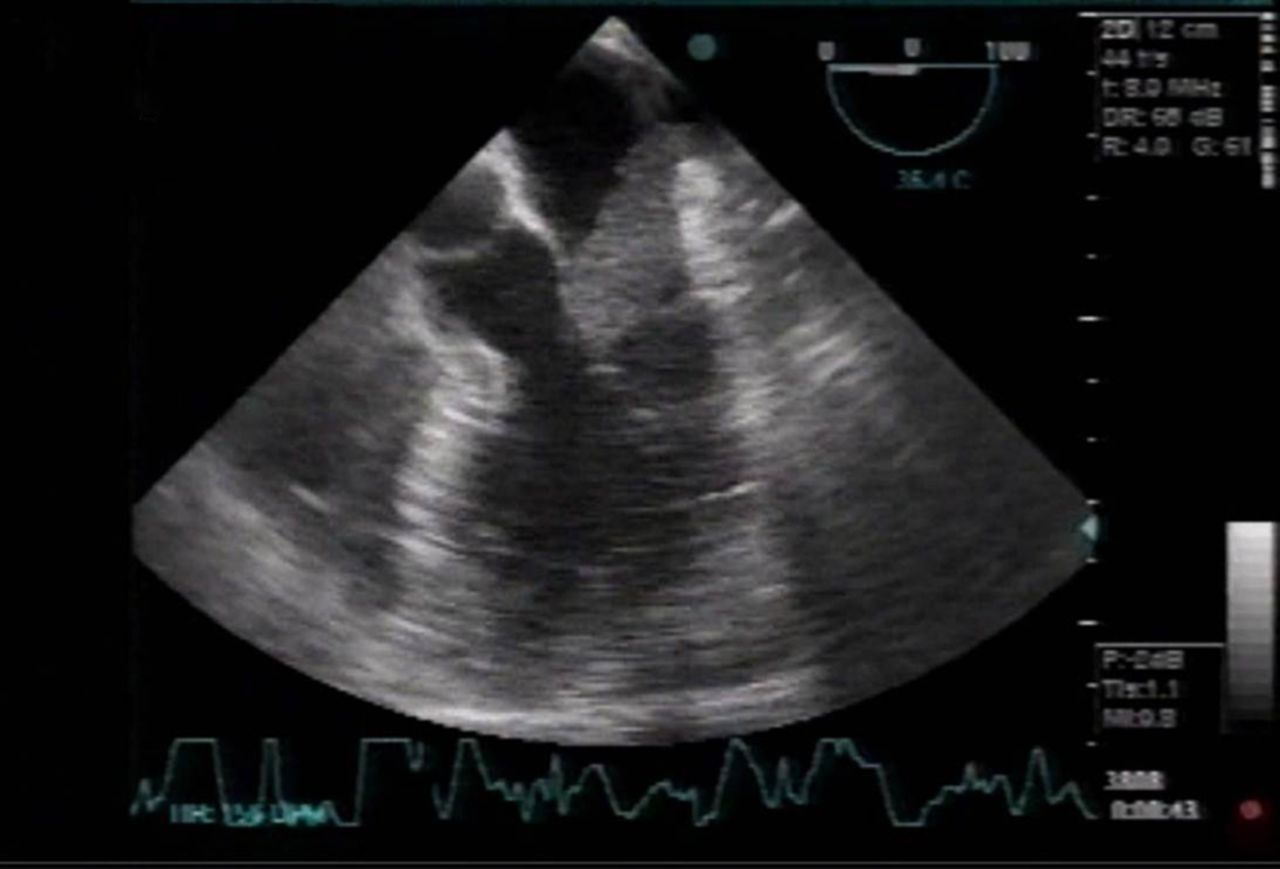
Mobile mass that originate from pulmonary vein on transesophageal echocardiogram.
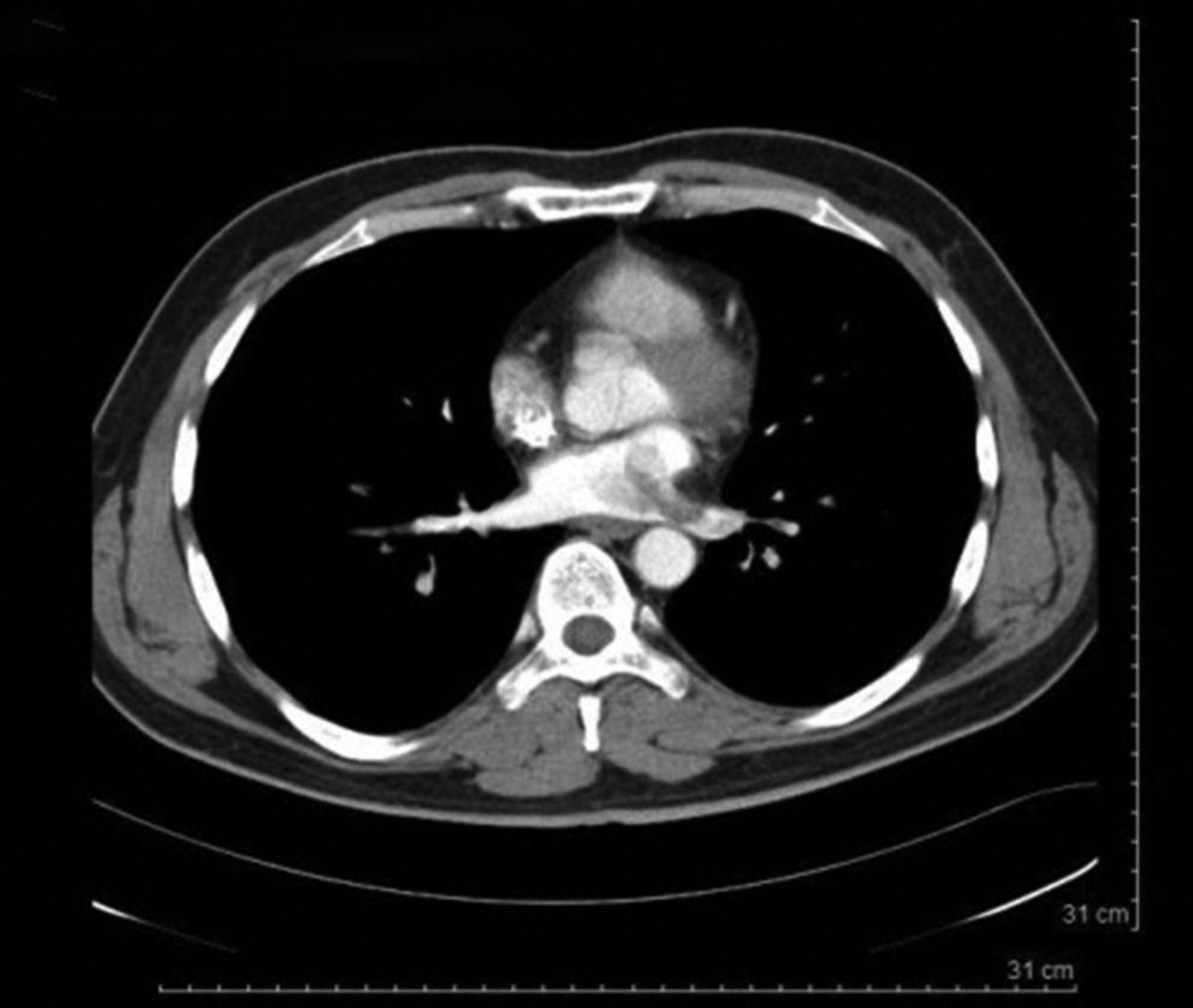
Spiral CT scan of the thorax (with and without contrast) showed evidence of a soft tissue density mass at the left atrium with extension towards the left ventricle as well as defects at the pulmonary veins, particularly at the left inferior pulmonary vein (figures 3 and 4).

Soft tissue density mass lesion at left atrium with defect at pulmonary vein.

Soft tissue density mass lesion in left atrium.
Multiple abnormal soft tissue density masses were noted at the basal segments of both lungs. The largest one was about 55 mm at left lower lobe, with foci of calcification and ossification. Also, a pulmonary nodule up to 3 mm was seen at the apical segment of the right lower lung, which was suggestive of metastasis (figure 5).

Soft tissue mass at left lower lobe.
After a month, the patient developed right-sided hemiparesis with features indicative of ischaemic lesions in the brain CT scan.
Eventually, he underwent open heart surgery in light of the fact that the left atrial mass could result in more embolic episodes in the arterial system.
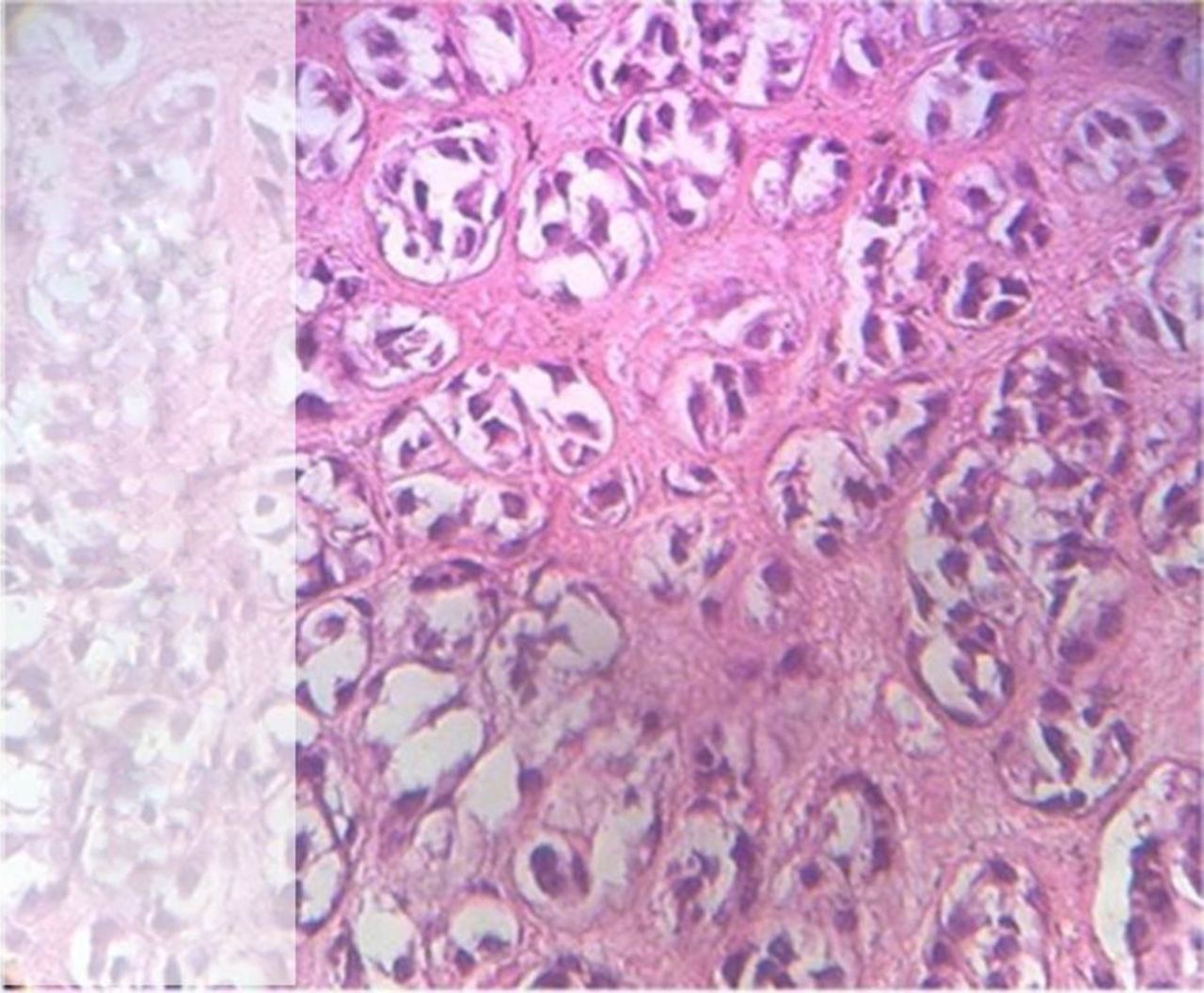
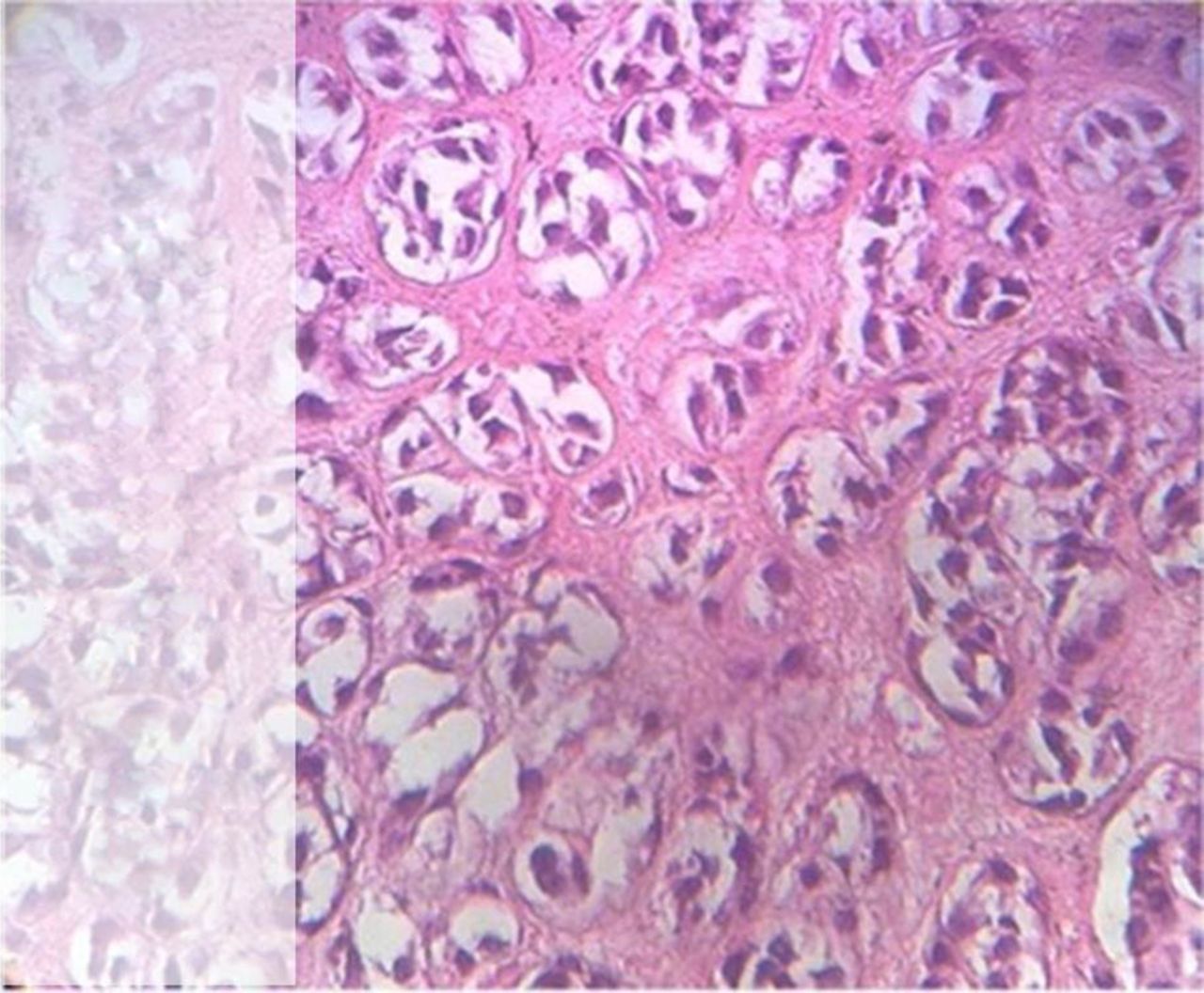
A large and fragile cauliflower-shaped creamy mass, measuring 5×4×2 cm, was excised from the left atrium and was sent to our pathology department for histopathological evaluation. The morphological findings revealed a pleomorphic round cell sarcoma with foci of haemorrhage and necrosis, consistent with metastatic osteosarcoma (figure 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pleomorphic round cell sarcoma with foci of haemorrhage and necrosis, consistent with metastatic osteosarcoma.
The postoperative course was unremarkable, and the patient was discharged from the hospital in good clinical condition and was instructed to seek further medical follow-up.
Discussion
Metastatic sarcomas to the heart are more likely to involve the myocardium than the pericardium. All types of sarcomas are known to metastasise to the heart and evidently this occurs via the haematogenous route. The right side of the heart is affected in 20–30% of cases, the left side in 10–33%, and bilateral or diffuse involvement is seen in 30–35% of cases. Only in 5% of cases are the endocardium or chamber cavities involved, as was the case in our patient. Another extremely uncommon feature that was noted in our patient was its occurrence as an isolated lesion.1
The clinical signs and symptoms of metastatic cardiac neoplasms include dyspnoea, cough, chest pain, palpitations, superior vena cava syndrome, right ventricular outflow tract obstruction and pericardial effusion.2 Only 25 antemortem cases of metastatic osteogenic sarcoma to the heart have been diagnosed over the past 50 years, whereas a prevalence as high as 20% is noted at autopsy.3
Among patients who suffer from primary or secondary malignancies to the heart, osteogenic sarcoma is unique, inasmuch as it may contain radiographically visible neoplastic bone. It is worth reiterating that it is usually large in size, and often intracavitary in location.4 In a rare instance, this tumour was found to be lodged in the pulmonary artery, and in spite of the fact that the patient lacked any symptoms, repeated surgical operations had to be carried out for its removal.5
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online video
Footnotes
-
Contributors MM: Professor of cardiology in echocardiography department of Shahid Rajaei Heart Center, the corresponding author of this paper and responsible for integrity of whole work. KM: Assistant professor of pathology and responsible for interpretation of histological samples. NG: Associate professor of cardiac surgery in Shahid Rajaei Heart Center, in charge of the operation team on the patient, and obtaining samples for our pathologist. AT and BB: Fellows of cardiology, responsible for gathering data, drafting and revising the manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The ethics committee of Rajayee Heart Center.
-
Provenance and peer review Not commissioned; internally peer reviewed.