Article Text

Statistics from Altmetric.com
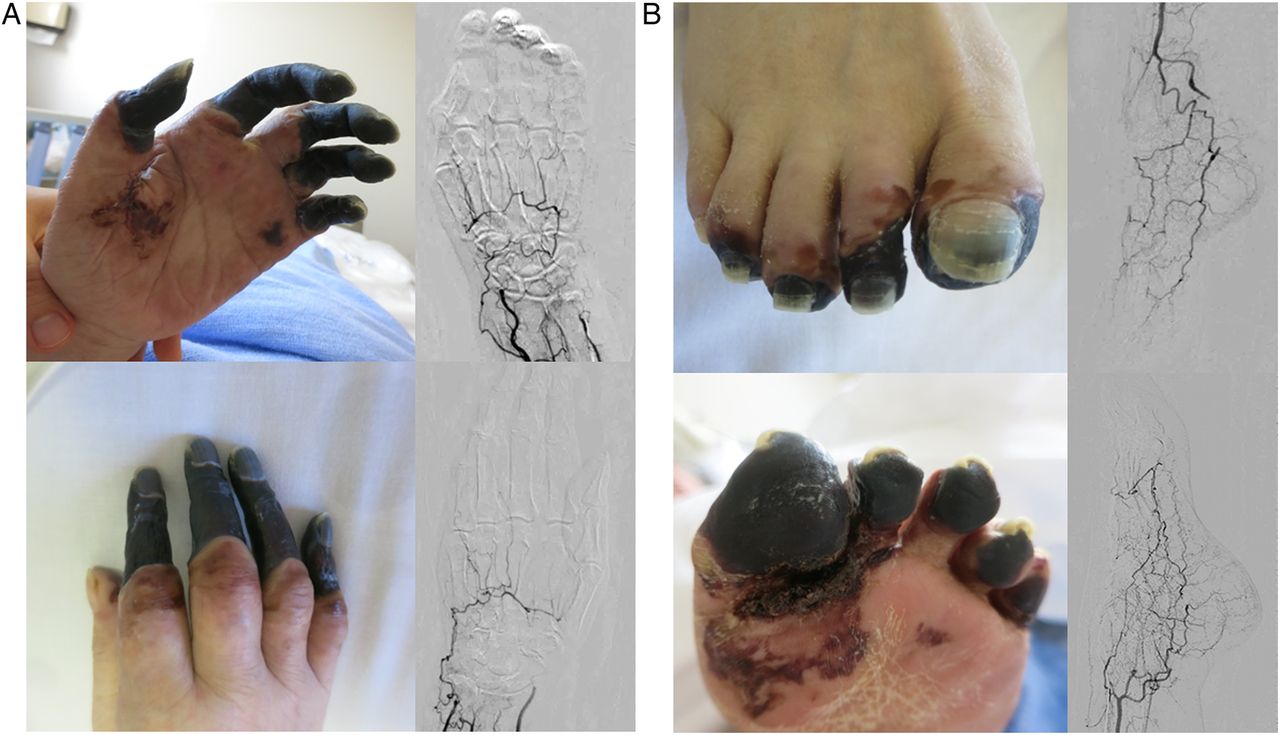
A 75-year-old woman with a history of recurrent spontaneous abortions and smoking was referred to our hospital for the treatment of symmetric peripheral gangrene in all four extremities. Her painful digital and toe gangrene developed over 2 weeks (figure 1). Her peripheral pulses were absent, and angiography revealed total occlusion of the palmar and pedal arches (figure 1). Concomitant deep vein thrombosis in the soleus vein was revealed by duplex ultrasonography. Laboratory testing showed lupus anticoagulant (LA) positive with dilute Russell’s viper venom time (5.0, normal range <1.3), activated partial thromboplastin time (20.7 s, normal range <6.3 s), and antibodies to phosphatidylserine/prothrombin complex (IgG) (38 U/mL, normal range <12 U/mL). Furthermore, the cross-mixing test showed an inhibitor (LA) pattern. Other vascular disorders were excluded, especially antineutrophil cytoplasmic antibody was negative. Given these findings, the diagnosis of antiphospholipid syndrome (APS) was made. APS was defined as the occurrence of arterial and/or venous thrombosis, including an early pregnancy morbidity, associated with persistently positive results for antiphospholipid antibodies.1 With medical treatment, including vasodilators, antiplatelet agents, and anticoagulants, her symptoms were stabilised with preservation of peripheral skin perfusion pressure.
{kind=link}
(A and B) Symmetric peripheral gangrene with angiographical evidence of the occlusions of the palmar and pedal arches.
Peripheral gangrene in four limbs can be caused by a variety of disorders, including atherosclerosis, thromboembolism, connective tissue disease, vasculitis, thrombophilia, Buerger's disease, Raynaud's disease, drug-induced vasospasm, blood dyscrasias, myeloproliferative disorders and sepsis.2 We emphasise the need for an increasing awareness of APS even in elderly patients with symmetric peripheral gangrene for an improved patient care in the field of cardiovascular medicine.
Footnotes
Contributors All the authors were involved in the clinical management of the patient. MS drafted and MI and OK revised the manuscript.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.